
Abstract
Background
Monitoring of blood coagulation is essential in ECMO patients. We investigated the prevalence of lupus anticoagulant (LA) and its association with coagulation testing and hemostaseologic complications in patients treated with ECMO.
Methods
This is a retrospective analysis including adult patients who received ECMO at a medical intensive care unit at the Medical University of Vienna. The primary outcome was the prevalence of LA. Secondary outcomes included conditions associated with LA positivity, rates of bleeding and thromboembolic events, as well as the proportions of aPTT and antiXa measurements within the target range.
Results
Between 2013 and 2021 193 patients received ECMO, in 62 (32%) of whom LA diagnostics were performed. Twenty-two (35%) patients tested positive. LA positive patients had more frequently received VV ECMO (77.3% vs 34.3%; p = 0.002), were more frequently diagnosed with viral respiratory infections (SARS-CoV2: 45.5% vs 20%; p = 0.041, influenza virus: 22.7% vs 0%; p = 0.003), had a longer ECMO treatment duration (25 vs 10 days; p = 0.011) and a longer ICU stay (48 vs 25 days; p = 0.022), but similar rates of bleeding and thromboembolic events.
Keywords
Background
During extracorporeal membrane oxygenation (ECMO), human blood is exposed to large artificial surfaces, which promotes clot formation and requires systemic anticoagulation. 1 Anticoagulation in ECMO patients is critical to ensure a tightly regulated balance between clotting and bleeding, warranting regular monitoring of anticoagulation targets. Activated partial thromboplastin time (aPTT) is most commonly used to monitor anticoagulation during ECMO. 2 In ECMO patients, prolongation of aPTT can be caused either by anticoagulation with unfractionated (UFH), low molecular weight heparins (LMWH)3,4 or direct thrombin inhibitors 5 or by several confounding conditions. 6 The latter include a deficiency of coagulation factors or the presence of lupus anticoagulant (LA) antibodies. 7
Lupus anticoagulant belongs to the family of antiphospholipid antibodies (aPL), a heterogeneous group of antibodies that directly target proteins with high affinity for negatively charged phospholipids, including coagulation factors and plasma proteins.8,9 In vivo, the presence of LA may be associated with an increased tendency to develop thrombosis. 10 To date, there are no data on the occurrence of LA during ECMO treatment.
In this context, we performed this study to determine (i) the prevalence of LA in patients during ECMO, to address the relevance of its confounding effect on aPTT-guided anticoagulation, (ii) assess factors associated with LA-positivity and (iii) investigate whether LA-positivity was associated with thromboembolic events.
Methods
Study Design and Patients
This retrospective study was conducted at a medical Intensive Care Unit (ICU) at a European tertiary care center. Only adult patients (≥18 years) were included. Medical records were screened for patients receiving ECMO. Data were extracted from a prospectively compiled ECMO registry.
All patients received anticoagulation with continuously administered UFH (maintenance dose of 7.5–20 IU/kg/h). In patients with confirmed heparin-induced thrombocytopenia (HIT), Argatroban was used (Starting dose: 0.3 µg/kg/min). Anticoagulation with UFH and Argatroban was monitored by aPTT-A (aPTT-A target: 1.5–2.5× baseline or 50–60 s; aPTT-A reference range: 27–41 s) and a coagulometric antiXa assay (antiXa target 0.2 to 0.3 IU/mL) for patients receiving UFH.
Testing for LA was prompted at the discretion of the treating intensivist during ECMO. When requested to determine LA, aPTTs (LA, actin-FS, A (standard)) and dilute Russell's viper venom time (dRVVT) with an antiheparin agent were performed as screening tests. If the result was indicative of LA, a mixing test and confirmatory tests to assess phospholipid dependence were subsequently added in a stepwise diagnostic procedure. 11 The respective confirmatory tests were chosen based on the initial pathologic screening test, ie aPTT or dRVVT based. The confirmatory tests are insensitive to heparin levels up to 1 IU/ml and 0.8 IU/ml, respectively.
Test reagents for aPTT-A, aPTT-LA, dRVVT and the AntiXa assays from Diagnostica Stago (Asnieres, France) and for aPTT-actin FS from Siemens (Marburg, Germany) were used. For mixing studies the ‘Pool Norm’ from Diagnostica Stago (Asnieres, France) was used. All analysis were performed with the STAR-Max2 (Diagnostica Stago, Asnieres, France).
Patients were grouped as LA positive if they had a prolongation of lupus sensitive clotting times and a positive confirmatory test. LA before and after ECMO were not determined. Lupus anticoagulant positive patients received no specific treatment, but monitoring of anticoagulation in these patients was performed using tests not sensitive to presence of LA, ie the AntiXa assay for patients receiving UFH and the hemoclot assay for patients receiving direct thrombin inhibitors in case of HIT.
