
Abstract
In unfractionated heparin (UFH) monitoring during extracorporeal circulation, the traditional measures of activated clotting time (ACT) or activated partial thromboplastin time (APTT) may diverge, confounding anticoagulant adjustments. We aimed to explore the factors explaining this discrepancy in children and young adults. This retrospective observational study, conducted at an urban regional tertiary hospital, included consecutive pediatric patients who received UFH during extracorporeal circulation (continuous kidney replacement therapy or extracorporeal membrane oxygenation) between April 2017 and March 2021. After patients whose ACT and APTT were not measured simultaneously or who were also taking other anticoagulants were excluded, we analyzed 94 samples from 23 patients. To explain the discrepancy between ACT and APTT, regression equations were created using a generalized linear model (family = gamma, link = logarithmic) with ACT as the response variable. Other explanatory variables included age, platelet count, and antithrombin. Compared to APTT alone as an explanatory variable, the Akaike information criterion and pseudo-coefficient of determination improved from 855 to 625 and from 0.01 to 0.42, respectively, when these explanatory variables were used. In conclusion, we identified several factors that may explain some of the discrepancy between ACT and APTT in the routinely measured tests. Evaluation of these factors may aid in appropriate adjustments in anticoagulation therapy.
Keywords
Introduction
Hemorrhage and thrombosis are the most serious complications during extracorporeal circulation, with high morbidity and mortality rates. In adult patients undergoing venoarterial extracorporeal membrane oxygenation (VA-ECMO), the rates of significant bleeding, overt thrombotic events, and in-hospital mortality are 68.5%, 16.7%, and 59.3%, respectively. 1 Furthermore, a systematic review of venovenous extracorporeal membrane oxygenation (VV-ECMO) reported bleeding and thrombosis rates of 16% and 53%, respectively. 2 In continuous kidney replacement therapy (CKRT), where blood flow is slower than that in ECMO, premature clotting of the circuit is a major problem, leading to shorter circuit life, blood loss, reduced dialysis efficiency, increased workload, and higher costs. 3 Appropriate anticoagulant therapy is, therefore, essential to minimize these complications; however, optimal monitoring of anticoagulants in extracorporeal circulation has not yet been established. Owing to the limitations of each of the laboratory tests commonly used to monitor unfractionated heparin (UFH), the Extracorporeal Life Support Organization recommends a comprehensive evaluation that combines multiple tests. 4
In North America and Europe, anti-Xa activity and blood viscoelasticity tests are increasingly being used to monitor UFH, in addition to traditional tests such as activated clotting time (ACT) and activated partial thromboplastin time (APTT).5,6 Anti-Xa activity is a more direct measure of the anticoagulant effect of UFH while blood viscoelasticity provides information on various processes, from fibrinogenesis to fibrinolysis. However, there are still many countries and regions, including Japan, that face challenges in routinely conducting these tests owing to factors like costs, insurance coverage, and technical challenges. In such countries, heparin dosage adjustment is still based on traditional measures of ACT and APTT.
Although ACT and APTT both measure coagulation time by intrinsic coagulation mechanisms, poor correlation between the two tests has been reported,7-9 often leading to divergent measurement results. This discrepancy can lead to confusion in the interpretation of results and the risk of failure to adjust heparin dosage, which can contribute to bleeding or thrombus formation. Enhanced comprehension of factors behind ACT and APTT inconsistencies could lead to more accurate result interpretation.
We hypothesize that basic patient information (eg, age and weight) and common blood tests that are readily available worldwide may include factors that could elucidate the discrepancy between ACT and APTT. If we can identify even a partial explanation for the discrepancy between ACT and APTT, we may be able to better interpret the results of their measurements and better adjust for anticoagulants accordingly. ACT is reported to be affected by platelet count, hemodilution, hypothermia, hemoglobin, and antithrombin (AT) III levels,10,11 and APTT by acute phase reactants (eg, C-reactive protein), 12 blood sample volume, 13 and lupus anticoagulants. 14 Of these, factors that can be routinely measured were included in the current study. In this study, we aimed to explore the factors contributing to the discrepancy between ACT and APTT in patients who were administered UFH as an anticoagulant in extracorporeal circulation, using the information from routine practice.
Materials and Methods
Study Design and Setting
This study was a retrospective, single-center, observational study at the pediatric intensive care unit (PICU) of Osaka City General Hospital. This unit is a multivalent PICU with 12 beds. We included consecutive patients who were admitted to the PICU and received UFH during extracorporeal circulation for CKRT or ECMO between April 2017 and March 2021. Exclusion criteria comprised patients with coagulation/platelet abnormalities, non-simultaneous ACT and APTT measurements, or concurrent use of other anticoagulants like nafamostat mesylate. Samples in which ACT and APTT were measured simultaneously were used for further analysis. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement. 15
Anticoagulation and Circuit Strategies During Extracorporeal Circulation at our Hospital
The first choice of anticoagulant during blood extracorporeal circulation is UFH. If there was a high risk of hemorrhage, NM or no anticoagulant was selected. For both ECMO and CKRT, the initial control targets for ACT and APTT when UFH was used were 180-220 and 45-60 s, respectively. If there was early circuit blockage, the target was raised, and if there was significant bleeding, the target was lowered. In addition, because ECMO carries a higher risk of bleeding than CKRT, a platelet count of at least 100,000/µL and fibrinogen level of at least 150 mg/dL are maintained during ECMO. Usually, only saline is used for circuit priming; however, if the priming volume exceeds 10% of the circulating blood volume, half the priming volume of the red blood cell product is used to fill the circuit.
