
Abstract
Background:
Current guidelines recommend risk-based use of prophylaxis for preventing medical inpatients from venous thromboembolism (VTE). Little is known about the current prescription practice, and even less whether differences between subspecialists like cardiologists, usually treating patients with thrombotic or thromboembolic diseases, and gastroenterologists, treating more patients with gastrointestinal bleeding complications, exist.
Methods:
We performed a retrospective chart review of patients on cardiology and gastroenterology wards of our university hospital. Patients with a clear indication for anticoagulation and contraindication against antithrombotic treatment were excluded. A total of 450 patients per specialty were included. Quantitative risk assessment models were used to determine the risk of a VTE (Padua Prediction Score (PPS), IMPROVE Score) and bleeding (IMPROVE-Bleeding and HAS-BLED Score).
Results:
The overall rate of VTE prophylaxis was high in both patient populations. Significant more low-risk cardiology compared to gastroenterology patients received drug-based prophylaxis. Furthermore, crucial discrepancies were found in the way individual patients would be classified based on PPS and IMPROVE Score. Finally, not the risk category but the length of hospital stay was best at predicting which patient received prophylaxis.
Introduction
Studies show an increasing rate of pulmonary embolism (PE) mortality in middle-aged patients in North America with cancer, respiratory diseases, and infections as contributing factors of fatal PE. 1 The incidence of venous thromboembolism (VTE) events is higher in high-income countries like Sweden and Canada compared to low-income countries such as Pakistan and India. 2 In Germany the incidence of PE increased from 85/100.000 in 2005 to 109/100.000 in 2015. 3 Almost half of venous thromboembolic events are considered to be hospital acquired. 4 Therefore, prescribing venous thromboembolism (VTE) prophylactic treatment to inpatients remains to be an important health task. Prophylactic treatment with low molecular weight heparin (LMWH) can substantially reduce VTE risk for inpatients; however, it is also associated with side effects such as acute bleeding or heparin-induced thrombocytopenia (HIT). 5,6
In a critical evidence-based analysis of international guidelines, 7 the authors assumed that most inpatients have a clinical VTE risk that corresponds to or is even lower than the bleeding risk caused by LMWH. For that reason, it is important to assess the individual VTE risk of each patient to avoid possible side effects from overtreatment with LMWH. Accordingly, current German and international guidelines do not recommend a universal prophylactic treatment with LMWH, but rather prophylactic treatment based on a classification of patients into low, medium, and high-risk for VTE. 8,9
Although Greene et. al (2016) note that due to the lower incidence of VTE in nonsurgical patient population, the usefulness of the existing RAM may be limited. 10 PPS and IMPROVE Score still are the most widely recommended risk assessment models to evaluate the indication for drug-based VTE-prophylaxis in medical inpatients. The IMPROVE Score was externally validated in a large cohort of 247.241 patients in the VTE-VALOURR study 11 as well by Rosenberg et. al (2014) in a cohort of 19.217 patients. 12 While Germini et. al (2016) show that the incidence of VTE could significantly be decreased if the prescription of VTE prophylaxis was guided by the PPS. 13
The first aim of this study is to evaluate the current prescription habits at our tertiary care hospital for potential signs of overtreatment more than 10 years after ENDORSE, a multinational cross-sectional study published in 2008, showed possible indication of overtreatment with LMWH, with Germany taking the first place in prescribing prophylactic treatment. 14 The second is to investigate whether the prescription is based on patients’ risk for developing VTE by using the Padua Prediction Score (PPS) and IMPROVE Score. 15,16 The third is to examine whether internists subspecialization could influence prescription habits. ENDORSE did not discriminate between prescription habits in different subspecialties: While cardiologists usually treat patients with thrombotic or thromboembolic diseases, gastroenterologists see more patients with gastrointestinal bleeding complications. Thus, we hypothesized that the prescription of VTE-prophylaxis will be influenced by the treating physicians’ field of specialization.