With regard to complications, this study distinguished between bleeding and thromboembolic complications. Bleeding included an increased bleeding tendency from puncture and surgical sites, organ bleeding (gastrointestinal, pulmonary and intracranial bleeding, macrohematuria) and hemothorax. Thromboembolism was defined as membrane lung clotting or pump thrombosis necessitating system exchange, as well as thrombus formation in the cardiovascular system (at the cannulation site, pulmonary embolism, ischemic stroke).
This study was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki.
Outcomes
The primary outcome was the prevalence of LA in patients receiving ECMO. Secondary outcomes were to determine the impact of the presence of LA on clinically significant complications and monitoring of anticoagulation during ECMO, and to identify factors contributing to the development of LA.
Statistical Analysis
Variables are presented as absolute values (n), relative frequencies (%, with 95% confidence interval (CI)), and median with interquartile range (IQR). The primary outcome was assessed descriptively. The study population was categorized into positive, negative, or untested according to LA status. Secondary outcomes were assessed descriptively. Between group comparisons were performed by using the t-test, the Mann-Whitney U test and χ2- test, respectively. Between group comparisons for time-dependent events were analyzed with the log-rank test.
For data analysis, we used SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) and figures were modified with RStudio (“Ghost Orchid” Release (fc9e2179, 2022-01-04) for macOS). A two-sided p-value <0.05 was considered statistically significant.
Results
Between January 2013 and August 2021, 193 patients received ECMO. LA diagnostics were performed in 62 patients (32%). Patients were predominantly male (n = 38; 61.3%), and aged 53 years (IQR 42–61). The median ECMO runtime was 5 days (IQR 7–31), 33 patients (53.2%) were successfully discharged from the ICU and 28 patients (45.2%) were successfully discharged from the hospital. Heparin-induced thrombocytopeniawas documented in three of the 62 patients (LA positive n = 1). Baseline characteristics are shown in Table 1.
Baseline Characteristics and Outcome.

P-values represent between group comparisons of LA negative and LA positive patients.
Abbreviations: aPTT, activated partial thromboplastin time; ECMO, Extracorporeal membrane oxygenation; IQR, interquartile range; PT, prothrombin time; SAPS II, Simplified Acute Physiology Score II.
aNumbers display patients with at least one thromboembolic/bleeding event.
Of the 62 patients tested, 22 (35.5%; CI 23.2–47.7) were LA positive, with a median determination on the third ECMO day (IQR 1–12). Thirty five patients tested negative for LA and in five cases no determination was possible due to preanalytical errors. In 42 of these patients, LA diagnostics were performed within the first seven ECMO days. Thirty three point three percent of these patients (n = 14) tested positive. The remaining 20 patients were tested after ECMO day seven, with 40% (n = 8) testing positive. The rate of positive LA testing was not different between tests performed before and after ECMO day seven (p = 0.608). LA testing was performed on day 10 (IQR 5–21) after ICU admission in LA positive patients and on day four after ICU admission in LA negative patients (IQR 2–13; p = 0.026).
There were no significant differences with respect to bleeding and thromboembolic complications. More patients with LA had one or more thromboembolic events (n = 13/22; 59.1%) compared to LA negative patients (n = 17/35; 48.6%; p = 0.439; Table 1). Testing for LA status was performed prior to the first thromboembolic event in 70% of cases. Thromboembolism-free intervals were longer in LA positive patients (33 (CI 15–50) versus 20 (CI 10–29) days; p = 0.58), but did not reach statistical significance (Figure 1).

Survival without thromboembolic events compared between LA subgroups.
Less patients with LA had one or more bleeding complications (n = 8/22; 36.4%) compared to LA negative patients (n = 15/35; 42.9%; p = 0.627; Table 1, Table 2 and Table 3). Similarly, the time to the first bleeding complication was shorter in LA negative patients (32 (CI 17–47) versus 93 (CI 60–127) days; p = 0.33; Figure 2).

Survival without hemorrhagic events compared between LA subgroups.
Bleeding Complications – BARC Classification.

Abbreviations: BARC, bleeding academic research consortium; LA, lupus anticoagulant.
Bleeding Complications – Localization.