Survey Contents
In addition to demographic factors representing the characteristics of the study participants, factors that could theoretically influence the discrepancy between ACT and APTT were retrospectively extracted from the data available in the electronic medical records. Patient demographic data included age (months), weight (kg), sex, diagnosis at PICU admission, underlying medical conditions, type of extracorporeal blood circulation (CKRT/ECMO), and reason for introducing extracorporeal circulation. Blood tests included testing for ACT (s), APTT (s), prothrombin time (PT) (s), fibrinogen (mg/dL), AT (%), fibrinogen/fibrin degradation products (μg/mL), white blood cell count (/µL), hematocrit (%), platelet count (103/µL), C-reactive protein level (mg/dL), and ionized calcium concentration (mmol/L). Heparin dose (U/kg/hour) was included as an additional parameter. All blood samples were collected from the arterial lines, and sufficient blood was drawn to prevent heparin contamination. ACT was measured using the Hemochron® Response instrument by contact activation with Celite (International Technidyne Corporation, Edison, NJ, USA). APTT was measured using CS-5100 (Sysmex Corporation, Kobe, Japan). The normal reference ranges for ACT and APTT were 70-120 s and 24-37 s, respectively.
Statistical Analysis
Continuous variables were expressed as medians with interquartile ranges or minimum-maximum, while categorical variables were expressed as frequencies and percentages. Spearman's ranked correlation coefficient was used to assess the correlation between variables. The false discovery rate method was used to correct multiple correlation tests. To explain the discrepancy between ACT and APTT, a generalized linear model (GLM) was constructed with ACT as the response variable and APTT and other factors assumed to be possible causes of the discrepancy as explanatory variables. The response variable ACT was assumed to follow a gamma distribution because it was a continuous value greater than or equal to zero. The logarithmic link function was chosen, and the backward-forward stepwise method using the Akaike information criterion (AIC) was used to select the best-fitting model. Pseudo-coefficient of