Methods
We performed a retrospective chart review of patients treated on internal medicine wards of our university hospital during the period from August 2018 to July 2019. Clinical data were extracted from electronic patient health records. Validated risk assessment models were used to evaluate patients individual risk for thrombotic events. We correlated patients’ VTE-risk with the likelihood of receiving drug-based VTE prophylaxis e.g. with LMWH or unfractionated heparin. The patient’s clinical data were also used to assess their risk of bleeding events. This study was performed following national and international law as well as ethical standards and was approved by the ethics committee of the University of Freiburg (number 95/20).
Study Population
A total of 1917 consecutive inpatients who had a hospital stay between August 2018 and July 2019 were screened. The patient collective included patients from 3 cardiology and 3 gastroenterology wards of our university hospital. Exclusion criteria were mainly based on the criteria used in the IMPROVE and PPS studies. 15,17 We excluded patients who were already anticoagulated for reasons like atrial fibrillation, a past thrombotic event (e.g. pulmonary embolism or deep vein thrombosis), or acute myocardial infarction. Patients with clear indications against prophylactic treatment with LMWH such as acute bleeding or HIT were also excluded. Furthermore, patients with a shorter hospital stay of < 48 hours, and patients with missing clinical data for assessment of the VTE-risk were excluded. For the flow diagrams of the study population see Figure 1.

Flow diagrams of study population. Flow diagrams of cardiology (left) and gastroenterology (right) patients. Patients were included and excluded according to predefined criteria. All included patients were stratified according to their Padua Prediction Score (PPS) and IMPROVE Score. PE indicates pulmonary embolism; HIT, heparin induced thrombocytopenia; LMWH, low molecular-weight heparin.
Risk Stratification
Risk stratification for the development of thrombotic events during the hospital stay was done by using the PPS and the IMPROVE Score. The PPS is a modification of the Kucher model and consists of 11 VTE risk factors, which are assigned 1 to 3 points depending on their impact on increasing VTE risk (
Data Analysis
We used a logistic regression analysis to answer the question of whether the prescription of VTE prophylaxis correlates with increasing VTE risk. For both VTE risk scores receiver operating characteristic (ROC) curves were created and the area under the curve (AUC) as well as the corresponding 95% confidence intervals (CI) were calculated. To compare different groups in demographic characteristics and clinical characteristics, categorical variables were evaluated by using the χ2 test. For the numerical variables, we used a traditional unpaired t-test. All statistical tests were 2-sided and P = < .05 was considered statistically significant. P-values and 95% CI were not adjusted for multiple comparisons and inferences drawn from them may not be reproducible. Calculations for the logistic regression analysis and χ2 test were performed by using the program Prism 8 (version 8.4.3), and calculation of unpaired t-test was performed by using R-statistics (version 4.0.3).
Results
Patient Characteristics
To include 450 cardiology and 450 gastroenterology inpatients for this study a total of 1917 patients had to be screened (Figure 1). Exclusion criteria were met by 678 cardiology (Figure 1A) and 339 gastroenterology patients (Figure 1B). The main reason for exclusion was current anticoagulation due to atrial fibrillation for cardiology (n = 393, Figure 1A) and treatment for acute bleeding for gastroenterology patients (n = 139, Figure 1B). Supplemental Table 2 reports the gastroenterology and cardiology patients’ demographic and clinical characteristics. While
PPS and IMPROVE Score Distribution
Figure 2 shows the correlation between PPS and IMPROVE Score with the likelihood of receiving drug-based VTE prophylaxis. The 450 cardiology patients stratified by PPS (Figure 2A) and IMPROVE Score (Figure 2B) reached score points from 0 to 10 and from 0 to 7, respectively. The rate of VTE prophylaxis rose with increasing score values and all cardiology patients with a PPS of ≥ 7 or an IMPROVE Score of 5 received VTE prophylaxis. Like their cardiology counterparts, all gastroenterology patients had PPS between 0 and 10 (Figure 2C) and IMPROVE Scores between 0 and 7 (Figure 2D). With increasing score values, the rate of VTE prophylaxis tended to increase for both scores, but even at very high PPS and IMPROVE Score values not all gastroenterology patients received prophylaxis.

