
Abstract
Objective
To investigate the safety and efficacy of regional citrate anticoagulation (RCA) on elderly patients at high risk of bleeding after continuous renal replacement therapy (CRRT).
Methods
A total of 31 patients at high risk of bleeding who received CRRT in the intensive care unit were collected. The patients were divided into RCA group (n = 17) and no anticoagulation group (NA, n = 14) according to whether RCA was used or not. The levels of creatinine (Cr), blood urea nitrogen (BUN), prothrombin time (PT), activated partial thromboplastin time (APTT), total calcium (tCa), ionized calcium ion (iCa2+), sodium ion (Na+), bicarbonate ion (HCO3−), tCa/iCa2+ ratio, and pH were observed after treatment. The filter use time, number of filters used, filter obstruction events, clinical outcomes, and safety evaluation indexes were compared post-treatment.
Results
After treatment, serum Cr and BUN levels, APTT and PT levels in the RCA group were significantly lower than the NA group. The tCa, iCa2+, HCO3−, tCa/iCa2+, and pH were within the normal range after RCA treatment while Na+ levels saw a significant increase. In the RCA group, the filter using time was significantly longer, with significantly reduced numbers of filter use within 72 h and filter disorder events. Additionally, patients in the RCA group showed significant recovery of renal function and a significant reduction in bleeding events and in-hospital mortality.
Conclusion
RCA treatment significantly improves clinical outcome of patients at high risk of bleeding after CRRT, safely and effectively prolongs the filter life and avoids coagulation incidences.
Keywords
Introduction
Acute kidney injury (AKI) is a group of clinical syndromes referring to renal function's sudden and continuous decline. This scenario has become a prevalent disease in the intensive care unit (ICU).1,2 It has been reported that patients with AKI in developed countries account for 3.2%- 9.6% of hospitalized patients with case fatality rates at 5%-20%. On the other hand, the case fatality rate of AKI patients in ICU is as high as 35%-65%. 3 At present, renal replacement therapy (RRT) is the most common treatment used for severe AKI patients in ICU. When the hemodynamics of AKI patients is unstable and suffering from brain edema or acute brain injury, continuous renal replacement therapy (CRRT) is more beneficial than intermittent renal replacement therapy (IRRT).4,5 High-risk bleeding in ICU wards can be caused by numerous factors, including trauma resulting from a cardiac, brain, or abdominal surgery and coagulopathy and thrombocytopenia caused by sepsis or active bleeding.6–8 The use of systemic anticoagulants in patients undergoing CRRT further increases the risk of pre-existing bleeding, but this risk is poorly understood. Therefore, it is essential to understand the proper use of anticoagulants in CRRT.
The mass understanding is believed to be that heparin infusion is low cost, easy to manage and monitor, and is the most commonly used anticoagulant method in blood purification therapy. However, heparin infusion has systemic effects, increases the risk of bleeding, and causes the incidence of heparin-induced thrombocytopenia with life-threatening high-risk complications as high as 10% −30%. 9 Regional citrate anticoagulation (RCA) acts as an anticoagulant in cardiopulmonary bypass is safer than the systemic effect of heparin anticoagulation. 10 Some studies evaluated and compared the efficacy and safety of RCA and heparin anticoagulant therapy, with results showing considerable differences in indicators such as bleeding risk and filter life,11–14 with RCA carrying a prominent advantage. The Kidney Disease Improving Global Outcomes (KDIGO) guidelines also recommend RCA as the first choice for patients who require CRRT. 15 However, due to the complexity of RCA technology and the impact on the internal environment and other issues that have not been thoroughly studied, this has so far not yet been widely used. In conclusion, this study is intended to investigate the efficacy and safety of RCA in CRRT on elderly patients at a high risk of bleeding.
Materials and Methods
General Information
The research conducted is a prospective, single-blind, randomized, controlled clinical study. We selected a total of 31 patients that are at a high risk of bleeding who have received CRRT treatment in the People's Hospital of Suzhou New District from January 2015 to October 2020. Patients were randomly divided into groups namely RCA group (n = 17) and No anticoagulation (NA) group (n = 14). The Ethics Committee of The People's Hospital of Suzhou New District (2021-100) has approved this study with signed informed consent from all associated patients.