determination (pseudo-R2) was used to evaluate the fit of the models. A t-test was used to determine whether the estimated value of the coefficient for each explanatory variable in the regression model was zero. The variance inflation factor (VIF) was calculated to assess multicollinearity among the explanatory variables. Statistical significance was set at P < .05 for two-sided tests. Statistical analyses were performed using R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria; www.R-project.org).
Ethics Approval and Consent to Participate
The study protocol was approved by the ethics committee of Osaka City General Hospital (reference number: 2212104) and was conducted in compliance with the 1975 Declaration of Helsinki and Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects. In addition, the aforementioned ethics committee waived the need for informed consent from the patients because only non-personally identifiable data from electronic patient records were used, and no personal information was disclosed.
Availability of Data and Materials
The data supporting the findings of this study are available in the Supplemental material.
Results
Characteristics of Study Participants
A total of 94 specimens from 23 patients who met the inclusion criteria were analyzed (Figure 1). Table 1 shows the patient demographics. The median age, weight, and height of the patients were 21 months, 9.4 kg, and 71 cm, respectively. The prevalence of the most common diseases that require extracorporeal circulation, such as circulatory disorders, post-cardiac arrest, metabolic disease, and sepsis, was 34.8%, 21.7%, 17.4%, and 8.7%, respectively. The percentages of patients with congenital heart disease and malignant tumors as underlying diseases were 39.1% and 8.7%, respectively. Postoperative ICU admission accounted for 34.8% of the patients, and the ICU and hospital mortality rates were 21.7% and 26.1%, respectively.
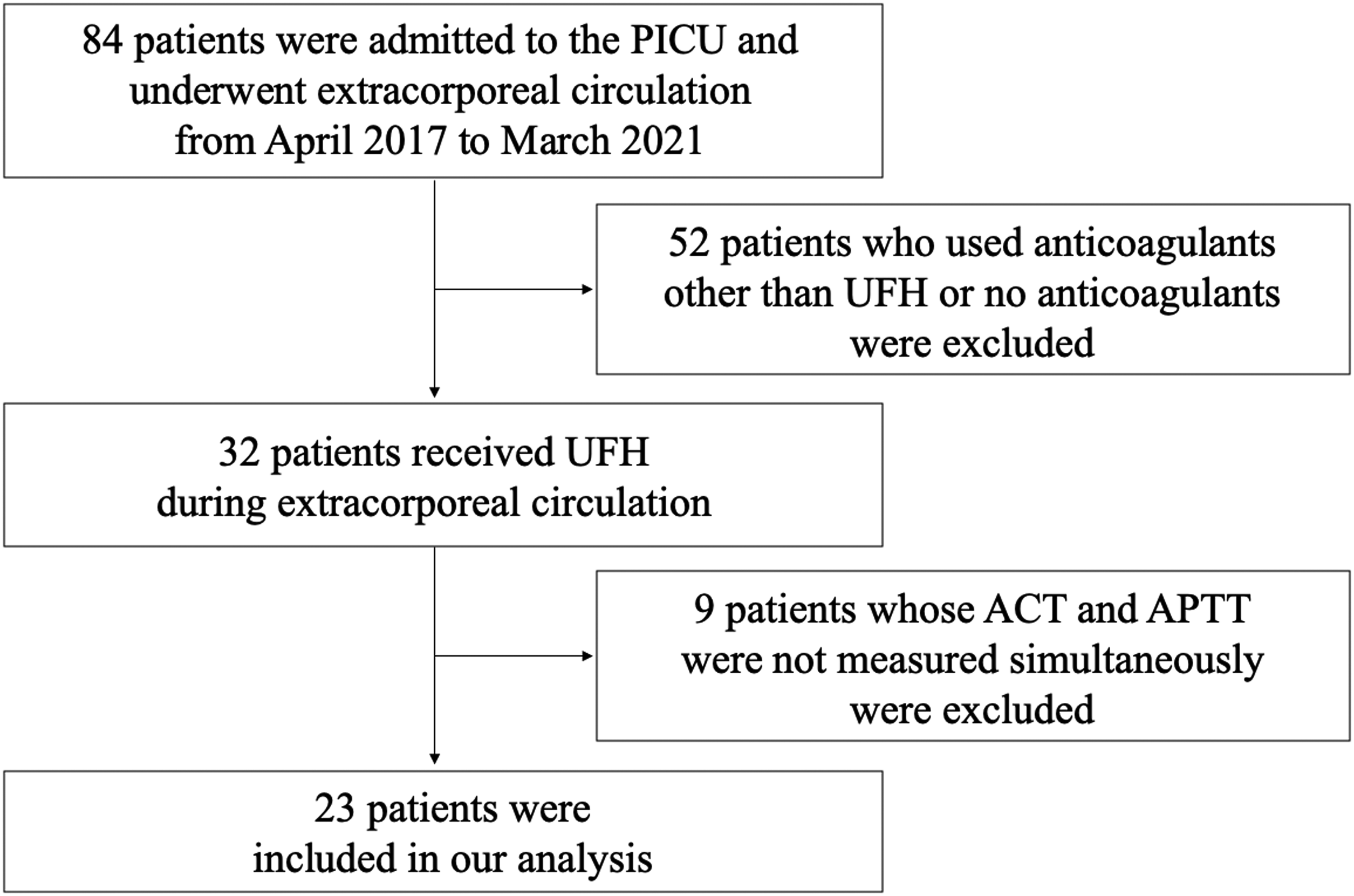
Study enrollment. PICU, pediatric intensive care unit; UFH, unfractionated heparin; ACT, activated clotting time; APTT, activated partial thromboplastin time.
Patient Demographics.
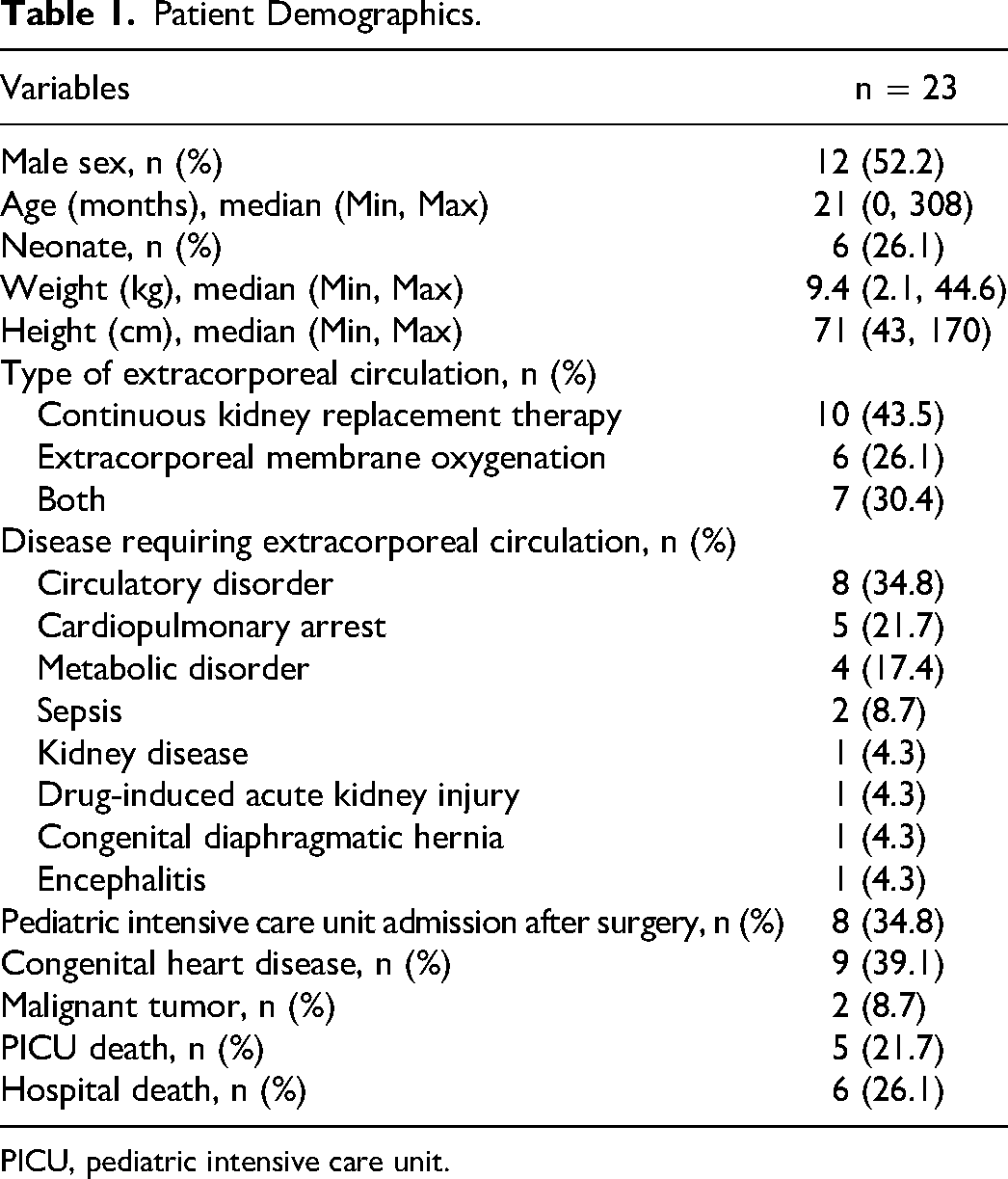
PICU, pediatric intensive care unit.
