
Abstract
Atherosclerosis and venous thromboembolism (VTE) share common risk factors. We set to assess the strength of the association between atherosclerosis risk factors and disease manifestation, and VTE, in patients with coronary artery disease undergoing percutaneous coronary intervention. We pooled data from 6 global randomized controlled trials assessing coronary stenting (ENDEAVOR and SIRIUS programs), developed separate risk scores to predict major adverse cardiac and cerebrovascular events (MACCEs: cardiac death, myocardial infarction, and stroke) and VTE, and compared their performance. The 5-year rates of MACCE and VTE were 10.8% and 2.04%, respectively. Selected predictors for MACCE performed equally well in predicting VTE (area under the receiver–operating characteristic curve [AUC] 0.651 vs 0.672), and selected predictors for VTE performed equally well in predicting MACCE (AUC 0.699 vs 0.620). Ejection fraction and age were associated with both MACCE and VTE. These findings support the concept of overlapping pathophysiology of VTE and atherothrombosis.
Introduction
Atherosclerosis and venous thromboembolism (VTE) have been considered distinct in their pathophysiology and epidemiology. However, VTE and atherosclerosis share overlapping risk factors and pathophysiology. 1 Patients with unprovoked VTE have a higher atherosclerotic disease burden and are at increased risk of atherothrombotic events. 1,2
The objective of this analysis was to assess the strength of the association between cardiovascular risk factors and atherothrombotic as well as VTE events in a cohort of patients with symptomatic coronary arterial disease undergoing nonemergent percutaneous coronary intervention (PCI). Specifically, we sought to assess whether a risk assessment tool developed to predict atherothrombotic events can be applied to predict incident VTE and whether a VTE-specific risk score can be applied to predict atherothrombotic events. We also aimed to assess whether the risk factors associated with VTE are the same as those associated with atherothrombotic events and whether the strengths of the association are similar.
Materials and Methods
The authors sought and were granted access to deidentified patient-level data from the ENDEAVOR II, ENDEAVOR III, and ENDEAVOR IV trials (Medtronic, Inc, Santa Rosa, California). Details of study design and results for each study were previously reported. 3 –5 These were multicenter, prospective, double-blinded randomized controlled trials evaluating the Endeavor zotarolimus-eluting stent versus control (bare-metal or drug-eluting stents) in which 5-year follow-up data are available. These data served to develop the risk prediction models. Additionally, data from 3 multicenter, prospective, double-blinded randomized controlled trials evaluating the Cypher sirolimus-eluting stent (Cordis, Miami Lakes, Florida) versus bare-metal stents (SIRIUS, E-SIRIUS, and C-SIRIUS) 6 –8 were used to verify the predictive strength of this model for predicting atherosclerosis-related outcomes.
Study Population
Inclusion and exclusion criteria were similar in the trials assessed. Patients were required to have clinical evidence of ischemic coronary disease or a positive functional study. Patients presenting with ST-segment elevation myocardial infarction (MI) were excluded. Angiographic requirements were the presence of a single de novo native coronary lesion with a diameter stenosis of at least 50% but <100% by visual estimate. Reference vessel diameter ranged between 2.5 and 3.5 mm and lesion length ranged between 14 and 32 mm. Patient demographic, clinical, and angiographic baseline characteristics were evaluated. We calculated a simplified atherosclerotic burden index per patient as a sum of the modified American College of Cardiology/American Heart Association lesion classification 9 , where a class A lesion contributes 1, a class B1 lesion contributes 2, a class B2 lesion contributes 3, and a class C lesion contributes 4.