Inclusion criteria
(1) all patients were ≥ 65 years old; (2) high-risk of spontaneous bleeding: heparin-related bleeding, prothrombin time (PT) > 18 s, activated partial thromboplastin time (APTT) > 45 s, international normalized ratio (INR) > 1.5, thrombocytopenia caused by anticoagulants, anti-platelets or thrombolytic agents combination therapy (Platelets < 50 × 10 9 /L); (3) within the time frame of 48 h post-surgery; (4) all patients have received CRRT.
Exclusion criteria
(1) presence of contraindications to CRRT; (2) severe hypotension and hypoxemia that cannot be corrected; (3) abnormal coagulation function caused by diseases of the blood system; (4) severe abnormal liver function; malignant tumour complication; (5) sodium citrate allergies; (6) pregnant or lactating women.
Treatment Methods
All patients were treated with continuous venovenous hemofiltration (CVVH), with a controlled 150 to 200 ml/min blood flow velocity. Initially, the RCA group was given 4% RCA at a flow rate of 200 ml/h to reach the 2.5 to 3.5 mmol/L blood citric acid concentration range. Then the patients in the RCA group received a 10% calcium gluconate intravenous infusion. During the treatment, ionized calcium ion (iCa2+) levels after the filter and body were monitored every 4 h. iCa2+ after the filter was maintained at 0.25 to 0.35 mmol/L while levels in the body were at 1.0 to 1.3 mmol/L. NA group: No anticoagulation was performed. Blood gas analysis and routine blood coagulation testing were performed every 4 h before and after treatment in both groups, with blood cells examined daily during treatment.
Observation Indicators and Safety Evaluation
Before and after treatment, 5 mL of venous blood was collected without anticoagulation, with the serum being separated after centrifugation. The serum creatinine (Cr) and blood urea nitrogen (BUN) levels in the two groups were compared using an automatic biochemical analyzer. PT and APTT levels were monitored in both groups. The levels of serum total calcium (tCa), iCa2+, sodium ion (Na+), bicarbonate ion (HCO3−), tCa/iCa2+ ratio, and pH were observed in patients in the RCA group on days 0, 1, 2, and 3 during the treatment. The two groups compared the duration of filter use, the number of filters used within 72 h, and events of filter impairment (filter clotting, conversion to dialysis treatment, radiological assessment interrupted treatment, extracorporeal circulation dysfunction, transfer, other). Clinical outcome measures and safety evaluation included recovery of renal function, bleeding events, citrate accumulation (CA), acid-base imbalance, electrolyte imbalance, red blood cell (RBC) transfusion, and in-hospital mortality.
Statistical Analyses
The data obtained from the experiment were analyzed using SAS 9.1 statistical software. T-test was used to analyze the two groups, and one-way analysis of variance was used for analysis between multiple groups. The results were represented by mean ± standard deviation (SD), and P < .05 was considered a statistically significant difference.
Results
Baseline Clinical Characteristics of Patients in the NA and RCA Groups
Patients were divided into the RCA group (n = 17) and NA group (n = 14) according to whether or not they received regional sodium citrate anticoagulation. There were no statistical differences in baseline characteristics between the two groups (P > .05). The results are presented in Table 1.
Baseline clinical characteristics of patients in the NA and RCA groups.