The variables that may have influenced the discrepancy between ACT and APTT are listed in Table 2. In eight samples, the measurement sensitivity of the APTT was exceeded (>170 s). A scatterplot of ACT and APTT, excluding the eight samples, is shown in Figure 2. Spearman's ranked correlation coefficient between ACT and APTT was 0.04 (P = .74). The correlation coefficients between the variables are listed in Table 3. The false discovery rate method was used to correct for multiple tests. ACT showed a significant positive correlation with age (in months) and weight with correlation coefficients of 0.30 and 0.29, respectively. Meanwhile, APTT significantly correlated with PT and fibrinogen, with correlation coefficients of 0.50 and − 0.30, respectively. Age (months) and weight were strongly correlated (correlation coefficient = 0.97).
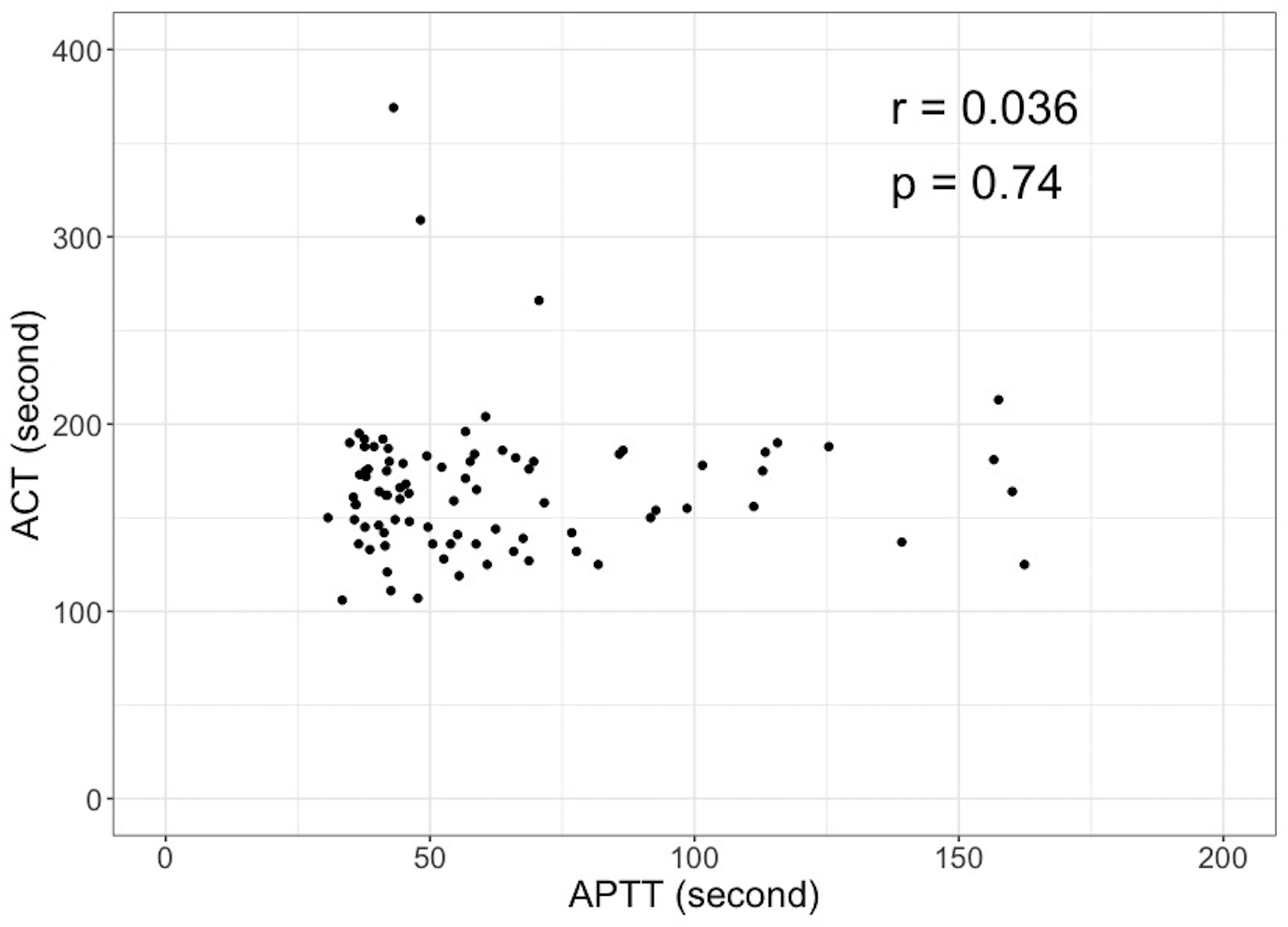
Scatterplot and correlation between ACT and APTT. To evaluate the correlation between ACT and APTT, a test of no correlation using Spearman’s rank correlation coefficient was performed. The correlation coefficient (r) was 0.036, with a P-value of .74. ACT, activated clotting time; APTT, activated partial thromboplastin time.