Outcomes
Outcomes were available for 5-year follow-up. Atherothrombotic outcomes for both the ENDEAVOR and the SIRIUS programs were assessed as the incidence of major adverse cardiac and cerebrovascular events (MACCEs), a composite of cardiovascular death, stroke, and MI events. The VTE events were collected only from the ENDEAVOR trials for which adverse event listings were available for evaluation. Additionally, we examined the clinical narratives of adjudicated cardiac and vascular deaths, in search of VTE events leading to death, which were not captured as the primary safety event under the safety listings. Cardiac death was defined as any death due to a proximate cardiac cause, cardiac procedure-related deaths, including those related to concomitant treatment, or any death of unknown cause. Vascular death was defined as death caused by noncoronary vascular causes, such as cerebrovascular disease, pulmonary embolism, ruptured aortic aneurysm, dissecting aneurysm, or other vascular diseases. Finally, all suspected VTE events were categorized according to the level of evidence supporting the diagnosis. Definite events were confirmed by imaging modalities, pathologic confirmation, or site-reported diagnosis. Probable events were events in which the clinical impression of VTE by the treating physicians was reflected in documentation or by treatment modalities, or in suspected PE events for which the ventilation–perfusion lung scan was intermediate in probability, and where other diagnostic modalities did not exclude the diagnosis and in which no obvious alternative diagnosis was evident. Definite and probable events were included in the analysis, while all other suspected events were excluded.