Received VTE prophylaxis based on PPS or IMPROVE Score. Patients were stratified by their risk for VTE based on their PPS or IMPROVE Score (x-achis) and compared to the percentage of patients receiving VTE prophylaxis (y-achis). The score value as well as the number of patients in each group are shown. A, Cardiology patients stratified by PPS, (B) cardiology patients stratified by IMPROVE Score, (C) gastroenterology patients stratified by PPS and (D) gastroenterology patients stratified IMPROVE Score. PPS indicates Padua Prediction Score; SD, standard deviation.
In total 85.33% cardiology and 69.33% of gastroenterology patients received drug-based VTE-prophylaxis. In both patient groups, mainly LMWH in high-risk dose (e.g. 4000 I.E. Enoxaparin) were prescribed. Of all prescriptions, 91.15% of cardiology and 87.18% of gastroenterology patients were prescribed high-risk dose equivalents of LMWH with no statistically significant difference between the 2 specialties (P = .0914).
VTE risk groups
In Figure 3 patients were divided into 3 groups (low, medium, and high-risk for VTE) and interrelated with the likelihood of receiving drug-based VTE prophylaxis.
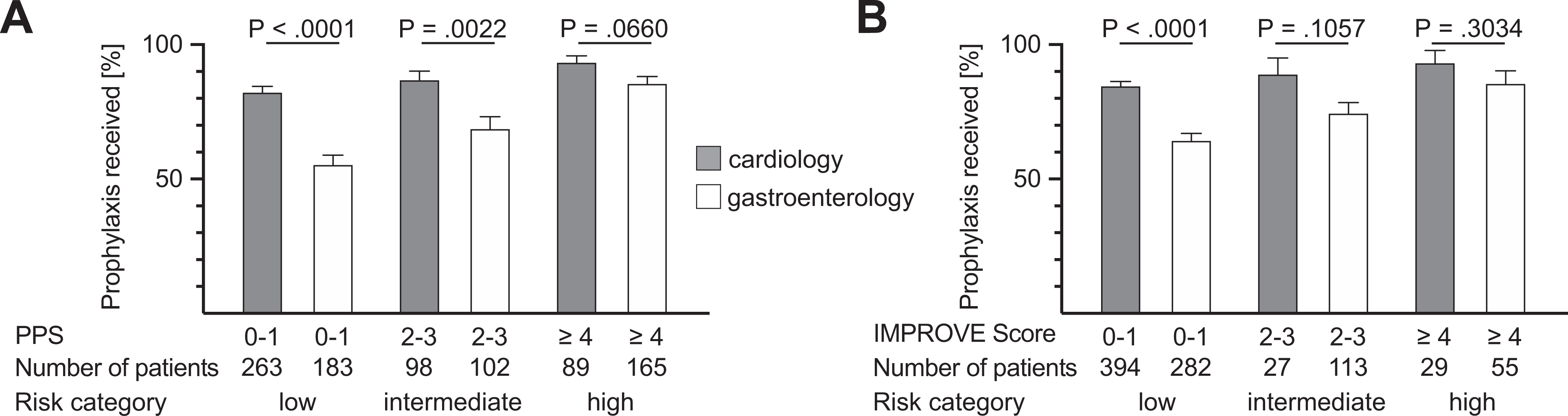
Padua and IMPROVE risk category and VTE prophylaxis. Patients were categorized in low, medium and high risk for VTE based on their Padua Prediction Score (PPS) or IMPROVE Score, y-achis displays the percentage of received VTE prophylaxis. The score range of each category is shown below the graphs as well as the number of patients in each group. Cardiology (gray bars) and gastroenterology (white bars) patients classified by PPS are shown in (A) and by IMPROVE Score in (B).
High-Risk
According to the PPS, 89 of 450 cardiology patients and 165 of 450 gastroenterology patients (Figure 3A) were defined as being at high risk (PPS ≥ 4) of a thrombotic event during their hospital stay. Of this high-risk population, 93.26% of the cardiology and 85.45% of the gastroenterology patients received drug-based prophylaxis. The difference between the 2 specialties did not meet the predetermined threshold for significance (P = .0660). Stratified by the IMPROVE Score 29 of 450 cardiology and 55 of 450 gastroenterology patients (Figure 3B) were classified to be at high-risk for VTE (IMPROVE Score ≥ 4) and 93.10% of the cardiology and 85.45% of the gastroenterology patients received prophylaxis. Again, the difference in VTE prophylaxis use was not statistically significant between the 2 groups (P = .3034).