Variables That Might Explain the Discrepancy Between ACT and APTT.
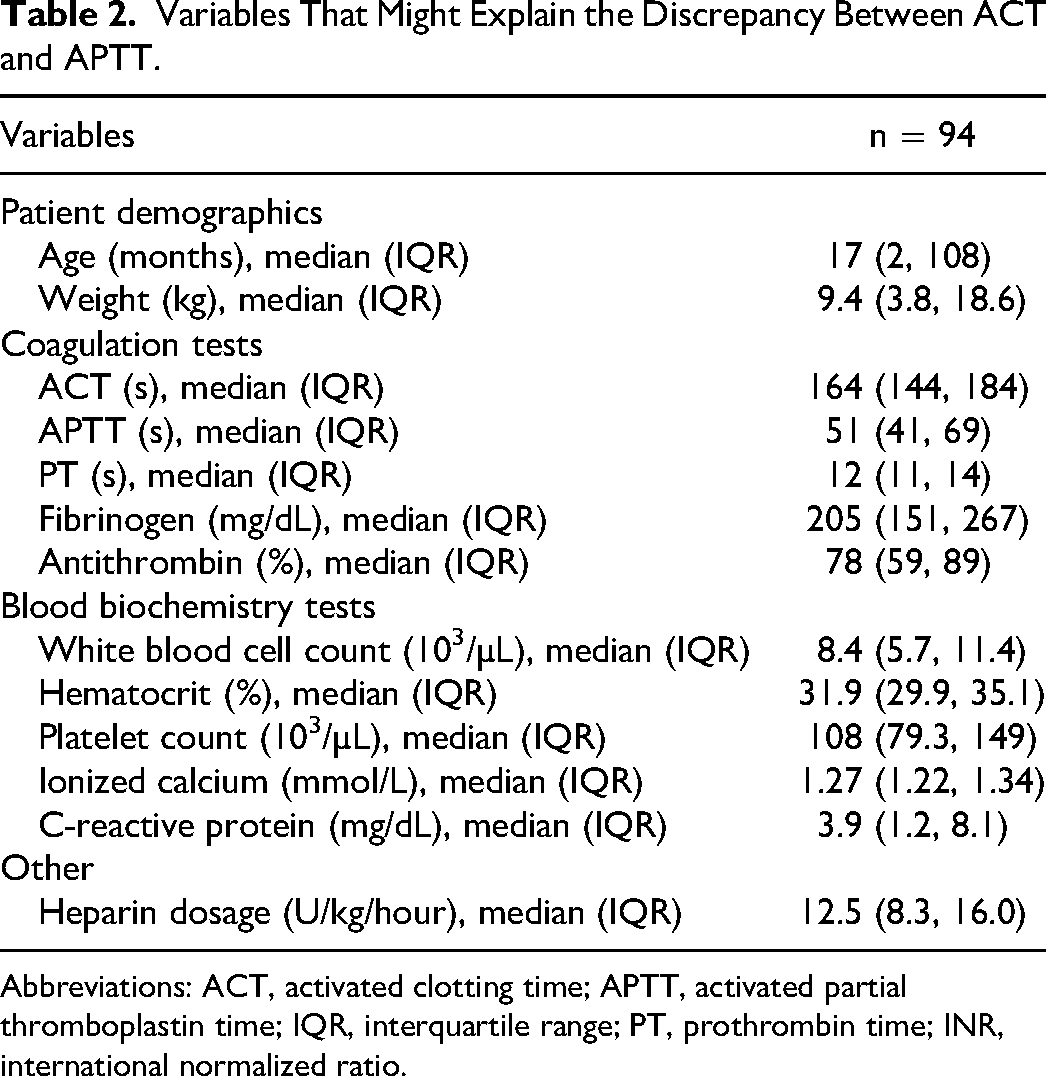
Abbreviations: ACT, activated clotting time; APTT, activated partial thromboplastin time; IQR, interquartile range; PT, prothrombin time; INR, international normalized ratio.
Correlation Coefficients Between Each variable.