Statistical Analysis
Using logistic regression, we developed 2 risk scores on the development cohort (ENDEAVOR trials)—one for predicting MACCE and the other for predicting VTE. The performance of the risk score for MACCE was confirmed on the validation cohort (SIRIUS trials). We assessed the performance of the risk score for MACCE for predicting VTE and compared it to the performance of the risk score for VTE. We also assessed the performance of the risk score for VTE for predicting MACCE. Area under the receiver–operating characteristic curve (AUC) analyses were utilized as standard metrics of model discrimination. To test the strength of association between VTE and atherothrombotic risk factors, we used a competing risk model with VTE and MACCE as the 2 competing outcomes. Tests of differential effect were conducted for all variables found significantly associated with either outcome. A P value of <.05 was considered statistically significant. The statistical analyses were performed with SAS version 9.2 (SAS Institute Inc, Cary, North Carolina).
Results
The ENDEAVOR and SIRIUS pooled cohorts (Table 1) contributed 2975 and 1695 patients undergoing PCI, respectively. Clinical follow-up through 5 years was complete for 82.8% of the patients in both cohorts. There was a small but statistically significant difference in atherosclerotic burden between the ENDEAVOR and the SIRIUS cohorts (2.9 ± 0.8 and 2.7 ± 0.9, respectively, P < .001; Table 2).
Characteristics of Included Studies.
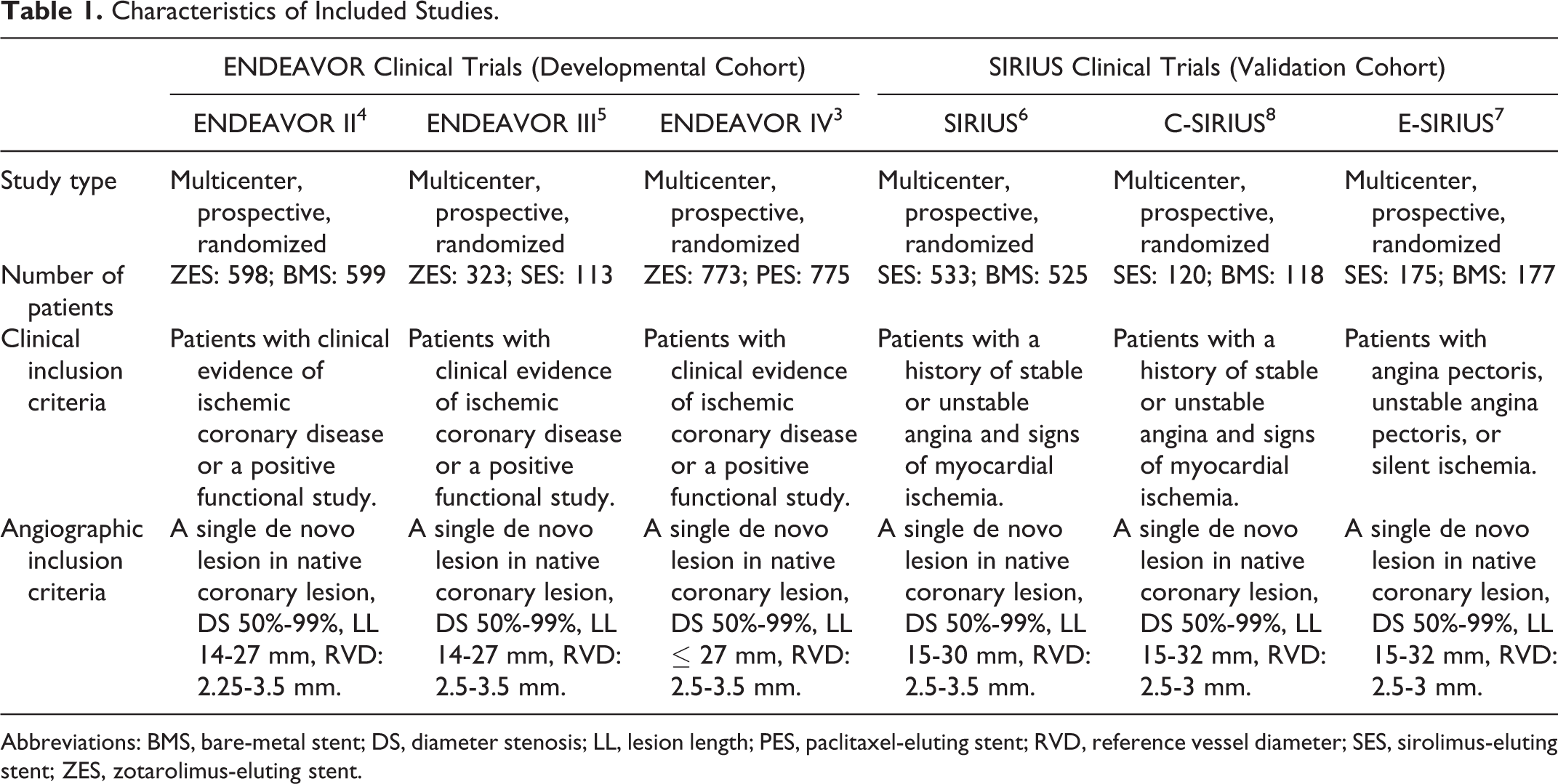