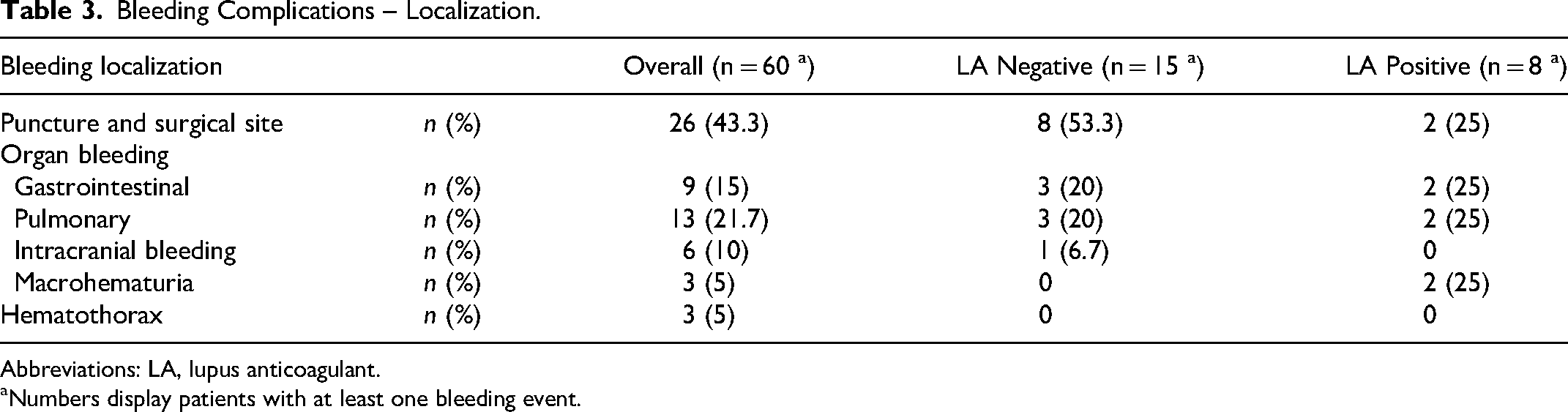
Abbreviations: LA, lupus anticoagulant.
Numbers display patients with at least one bleeding event.
LA positive patients received a median of 219 IU/kg UFH per day (IQR 145-327). LA negative patients received a median of 212 IU/kg UFH per day (IQR 167-316; p = 0.78). Regarding aPTT, the proportion of measurements within the target range per patient was 22% (IQR 14%–36%) in the LA positive group and 29% (IQR 14%–38%) in the LA negative group (p = 0.451). Concerning antiXa, the proportion within the target range per patient was 25% (IQR 6%–48%) in the LA positive group and 13% (IQR 0%–36%) in the LA negative group (p = 0.066).
The prevalence of LA was higher in patients on VV ECMO (n = 17; 77.3%; p = 0.002; Table 1). 17 patients with VV-ECMO (n = 17/29; 58.6%) and three patients with VA-ECMO (n = 3/19; 15.8%) were LA positive. The remaining two LA positive patients had a different configuration or a configuration change. The presence of LA was associated with a higher number of viral respiratory tract infections as underlying disease: 10 of the 22 LA-positive patients (45.5%; p = 0.041) were infected with SARS-CoV-2 and 5 (22.7%; p = 0.003) with influenza virus. Data on relationship between ECMO type and duration and viral respiratory tract infections is shown in Table 4.
Relationship Between ECMO Type and Duration and Viral Respiratory Tract Infections.

Abbreviations: ECMO, extracorporeal membrane oxygenation; IQR, interquartile range; VA, venoarterial; VV, venovenous.
In addition, LA positive patients had a significantly longer ECMO treatment duration (25 days; p = 0.011) and ICU length of stay (48 days; p = 0.022). There was no difference in ICU and hospital survival with respect to LA status.
Discussion
The present study provides information on the prevalence of LA in ECMO patients, associated factors, and potential implications for anticoagulation monitoring.
In our study cohort, (i) one-third of patients who underwent testing were positive for LA during ECMO, (ii) LA was more common in patients on VV ECMO and with viral respiratory infections and was associated with longer ECMO duration and ICU stay, and (iii) LA positivity was not associated with thromboembolic complications.
Prevalence of LA in ECMO Patients
The aPTT is the most commonly used test to monitor the anticoagulant effect of UFH. However, the aPTT can be prolonged by various confounding factors such as the presence of a LA, factor XII deficiency or sepsis.12,13 There are limited data on the prevalence of LA in ICU patients and especially in ECMO patients. Two retrospective studies report a prevalence of LA of 35% and 53% in critically ill COVID-19 14 and non-COVID-19 patients, respectively. 15 This is consistent with our cohort, in which one-third of patients tested positive for LA. According to our and previous data, patients show LA within the first two weeks of their ICU stay. 15 Patients were not routinely tested for persistence of LA-positivity, which therefore needs to be determined in future studies. Recent data from COVID-19 patients showed, that the vast majority of patients was negative at retesting after 1 16 or 3 to 6 months, 17 which suggests that LA positivity is a transient phenomenon during viral infection.