Intermediate Risk
Grouped by the PPS, 98 of 450 cardiology patients and 102 of 450 gastroenterology patients (Figure 3A) had a PPS between 2 and 3. In this intermediate-risk group, the cardiology patients were more likely to receive VTE prophylaxis (86.73 vs. 68.63%, P = .0022). Classified by IMPROVE Score, 27 of 450 cardiology patients and 113 of 450 gastroenterology patients (Figure 3B) scored 2 to 3 points. The rate of VTE prophylaxis was 88.89% for the cardiology and 74.34% for the gastroenterology patients, a difference that did not meet statistical significance (P = .1057).
Low-Risk
Categorized by their PPS, 263 of 450 cardiology patients and 183 of 450 gastroenterology patients (Figure 3A) were considered to be at low risk (PPS ≤ 1) of VTE. Low risk cardiology patients were more likely to receive VTE prophylaxis than gastroenterology patients (82.13 vs. 55.19%, P = < .0001). Analyzed by IMPROVE Score, 394 cardiology patients and 282 gastroenterology patients (Figure 3B) were classified as low-risk. The percentages for VTE prophylaxis use were statistically different (P = < .0001) at 84.52% and 64.18%, respectively.
Correlation Between VTE Risk and prophylaxis
In case of the cardiology patients, the PPS (Figure 4A) significantly correlated with the likelihood of receiving drug-based VTE prophylaxis with an area under the curve (AUC) of 0.63 (95% CI 0.56-0.70). However, stratified by the IMPROVE Score (Figure 4B) no significant correlation was found (AUC 0.55, 95% CI 0.48-0.63). In contrast, in case of the gastroenterology patients the PPS (Figure 4C) significantly correlated with the likelihood of receiving VTE prophylaxis with an AUC of 0.67 (95% CI 0.62-0.73) as well as their IMPROVE Score (AUC 0.57, 95% CI 0.52-0.63, Figure 4D).
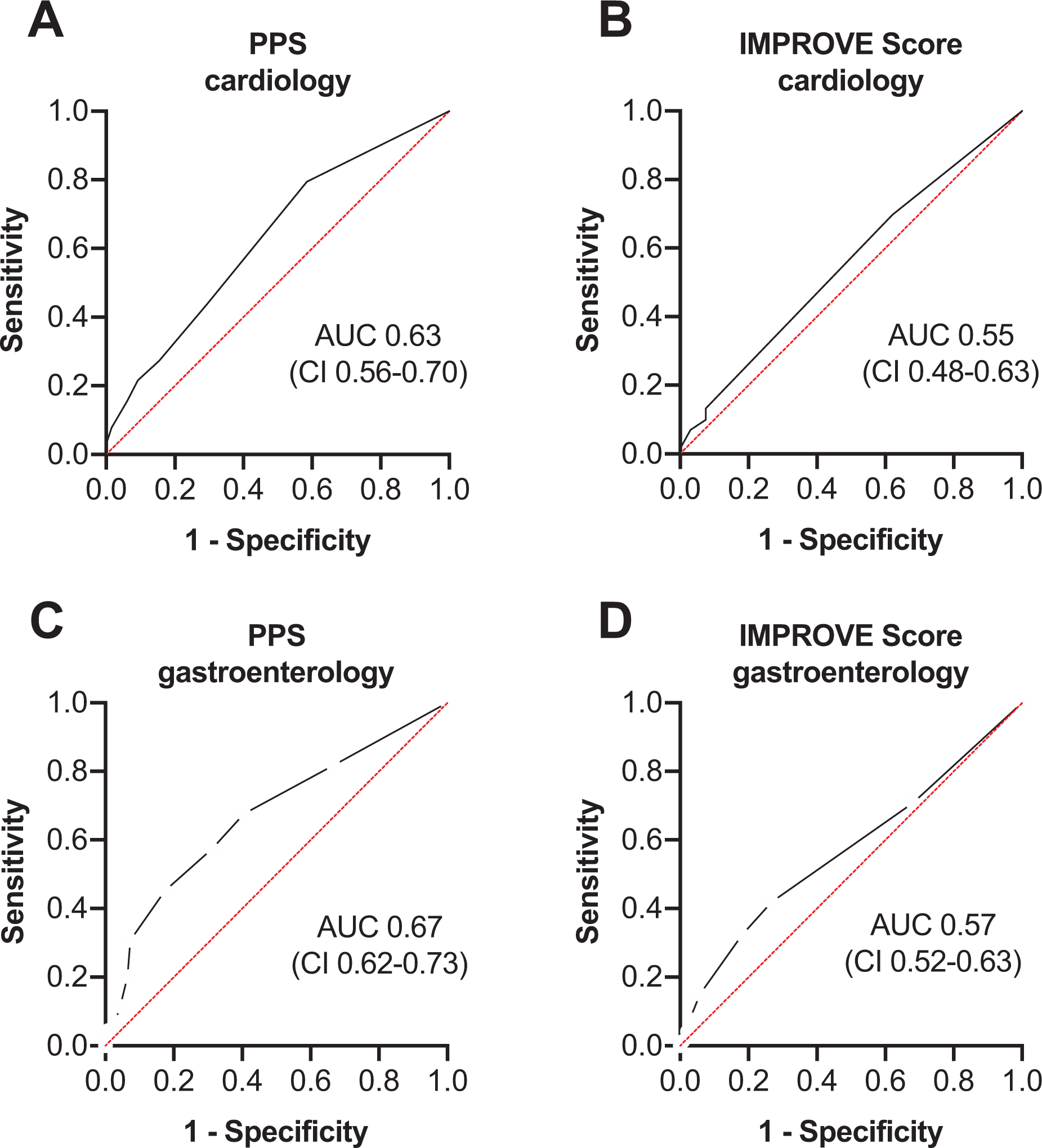
Receiver Operating Characteristic (ROC) curves of the interrelation between VTE-Score and likelihood of receiving VTE-prophylaxis. Logistic regression was performed after stratifying patients by their PPS or IMPROVE score and the likelihood of receiving VTE-Prophylaxis. PPS indicates Padua Prediction Score; AUC, area under the curve; CI, 95% confidence interval.