Abbreviations: BMS, bare-metal stent; DS, diameter stenosis; LL, lesion length; PES, paclitaxel-eluting stent; RVD, reference vessel diameter; SES, sirolimus-eluting stent; ZES, zotarolimus-eluting stent.
Baseline Clinical and Angiographic Characteristics.
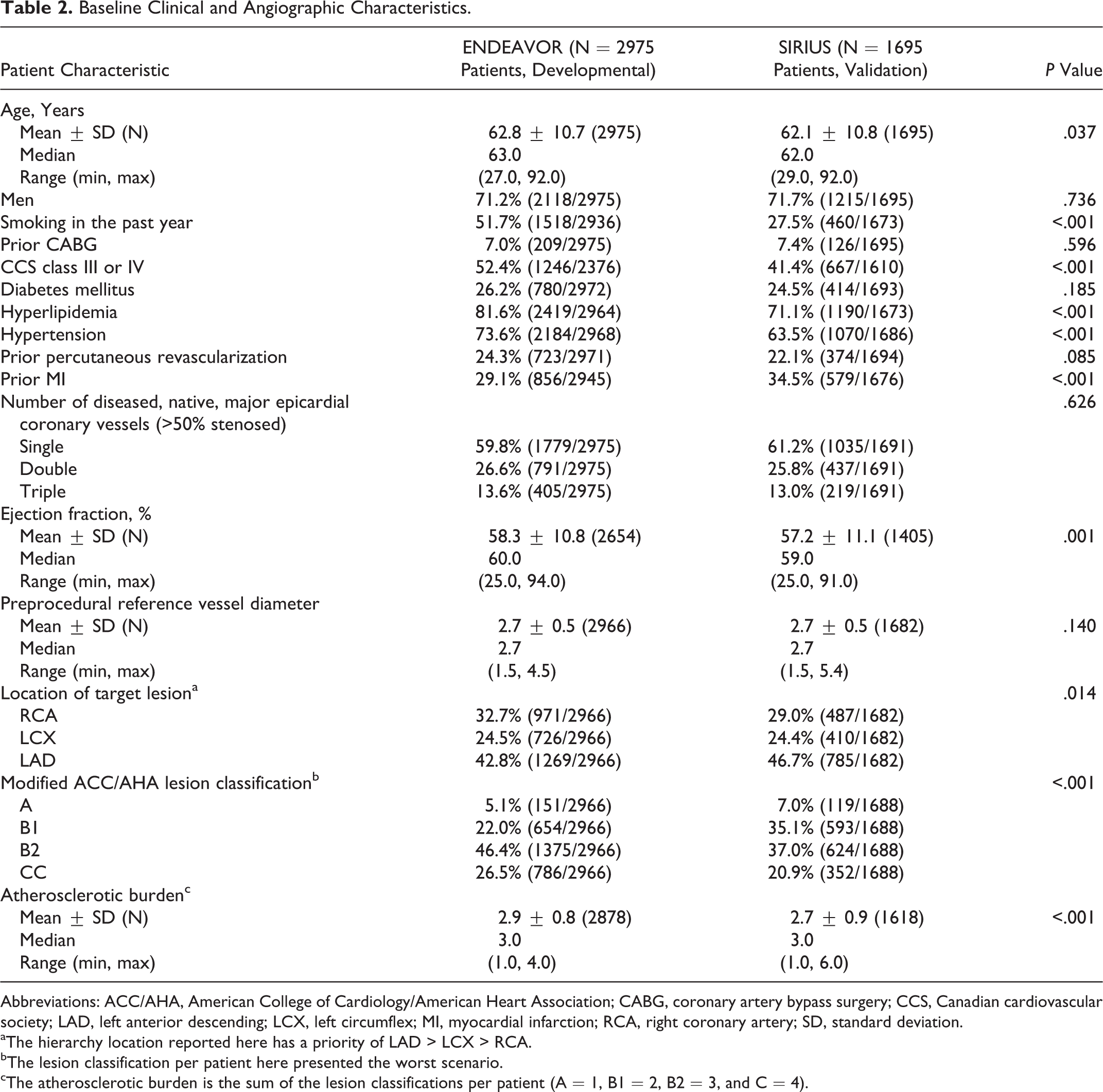
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; CABG, coronary artery bypass surgery; CCS, Canadian cardiovascular society; LAD, left anterior descending; LCX, left circumflex; MI, myocardial infarction; RCA, right coronary artery; SD, standard deviation.
aThe hierarchy location reported here has a priority of LAD > LCX > RCA.
bThe lesion classification per patient here presented the worst scenario.
cThe atherosclerotic burden is the sum of the lesion classifications per patient (A = 1, B1 = 2, B2 = 3, and C = 4).
At 5 years, 10.8% (305 of 2812) of the patients in the ENDEAVOR cohort and 16.1% (228 of 1418) of the patients in the SIRIUS cohort had at least 1 MACCE (Kaplan-Meier estimates 10.6% and 14.2%, respectively). In the ENDEAVOR cohort, 2.04% (55 of 2702) had VTE.
Increased age, hypertension, decreased left ventricular ejection fraction (LVEF), prior MI, absence of hyperlipidemia, increased lesion class, and number of diseased vessels were significant predictors for MACCE (AUC 0.651) in the development cohort (Table 3). The AUC for this model in the validation cohort was similar at 0.647. Its AUC to predict VTE in the ENDEAVOR cohort was 0.672. Increased age, lower Canadian Cardiovascular Society functional class, decreased ejection fraction, and female gender were significant predictors for VTE (AUC 0.699) in the development cohort (Table 3). The AUC for predicting MACCE with the selected predictors for VTE was 0.620 (Figure 1).