Clinical Relevance, Underlying Diseases and Complications
In our study, a risk factor for development of LA was infection, mostly caused by viral diseases, promoting inflammation and probably antibody production within the host. In COVID-19 patients, molecular mimicry, neoepitope formation and phosphatidylserine exposure have been described as underlying mechanism for LA positivity.18,19 Previous data on critically ill patients described sepsis and requirement of vasopressors as risk factors for development of LA likewise highlighting infection and inflammation in the context of LA-positivity. 15
Patients positive for LA had a longer ECMO duration and more likely received VV ECMO compared to VA ECMO. The fact that ECMO patients with viral pneumonia have a longer ECMO duration is consistent with data of the Extracorporeal Life Support Organization (ELSO) Registry International Report 2016. 20 Thus, we interpret the longer ECMO duration in LA positive patients is likely a consequence of the underlying disease and not LA positivity.
In our cohort, there was no significant difference in thromboembolic events between LA positive and negative patients. LA positive patients had a slightly higher rate of at least one thromboembolic event, which may indicate a prothrombotic state. However, the literature indicates that the isolated presence of LA antibodies does not promote thrombosis unless accompanied by antibodies to 2-glycoprotein I, pro-thrombin, or cardiolipin, which were not tested in our study.21–23 Therefore, we cannot draw any conclusions about the effects of LA on thrombotic complications (or bleeding).
LA prolongs aPTT not related to an anticoagulatory effect. 7 This becomes critical, when only aPTT is used to monitor anticoagulation during ECMO therapy, as it may falsely suggest anticoagulation within preset target values. In this context, in patients with unexplained aPTT prolongation, testing for LA and other confounding factors, including FXII deficiency, should be prompted. According to our data, this should be done in a low-threshold manner, especially in patients on VV ECMO with ARDS due to viral diseases (Influenza and COVID-19). However, intensivists need to make sure, that LA testing during anticoagulation is performed with test systems unaffected by heparin (ie using reagents with heparin neutralizers) to obtain reliable results. 24
Further monitoring of anticoagulation in LA-positive patients should rely on tests unaffected by LA-positivity, including AntiXa assays for patients receiving UFH and AntiIIa assays for patients receiving DTIs. In our patient cohort, the UFH doses administered did not differ between the study groups. This may be explained by the established concomitant use of antiXa levels at our center to monitor anticoagulation. Accordingly, our data showed that in LA positive patients, therapeutic target values for aPTT are reached less frequently, whereas values for antiXa are reached more frequently. The high prevalence of LA in our study supports the use of at least two different testing systems to monitor anticoagulation in ECMO patients, as suggested by the ELSO guidelines.
Based on the hypothesis-generating data presented, future studies need to answer the following questions: I) Determination of the actual prevalence of LA positivity by continuous consecutive inclusion of ECMO patients to avoid selection bias; II) Assessment of the incidence and persistent positivity of LA antibodies by longitudinal sampling and long-term follow-up of LA positivity with multiple tests per patient, ideally even before ECMO therapy; and III) Evaluation of the influence of LA positivity on clinically relevant endpoints such as bleeding and thrombosis by analysis of larger sample sizes.
Limitations
The major limitations of this study result from the retrospective study design and the limited sample size. Interpretation of the results must take into account that LA was not routinely determined in all patients which introduced a selection bias. LA status was not available before and after ECMO. Therefore, we can not draw a conclusion regarding incidence and persistence of LA positivity.
LA testing was performed in patients who were continuously administered UFH. According to current guidelines, LA diagnosis should be performed after discontinuation of anticoagulation, 11 which, however, is not possible during ongoing ECMO therapy. However, De Kesel et al showed that by using the three-step procedure to determine LA, misclassification in the aPTT test system caused by prolongation of the aPTT by UFH is avoided. 25 The three-step procedure includes mixing studies that help to eliminate a heparin effect and thus help eliminate it (in patient plasma where heparin levels are just above the therapeutic range), 26 which thereby suggests valid test results in our patient collective.
History of prior coagulation disorders was only available from medical charts and no further routine clarification was performed in LA positive patients either, which is why no information is available in this regard and no conclusions can be drawn.
Conclusion
In this cohort, one-third of patients tested positive for LA during ECMO. LA should be considered as a potential confounder when using aPTT for monitoring of anticoagulation. Several conditions were observed more frequently in ECMO patients with LA, including viral infections, treatment with VV ECMO, longer ECMO duration, and longer ICU stay. However, larger studies are needed to confirm the observed results and to determine the impact of LA on complications during ECMO therapy to ultimately optimize the management of coagulopathy in these particular critically ill patients.
Essentials
In our study cohort, one-third of patients developed LA during ECMO.
LA was more common in patients on VV ECMO and in patients with viral respiratory infections.
LA was associated with longer ECMO duration and ICU stay.
LA positivity was associated with a lower proportion of aPTT measurements in the target range.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Medical Scientific Fund of the Mayor of the City of Vienna.