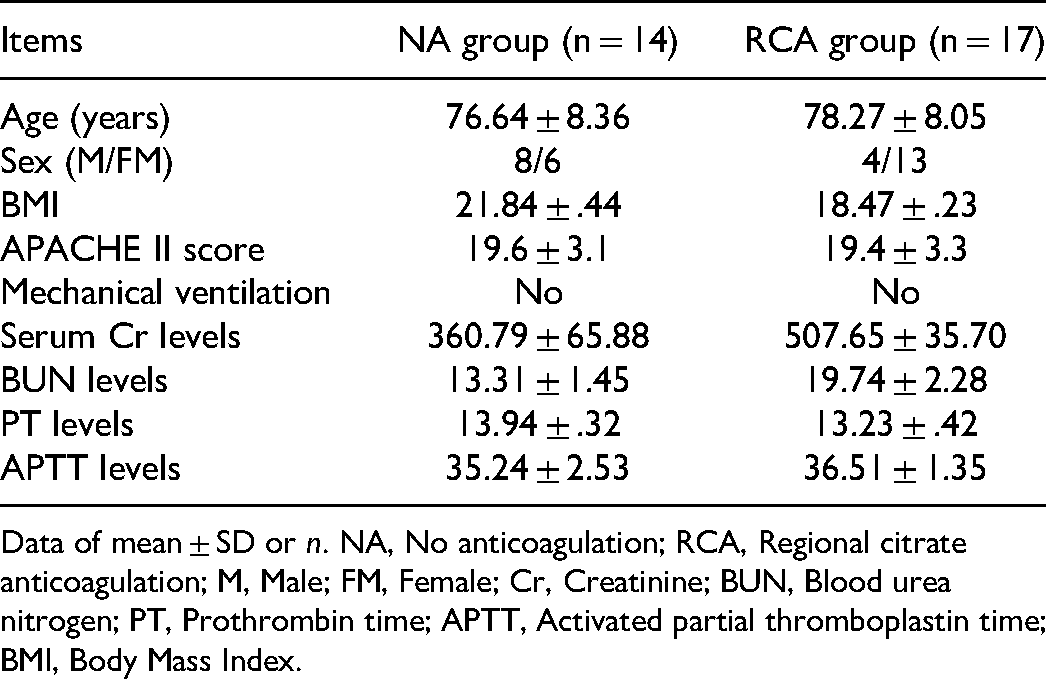
Data of mean ± SD or n. NA, No anticoagulation; RCA, Regional citrate anticoagulation; M, Male; FM, Female; Cr, Creatinine; BUN, Blood urea nitrogen; PT, Prothrombin time; APTT, Activated partial thromboplastin time; BMI, Body Mass Index.
Comparison of Serum Creatinine and Blood Urea Nitrogen Levels in Patients Between NA Group and RCA Group
When compared with before treatment, serum Cr and BUN levels in the two groups notably decreased after treatment. Compared with the NA group, the RCA group Cr and BUN levels were significantly lower after treatment. Results are detailed in Table 2.
Comparison of serum Cr and BUN levels between NA group and RCA group.

Data of mean ± SD, NA, No anticoagulation; RCA, Regional citrate anticoagulation; Cr, Creatinine; BUN, Blood urea nitrogen.
*P < .05 versusbefore treatment.
P < .05 versus NA group.
Comparison of PT and APTT Levels Between NA Group and RCA Group
Compared with the data before treatment, there was no significant difference in PT levels in the NA group post-treatment, but its APTT levels saw a considerable increase. After treatment, APTT and PT levels showed a substantial reduction in the RCA group compared to the NA group (Table 3).
Comparison of serum PT and APTT levels between NA group and RCA group.

Data of mean ± SD, NA, No anticoagulation; RCA, Regional citrate anticoagulation; PT, Prothrombin time; APTT, Activated partial thromboplastin time.
**P < .01 versus before treatment.
P < .01 versus NA group.
Influence of RCA on Electrolyte and Acid-Base Balance in Patients
At 0, 1, 2, and 3 days after treatment, no significant differences in tCa, iCa2+, tCa/iCa2+, HCO3− and pH were detected in the RCA group with levels within the normal range.
Compared with day 0, Na+ levels were signally higher on days 2 and 3, while no marked difference was identified with Na+ levels on day 1. The level of Na+ on days 1, 2, and 3 gradually increased, but the discrepancy was not statistically significant (Table 4).
Influence of RCA on electrolyte and acid-base balance in patients.

Data of mean ± SD, Regional citrate anticoagulation; tCa, total calcium; iCa2+, ionized calcium ion; Na+, sodium ion; HCO3−, bicarbonate ion.
*P < .05 versus Day 0. RCA.