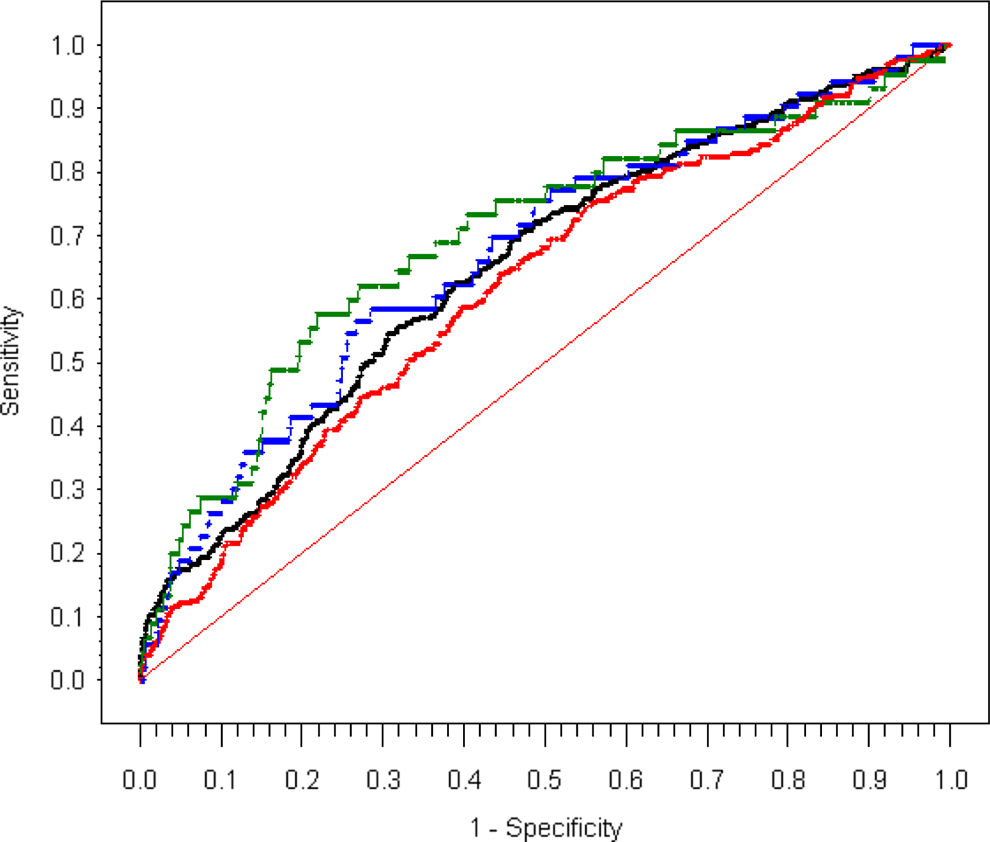
Predicting MACCE and VTE—AUC for predicting MACCE and VTE with selected predictors for MACCE or VTE. Red is ROC for MACCE using predictors selected from regression on VTE, AUC = 0.620; green is ROC for VTE using predictors selected from regression on VTE, AUC = 0.699; black is ROC for MACCE using predictors selected from regression on MACCE, AUC = 0.651; and blue is ROC for VTE using predictors selected from regression on MACCE, AUC = 0.672. AUC indicates area under the ROC curve; MACCE, major adverse cardiac and cerebrovascular event; ROC, receiver–operating characteristic; VTE venous thromboembolism.