Differences in Patients Receiving Prophylaxis or Not
Next, we investigated whether bleeding risk or other factors differed between low-risk patients receiving VTE prophylaxis or not (Table 1). Neither the IMPROVE-Bleeding nor HAS-BLED Score showed significant differences between the 2 groups, although the length of hospital stay was significantly longer in patients receiving VTE prophylaxis for cardiology (Table 1A) as well as gastroenterology patients (Table 1B). A similar pattern was found when all patients were included or when the analysis was limited to high-risk patients (Table 1A and B). The total number of patients not receiving VTE prophylaxis in the high-risk group was low, especially for cardiology patients with an IMPROVE score of ≥ 4 with only 2 patients in this group. Thus, for the latter group statistical analysis was not possible.
Comparison between patients receiving prophylaxis or not.a

Abbreviations: PPS, Padua Prediction Score; LMWH, low molecular-weight heparin; SD, standard deviation.
a Differences regarding age, duration of hospital stay, sex and bleeding risk according to HAS-BLED and IMPROVE-Bleeding Score were examined between the patients receiving and not receiving prophylaxis. The P-values were calculated by using the χ2 test for categorial variables and t-test for numerical variables.
Duration of Hospital Stay
The prior results led us to investigate the correlation between the duration of hospital stay and prescription rate of VTE-prophylaxis. ROC analyses for the cardiology (Figure 5A) and gastroenterology patients (Figure 5B) are shown. For both patient groups, the correlation was stronger than these we had found between PPS or IMPROVE Score and VTE prophylaxis for the respective groups (AUC 0.66 with 95% CI of 0.60-0.73 for cardiology and AUC 0.78 with 95% CI of 0.74-0.83 for gastroenterology patients; see Figure 4 for comparison).