Comparison of Filter use Efficiency Between NA Group and RCA Group
Compared with the NA group, the use time of filters was significantly prolonged in the RCA group. In contrast, the number of filters used within 72 h and the number of filter obstruction events were significantly reduced (Table 5). The proportion of dangerous events after filter use was further analyzed in both groups. Compared with the NA group, the number of patients in the RCA group who were converted to dialysis or had extracorporeal circulation dysfunction lessened significantly. No considerable differences in the number of patients with filter clotting, radiological assessment interrupted treatment, hospital transfer, or other events were observed(Table 6).
Comparison of filter use efficiency between NA group and RCA group.

Data of mean ± SD. NA, No anticoagulation; RCA, Regional citrate anticoagulation.
Comparison of dangerous events after filter use between the NA group and RCA filter.
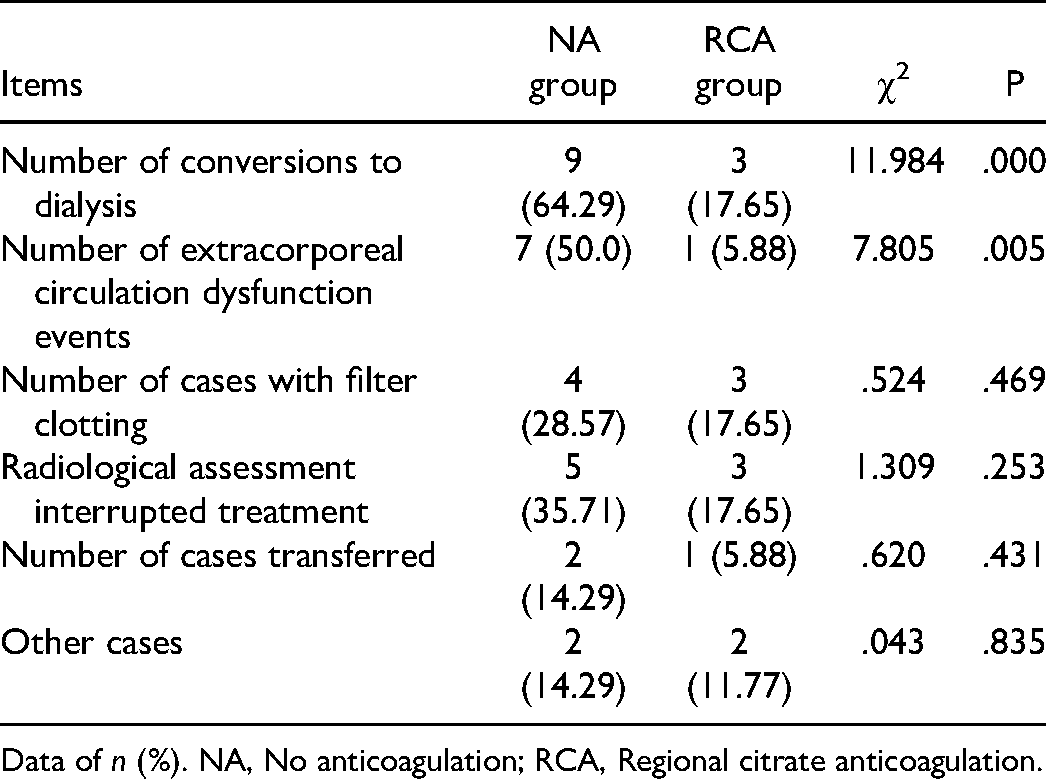
Data of n (%). NA, No anticoagulation; RCA, Regional citrate anticoagulation.
Comparison of Clinical Outcomes and Safety Between the NA Group and RCA Group
Finally, an analysis of clinical outcomes and the safety of the treatment modalities in the two groups was done. The results in Table 7 showed that the recovery of renal function significantly increased in the RCA group compared with the NA group. Bleeding events, RBC transfusion, and in-hospital mortality occurrences reduced significantly (P < .05). There was no significant difference in the number of patients with CA, acid-base imbalance, and electrolyte imbalance between the two groups (P > .05).
Comparison of clinical outcomes and safety between the NA group and RCA group.

Data of n (%). NA, Non-anticoagulation; RCA, Regional citrate anticoagulation; RBC, Red Blood Cell. CA, citrate accumulation.