Predictors for MACCE and VTE in the Developmental Cohort.a
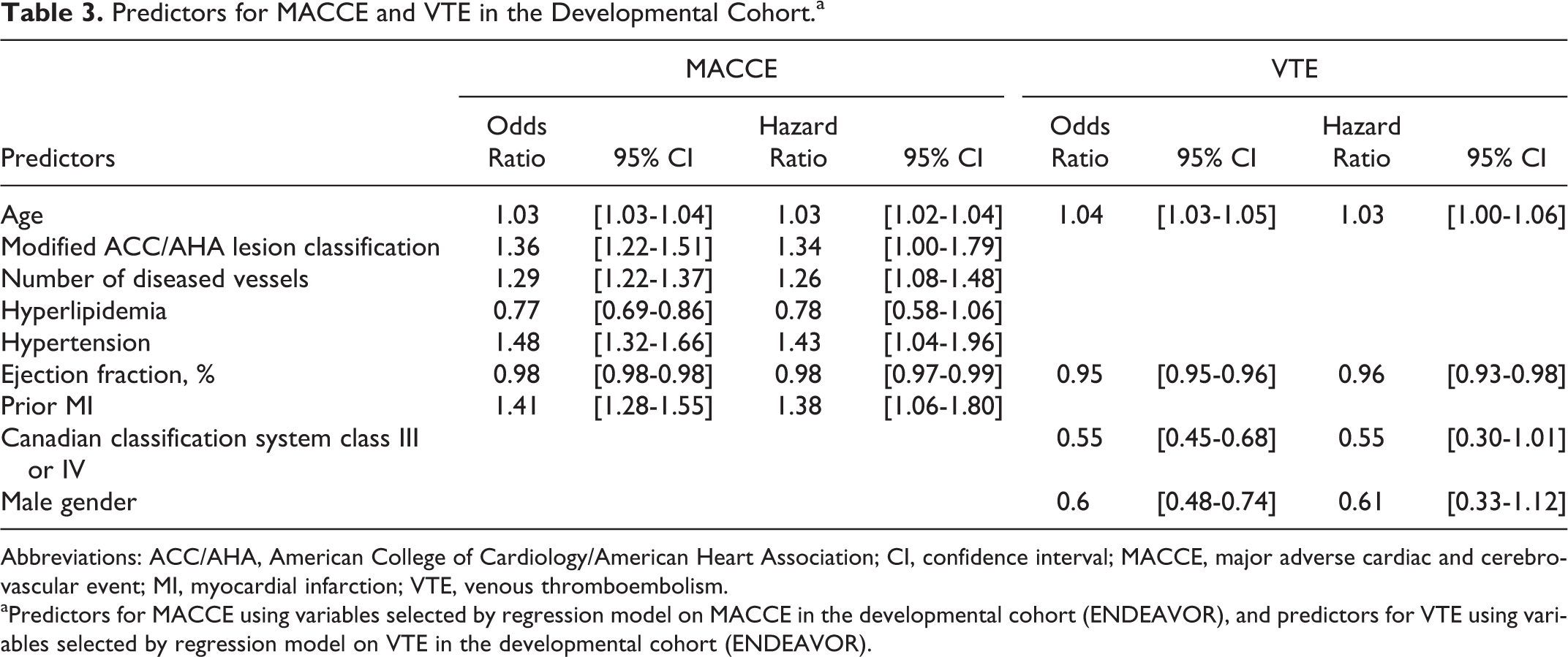
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; CI, confidence interval; MACCE, major adverse cardiac and cerebrovascular event; MI, myocardial infarction; VTE, venous thromboembolism.
aPredictors for MACCE using variables selected by regression model on MACCE in the developmental cohort (ENDEAVOR), and predictors for VTE using variables selected by regression model on VTE in the developmental cohort (ENDEAVOR).
The competing risk model showed decreased LVEF and increased age to be statistically significantly associated with both MACCE and VTE (for 1 year of age: odds ratio [OR] for MACCE 1.028 [95% confidence interval, CI, 1.012-1.043] and OR for VTE 1.042 [95% CI 1.009-1.077]; for 1 unit of LVEF: OR for MACCE 1.024 [95% CI 1.009-1.038] and OR for VTE 1.053 [95% CI 1.021-1.086]).
Discussion
We found that in this patient population, predictors for MACCE can predict VTE, and selected predictors for VTE can predict MACCE. The LVEF and increased age were risk factors contributing to both atheroembolic and VTE among patients undergoing PCI.