Receiver Operating Characteristic (ROC) curves of the interrelation between duration of hospital stay and likelihood of receiving VTE-prophylaxis. Logistic regression was performed between the duration of hospital stay and the likelihood of receiving VTE-prophylaxis for a cardiology patients and b gastroenterology patients. Abbreviations: AUC, area under the curve; CI, 95% confidence interval.
Increase of Bleeding Risk
We speculated that an increased risk of VTE would be associated with an increased risk of bleeding. While we could not find an association between the VTE risk and HAS-BLED Score, the IMPROVE-Bleeding Score showed a linear correlation between PPS (P = < .0001, Supplemental Figure 1a) and IMPROVE Score (P = .0140, Supplemental Figure 1b).
Comparing IMPROVE Score and PPS
To compare whether patients would fall into the same risk category by using both VTE risk scores we first grouped all patients by their IMPROVE Score and then calculated the corresponding PPS for each patient (Supplemental Figure 2). The most pronounced differences were found for intermediate-risk patients; 72.73% with an IMPROVE Score of 2 and 72.94% with an IMPROVE Score of 3 would be stratified as being at high risk based on PPS (score ≥ 4).
Rejection of Drug-Based VTE-Prophylaxis
Overall, few patients rejected drug-based VTE-prophylaxis (8 cardiology and 17 gastroenterology patients) most but not all of them were at low to intermediate risk for VTE.
Discussion
More cardiology than gastroenterology patients had to be excluded from our study because of indications for oral anticoagulation indications, e.g. atrial fibrillation. In addition, the 2 patient populations differed in many clinical characteristics. Both had been expected, since cardiologists and gastroenterologists focus on treating patients with different diseases.
Exclusion criteria were based on the exclusion criteria used in the observational studies from which the PPS 15 and IMPROVE Score 17 were obtained. From their PPS cohort Barbar et al 15 excluded about 44% of patients mainly for the indication of therapeutic anticoagulation, while we excluded 53%. The slightly higher exclusion rate in our cohort was caused by a higher proportion of cardiological patients, and thus a higher rate of comorbidities such as atrial fibrillation. Spyropoulos et al (2011) excluded about 55% of patients from their IMPROVE cohort, again mainly for use of therapeutic anticoagulation in addition to missing consent or missing data. 16,17
It was one of the initial hypotheses of our study, that the specialization of the treating physicians would influence their prescription habits in case of VTE prophylaxis, since cardiologists tend to see and treat more patients with thrombotic or thromboembolic diseases, while gastroenterologists are more often faced with patients suffering from gastrointestinal bleeding. In line with this hypothesis, we found cardiology patients with PPS and IMPROVE Scores of 0 -1 to be more often treated with LMWH during their hospital stay than their gastroenterology counterparts belonging to the same category of VTE low-risk patients.
As mentioned above, in the multinational cross-sectional study ENDORSE patients being at high risk of VTE were nearly universally treated with LMWH. 14 We found a similar high prescription rate in our patient populations with a numerically but not statistically higher rate of VTE prophylaxis in cardiology patients. Nearly all cardiology patients in the high-risk group received treatment.
An increasing PPS was found to be a good predictor of whether patients would receive VTE prophylaxis with a predictive value being slightly better for gastroenterology than cardiology patients. In contrast, the IMPROVE Score showed only a slight correlation with gastroenterology and no statistical correlation with cardiology patients receiving VTE prophylaxis. Still, the best prognosticator was the duration of hospital stay. Thus, in our patient population doctors seem to put more emphasis on how long a patient would stay in the hospital than the risk factors based on 2 established risk scores.
Which leaves the question how doctors might have known that some patients would have a longer hospital stay than others? First, patients were classified as VTE prophylaxis received, if it was prescribed for more than half of the hospital stay. Giving doctors time to decide how long a patient would likely stay in the hospital. Second, neither PPS nor IMPROVE Score account for how severely ill patients are nor for the reasons of the hospital stay. While doctors can use the reason of admission as well as the clinical gestalt to predict how long a patient will likely stay in the hospital.