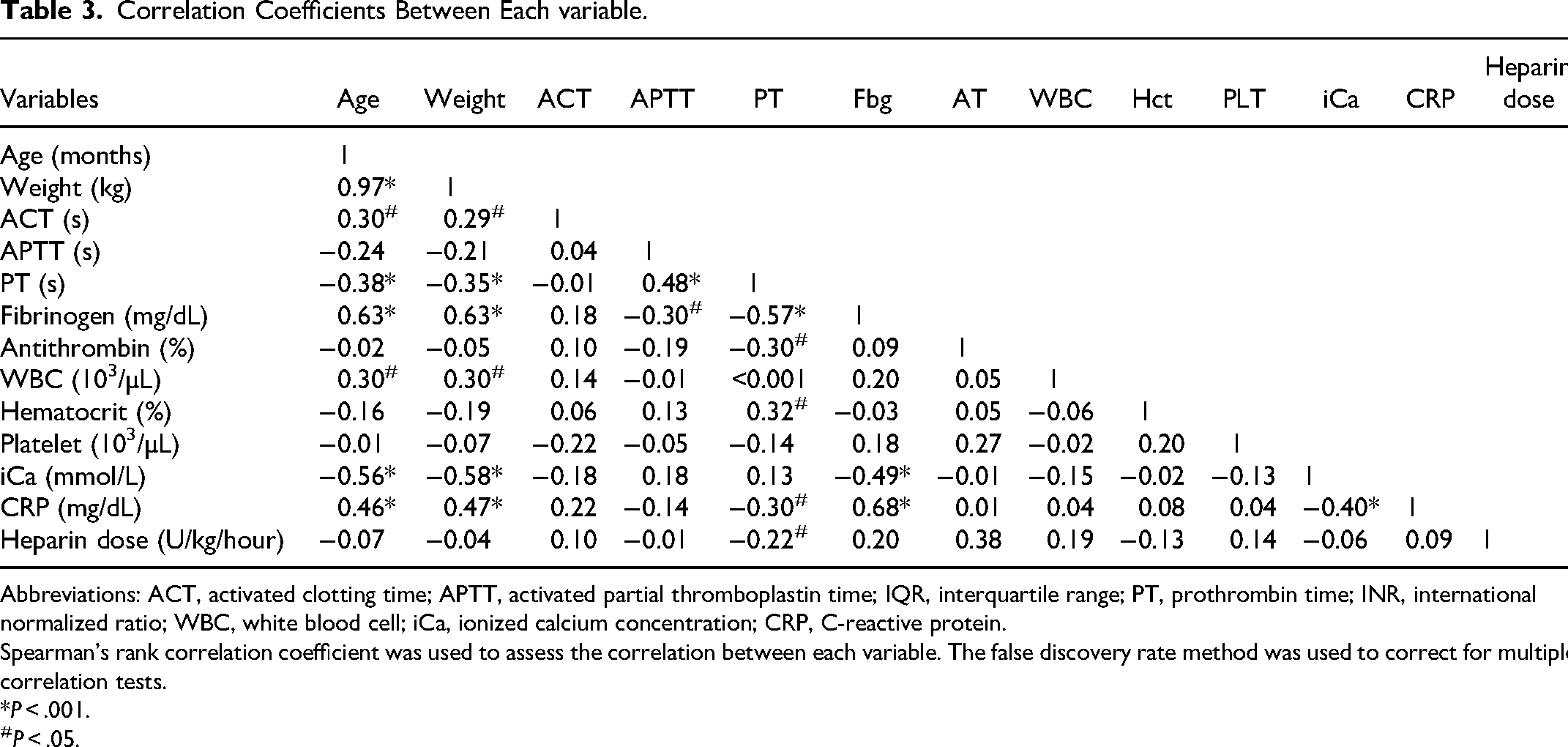
Abbreviations: ACT, activated clotting time; APTT, activated partial thromboplastin time; IQR, interquartile range; PT, prothrombin time; INR, international normalized ratio; WBC, white blood cell; iCa, ionized calcium concentration; CRP, C-reactive protein.
Spearman's rank correlation coefficient was used to assess the correlation between each variable. The false discovery rate method was used to correct for multiple correlation tests.
*P < .001.
P < .05.
GLMs were then developed for various combinations of explanatory variables, including APTT and ACT as response variables. Only age (months) was selected out of age (months) and weight, as it showed a robust correlation, as described above. A summary of each model selected using the stepwise method is presented in Table S1. First, in the model with APTT as the only explanatory variable, the AIC was 855 and the pseudo-R2 was 0.001. Based on an overall assessment of the model fit and clinical importance, the following were selected as the best models: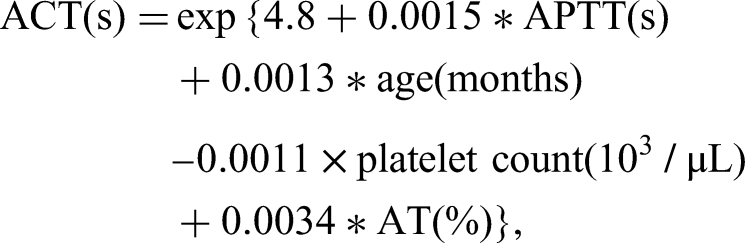
This model equation has been transformed to make it more comprehensible. By defining and substituting several equations, the original model equation can be simplified as follows:




Discussion
In this study, we developed a regression equation using readily available clinical practice data to identify the factors affecting the discrepancy between ACT and APTT. Compared to the model where ACT was considered as the dependent variable and APTT as the sole explanatory variable, the final model demonstrated improvement, reaching an acceptable—though not optimal—level, as evidenced by a decrease in AIC from 855 to 625 and an increase in pseudo-R2 from 0.01 to 0.42. The factors explaining the discrepancies in the final model were age (months), platelet count, and AT activity.