Prandoni et al found that patients without symptomatic atherosclerosis who had an unprovoked lower extremity DVT had a significantly higher rate of carotid artery plaque as detected by ultrasound than patients with provoked DVT or normal controls. 10 Hong et al found higher coronary artery calcium scores in patients with VTE compared to controls. 11 Becattini et al performed a systematic review and meta-analysis on arterial cardiovascular events after VTE and found that the risk of arterial cardiovascular events was higher in patients with unprovoked VTE compared with controls (incidence rate ratio [IRR] 1.87; 95% CI 1.32-2.65) or to patients with provoked VTE (IRR 1.86, 95% CI 1.19-2.89). 12
To the best of our knowledge, there are no established risk assessment tools to predict VTE in patients undergoing PCI. There are many risk assessments tools that address early and late outcomes after PCI (Table 4). These were not tested for their ability to predict a composite of death, MI, and stroke at 5 years. A recent analysis assessed the ability to predict a 1-year composite of death, MI, and target lesion revascularization. 13 The anatomical Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) risk score (SRS) score, the clinical ACEF (age, creatinine, ejection fraction), modified ACEF and NCDR (National Cardiovascular Data Registry) scores, and the combined anatomical and clinical SYNTAX score (CSS) and New York State Risk Score (NYSRS) scores were found to have AUC ranging from 0.53 (NCDR) to 0.63 (SRS). 13 The CSS, SRS ACEF, and modified ACEF scores were also assessed for their ability to predict a 5-year composite of death, stroke, revascularization, and MI after PCI, with AUCs ranging from 0.57 to 0.62, respectively. 14
Risk Scores to Predict Cardiovascular Outcomes After Percutaneous Intervention.
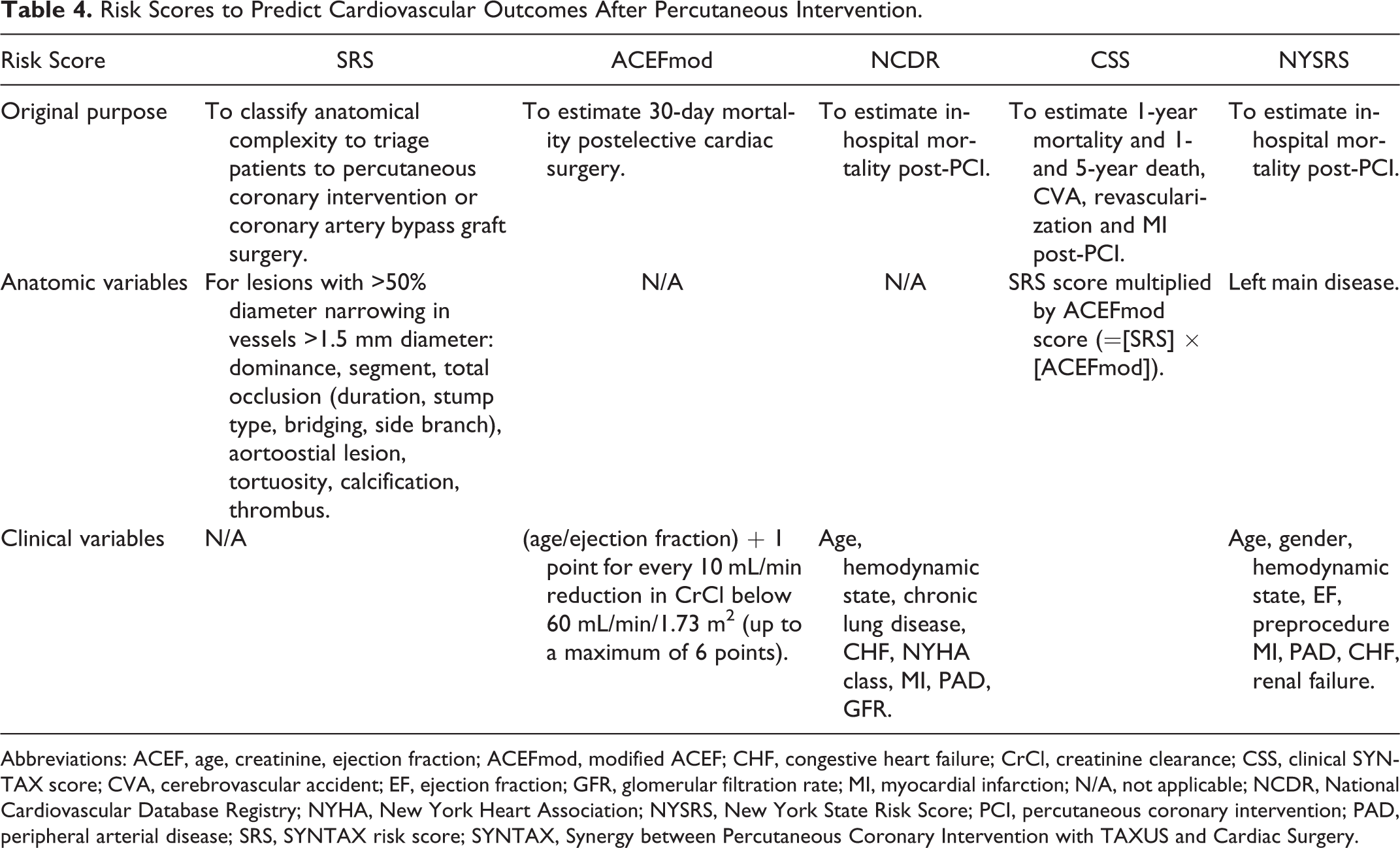
Abbreviations: ACEF, age, creatinine, ejection fraction; ACEFmod, modified ACEF; CHF, congestive heart failure; CrCl, creatinine clearance; CSS, clinical SYNTAX score; CVA, cerebrovascular accident; EF, ejection fraction; GFR, glomerular filtration rate; MI, myocardial infarction; N/A, not applicable; NCDR, National Cardiovascular Database Registry; NYHA, New York Heart Association; NYSRS, New York State Risk Score; PCI, percutaneous coronary intervention; PAD, peripheral arterial disease; SRS, SYNTAX risk score; SYNTAX, Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery.