Discussion
CRRT is a type of continuous blood purification therapy that takes over the function of the damaged kidney and is one of the “three major life support technologies” for critically ill patients. To ensure a good and smooth CRRT therapy operation, we need to provide a proficient anticoagulant effect. For elderly patients with a high risk of bleeding, we are faced with the threat of hemorrhagic complications at any time, which clinically manifests as coagulation disorders, significantly prolonged PT, and APTT significantly reduced fibrinogen or significantly reduced PLT. If systemic anticoagulation (such as heparin) is utilized at this time, the bleeding risk will increase and become life-threatening.11,16 Heparin-free CRRT is a strategy commonly used clinically that avoids heparin anticoagulation caused bleeding risks. However, it may reduce filter life and an increased pipeline replacement frequency and blood purification cost. This increases the economic burden of patients with financial difficulties, accompanied by a reduction in treatment satisfaction. 17 Therefore, when CRRT is used to treat patients with high bleeding risks, developing appropriate anticoagulant regimens is vital.
Studies have found that through close monitoring, timely adjustment of blood calcium ion concentration, and better metabolic capacity of the body's liver, muscle, and kidney, CRRT with RCA has little effect on the body's coagulation system. 18 Patients treated with CRRT using the conventional anticoagulant heparin sodium have reported a 10 to 50% chance of bleeding with bleeding caused mortality rates of about 15%. 19 Citrate is a small anticoagulant molecule with a molecular size of about 191 Da and is usually used as an anticoagulant. 20 ICa2+ is coagulation factor 4, one of the necessary coagulation factors in endogenous and exogenous coagulation pathways. Citrate carries a negative charge and can chelate with Ca2+ to prevent the conversion of prothrombin into thrombin and multiple steps in the coagulation cascade reaction to achieve the purpose of anticoagulation. 21 Several studies have evaluated the efficacy and safety of sodium citrate and heparin in CRRT anticoagulation. It was found that compared with systemic heparin anticoagulation, regional heparin anticoagulation had less influence on the body's blood coagulation system.22,23
Sodium citrate can significantly reduce the incidence of CRRT termination events caused by various reasons, 10 and the bleeding rate of sodium citrate treatment is lower than that of therapy by heparin. 24 In addition, sodium citrate has been shown to extend the service life of filters, reduce the risk of bleeding in patients, reduce catheter infection, and extend catheter life.25–28 However, scholars have also found that the use of citrate in CRRT may lead to the risk of hypernatremia, metabolic alkalosis, and hypocalcemia, so it is necessary to closely monitor electrolytes iCa2+ and acid-base balance throughout the treatment process. For patients with severe liver failure and lactic acidosis, the metabolic capacity of citrate is impaired. Improperly controlled dosage can lead to citrate poisoning, manifest into low systemic iCa2 + circulation, increased serum tCa, metabolic acidosis, and widening the anion gap. However, as long as blood iCa2+ is closely monitored with citrate dosages adjusted in time, these complications rarely occur when citrate is utilized as a regional anticoagulant.29,30 In this study, serum Cr and BUN levels were significantly decreased in both groups after treatment, with levels significantly lower in the RCA group than in the NA group. APTT and PT levels were also reduced dramatically in the RCA group after treatment.
Furthermore, filter use duration was significantly longer after RCA treatment when compared to the NA group. The number of filters used within 72 h, the number of filter dysfunction events, and the number of cases with transfer to dialysis and extracorporeal circulation dysfunction events saw a significant reduction compared with the NA group with a significantly increased renal function recovery the RCA group. Bleeding events, RBC transfusions, and in-hospital mortality were also considerably reduced. The above results showed that the use of RCA has beneficial clinical anticoagulant effects in elderly patients treatment who have a high risk of bleeding in CRRT, showing high safety and efficacy, and laying down the foundation for rapid patient recovery.
In summary, RCA has little effect on systemic coagulation function and does not increase the risk of bleeding. Clinical application of CRRT in critically ill patients with bleeding or at high risk of bleeding is safer with more desirable therapeutic effects. However, the specific mechanism of regional sodium citrate anticoagulation in CRRT for elderly patients with an increased risk of bleeding requires more in-depth research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.