In this study, the discrepancy between ACT and APTT increased with increasing age, with a relative prolongation in ACT. To some extent, the development of a coagulation system may explain the relationship between age and coagulation time. For instance, at birth, only fibrinogen, FV, and FVIII are present in levels corresponding to the normal adult range, whereas other coagulation-promoting factors, vitamin K-dependent coagulation factors (FII, FVII, FIX, FX), contact factors (FXI, FXII, and prekallikrein), and high-molecular-weight kininogens are only approximately 50% of the corresponding values in adults. These factors increase rapidly in the first few weeks of life and approach adult values by 6 months of age, but most factors are reported to be 20% lower than adult values until teenage years. Furthermore, in a previous study that investigated the normal reference range for coagulation with respect to age in healthy individuals, APTT was found to range between 1.2-1.27 at birth and 1.10-1.14 from 6 months to 10 years of age, with the value in adults being 1.0. 16 Specifically, APTT tends to decrease with age. We also observed a negative correlation of − 0.24 between age and APTT. Conversely, a positive correlation of 0.30 was observed between age and ACT. Although the cause of the inverse correlation between APTT and ACT with age is unclear, this is an interesting finding and a subject for future research.
Regarding platelets, ACT was prolonged relative to APTT as platelet counts decreased and the discrepancy between ACT and APTT increased in this study. Previous studies have similarly reported that thrombocytopenia worsens the agreement between ACT and APTT. 7 In considering the effect of platelet count on these coagulation tests, the difference in specimens is primarily important: whole blood is used as the specimen in ACT, whereas platelet-poor plasma, which contains few platelets, is used in APTT. Thus, APTT is largely unaffected by platelet count. Platelets play a role in adhesion and aggregation at the site of vascular injury as well as promote activation of the coagulation cascade. Increased platelet counts, and thus, increased platelet concentrations, promote thrombus formation by increasing phospholipid levels, which are substrates for tenase and prothrombinase complexes. 17 Conversely, decreased platelet counts result in prolonged ACT, as measured by thromboelastography. 18 This may explain the present results, in which decreased platelet counts resulted in prolonged ACT and a consequent increase in discrepancy between ACT and APTT.
Finally, increased AT activity was associated with prolonged ACT and increased discrepancy compared with APTT in this study. Since UFH has an indirect anticoagulant effect mainly by binding to AT, an increase in AT activity may enhance the anticoagulant effect of heparin and prolong coagulation time. 19 The present results suggest that the response to increased AT activity was greater for ACT than for APTT, but the reason for this is unclear. ACT has a larger reference value than APTT, which may reflect a relatively greater degree of prolongation.
The clinical applications of the present results will then be considered. In the simplified equation developed in the present study, ACT was expressed as the product of factors comprising the explanatory variables APTT, age in months, platelets, and AT, with a coefficient of 121.5. Table 4 presents the theoretical ranges for each explanatory variable. By substituting specific values, one can analogize the strength and direction of the impact of each explanatory variable on ACT. As another approach, among the explanatory variables in the present prediction equation, we assumed that APTT, age (months), and AT activity were constant at 50 s, 12 months, and 60%, respectively. If we then assume that the platelet count decreases to 150,000, 50,000, and 10,000/µL, the predicted values of ACT will be extended to 138.3 s, 154.4 s, and 161.4 s, respectively. Thus, by fixing two of the three explanatory variables and varying the remaining variable, the trend of changes in ACT measurements can be predicted. When ACT is excessively prolonged relative to APTT, it is possible to assume that the patient is older in months, has higher AT activity, or has a lower platelet count. If the platelet count is low, we can consider employing a less affected APTT, or if bleeding due to low platelets is a problem, transfusing a platelet product to correct the platelet count and then retesting the ACT. We then consider the modifiable factor, AT, which we set at 50 s APTT, 12 months of age, and a platelet count of 100,000/µL; varying AT by 20, 60, and 100% gives an ACT of 127.6, 146.1, and 167.4 s, respectively. This shows that a low AT shortens the ACT relative to the APTT. In other words, when the AT is low, ACT may underestimate anticoagulation therapy. If this is the case, it can be corrected by administering an AT concentrate. First, the anticoagulant effect of heparin is mainly mediated by AT, and low AT attenuates the effect of heparin. Their supplementation is recommended only when there is a clinical indication for their deficiency and should not be done only to correct the discrepancy between ACT and APTT.
Approximate Numerical Range of Equations with Each Explanatory variable.