Neither a high IMPROVE-Bleeding score nor a high HAS-BLED Score prevented doctors from treating patients with medical VTE prophylaxis. This result is in line with the finding from a retrospective database study with patients treated on an intensive care unit because of lower gastrointestinal bleeding. 20 Despite gastrointestinal bleeding, subcutaneous heparin for VTE prophylaxis was administered to more than 50% of the patients. As a consequence, these patients needed significantly more blood transfusions. The IMPROVE-Bleeding Score has been validated as a strong predictor of bleeding complications in our patient population 21 –23 while the HAS-BLED Score is mainly used in patients with atrial fibrillation. 19 Nevertheless, the HAS-BLED Score was used in a similar fashion in other studies. 24 Since the IMPROVE-Bleeding Score correlated well with the IMPROVE Score, patients being at increased risk for bleeding were at very high-risk for VTE events as well. Among other things, this can be explained by the fact that some risk factors such as age or active cancer are used for both risk assessment models.
In addition, we found some important discrepancies between guiding treatment decisions with regard to IMPROVE Score or PPS. About 72.86% of the patients of the intermediate-risk group by IMPROVE Score with score values of 2 or 3 were classified as being at high risk (score value ≥ 4) by PPS. Furthermore, 11.24% of the patients of the low-risk group by IMPROVE Score (score value 0 -1) were classified as being at high risk by PPS. And more patients were classified as increased or high-risk for VTE by PPS compared to IMPROVE Score. The IMPROVE Score failed to identify high-risk patients in the setting of the MARINER study, 25 even though the differences in study design like shorter follow-up, exclusion of in-hospital VTE events, universal usage of medical VTE prophylaxis during the index hospitalization as well differences in comorbidities and co-medication in the MARINER study population might account for this. Thus, neither scoring system seemed to be perfect for classifying all patients. Still, individualized treatment based on established risk models is more likely to have a net benefit than qualitative models or group prophylaxis strategies. 26,27
The increasing availability of electronic health records lends itself for the integration of automated treatment recommendation for medical VTE prophylaxis by checking if patients are receiving VTE prophylaxis and calculating risk probabilities for VTE events to assist in the correct decision for each individual patient.
Limitations
One limitation is the use of retrospective analysis of electronic health records and therefore the reliance on completeness and correctness of the records. We put a high emphasis on extracting all relevant information and excluded patients with missing or ambiguous data. In addition, the results of this monocentric study might not be transferable to all hospitals and countries. Furthermore, our study focused on prescription habits and not on associated VTE and bleeding events. Therefore, it would be underpowered to find changes in these outcomes. The association between the prescription of VTE prophylaxis as well as VTE and bleeding events has already been established in other studies. 11 –13 Our aim was to investigate how this knowledge has influenced current prescription practice.
Conclusions
In summary, we found a high rate of VTE prophylaxis prescription in both patient populations. Our hypothesis that cardiologists might be more likely to prescribe VTE prophylaxis during a patient’s hospital stay than their gastroenterology counterparts could be confirmed, at least for patients being at low risk of VTE events based on PPS and the IMPROVE Score. With crucial discrepancies between the 2 scores concerning how they would classify single patients, it is hard to accurately predict the risk of each patient. In addition, treating physicians in our study seemed to put the most weight on the duration of hospital stay when they had to decide whether to prescribe VTE prophylaxis.
Supplemental Material
Supplemental Material, sj-pptx-1-cat-10.1177_1076029621995563 - Do Inpatients Receive Risk-Based Prophylactic Treatment for Thrombotic Events?
Supplemental Material, sj-pptx-1-cat-10.1177_1076029621995563 for Do Inpatients Receive Risk-Based Prophylactic Treatment for Thrombotic Events? by Armin Nemani, Constantin von zur Mühlen, Friederike Steffen, Johannes Schulte, Christoph Bode and Marvin Krohn-Grimberghe in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
We thank Klaus Kaier, PhD from the Institute for Medical Biometry and Statistics (IMBI), for his assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.