The risk scoring models in the current analysis possess similar discrimination capabilities as the risk scores available in the literature. The risk scoring models support our growing understanding of shared risk factors for atherothrombotic events and VTE. We have shown that these risk scoring models, when based on predictors for MACCE or VTE, can similarly predict either MACCE or VTE. This suggests that the classic atherosclerosis risk factors play an interchangeable role for predicting arterial and venous events, implying a common underlying pathophysiology. Interestingly, aspirin has been shown to be beneficial in reducing the incidence of VTE in high-risk patients, 15 and recently it was shown to be beneficial in reducing the risk of recurrent VTE events when given to patients with unprovoked VTE who had discontinued anticoagulant treatment. 16,17
Limitations
Our study is retrospective and assessment of VTE events was not prespecified. Given the low number of VTE events, the study was not powered to detect potential contributions from additional risk factors. Our study includes only baseline characteristics classically associated with atherosclerosis and PCI outcomes, as collected by the original investigational plan, while many of the risk factors that have been well documented to be powerful predictors of VTE were not available for the analysis or served as exclusion criteria (eg, malignancy). The models in our study have limited ability to detect patients at increased risk of MACCE or VTE based on their AUC ranging from 0.57 to 0.62. However, the discrimination capability of our MACCE model is largely similar to those of other models presented in the literature. Finally, in this study we have pooled data from individual trials in the aim of assessing an outcome not defined in the original aims of the trials. We have used this method to increase the power to detect predictors for VTE, a rare occurrence in our cohort. Furthermore, the SIRIUS data did not include VTE events, thus the external validation of the VTE model could not be performed in the same rigorous manner as the MACCE model. In that respect, this study should only be regarded as hypothesis generating. Additional prospective studies are needed to investigate the association between atherosclerosis and venous thrombosis.
In a cohort of patients undergoing PCI, the predictors for a composite of cardiac death, MI, or stroke and those for VTE have similar accuracy in predicting both these clinical manifestations. These findings suggest that athero- and venous thromboembolic diseases are part of a panvascular syndrome that shares common pathways. Decreased LVEF and increased age are significantly and similarly associated with 5-year MACCE and VTE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.