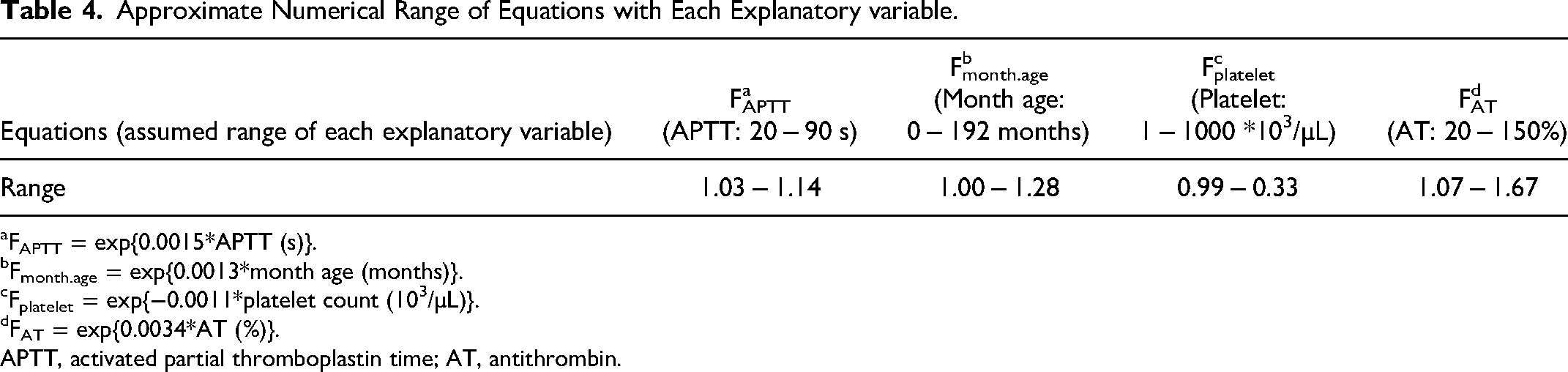
FAPTT = exp{0.0015*APTT (s)}.
Fmonth.age = exp{0.0013*month age (months)}.
Fplatelet = exp{−0.0011*platelet count (103/µL)}.
FAT = exp{0.0034*AT (%)}.
APTT, activated partial thromboplastin time; AT, antithrombin.
There is an ongoing debate regarding the preference between APTT and ACT. 20 APTT lacks blood cells in the sample, and the reagent contains phospholipids and Ca ions, which results in fewer factors that may influence the measured value compared to ACT. Additionally, some reports suggest that APTT more accurately reflects heparin concentration 21 ; therefore, we prefer APTT in case of discrepant results. In a study of pediatric patients on ECMO, heparin monitoring using ACT was associated with more bleeding complications, whereas monitoring using APTT was associated with more thrombotic complications. 22 As described above, both ACT and APTT have advantages and disadvantages, and a clinical decision must be made on a case-by-case basis for each individual patient.
Naturally, the three explanatory factors identified in this study might not comprehensively explain all variations. However, this innovative and straightforward approach for elucidating ACT and APTT inconsistencies offers a fresh viewpoint for enhancing anticoagulant monitoring through existing tests. In the future, we plan to increase the sample size and expand the explanatory factors, which may allow the identification of more accurate prediction equations, a better explanation of the discrepancies, and provide more detailed results.
This study had some limitations. First, this was a single-center study, and the results may not be generalizable to all centers because patient backgrounds and medical management vary across institutions and countries. Furthermore, because ACT and APTT measurements vary depending on the measuring device and reagents, the creation of prediction equations using data from each facility is preferable. The second limitation of the study was the small number of cases. Because we did not routinely measure ACT and APTT simultaneously at our institution, patients with different backgrounds were included to collect as many cases as possible. Regarding the impact of including CKRT and ECMO cases simultaneously, the effect of APTT on ACT changes with the type of extracorporeal circulation was tested using a covariance model. The results showed no evidence of an interaction between APTT and the type of extracorporeal circulation (F value = 2.49, degree of freedom = 1, 233, P = .11); therefore, the effect of including these cases simultaneously was determined to be small. However, the potential impact of clinical differences between ECMO and CKRT on the study results cannot be excluded; therefore, future research evaluating each of them separately with more cases is necessary. Third, this study only examined simple factors that are commonly tested in many institutions worldwide. There may be items other than those used in this study that could better explain the discrepancy between ACT and APTT. In addition, as the present study merely identified the factors that explain the discrepancy, the causes of the discrepancy were not examined in depth. More specialized and specific tests (eg, thromboelastography) are needed to examine the causes. Finally, owing to the retrospective design of this study, we did not examine the causality or accuracy of the prediction equation. A prospective evaluation is required to determine the validity of this prediction equation.
Conclusion
This retrospective study identified three factors that may explain some of the discrepancies between ACT and APTT. As a key takeaway, in cases where ACT and APTT deviate, monthly age, platelet count, and AT should also be examined. If platelets and AT are found to be low and their supplementation is clinically appropriate, supplementing them may correct some of the discrepancies. Our findings are poised to contribute to improved anticoagulation management in regions and countries that rely predominantly on traditional ACT and APTT for anticoagulant monitoring in extracorporeal circulation.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241252838 - Supplemental material for Factors Affecting the Discrepancy Between Coagulation Times on Extracorporeal Circulation Using Unfractionated Heparin in Children and Young Adults
Supplemental material, sj-docx-1-cat-10.1177_10760296241252838 for Factors Affecting the Discrepancy Between Coagulation Times on Extracorporeal Circulation Using Unfractionated Heparin in Children and Young Adults by Taiki Haga, Yotaro Misaki, Takaaki Sakaguchi and Yoko Akamine in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-csv-2-cat-10.1177_10760296241252838 - Supplemental material for Factors Affecting the Discrepancy Between Coagulation Times on Extracorporeal Circulation Using Unfractionated Heparin in Children and Young Adults
Supplemental material, sj-csv-2-cat-10.1177_10760296241252838 for Factors Affecting the Discrepancy Between Coagulation Times on Extracorporeal Circulation Using Unfractionated Heparin in Children and Young Adults by Taiki Haga, Yotaro Misaki, Takaaki Sakaguchi and Yoko Akamine in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.