
Abstract
Hypoxemia is a clinical characteristic of pulmonary embolism (PE). Hypoxemia is associated with variations in serum prostate-specific antigen (PSA) levels. Thus, the present study aimed to determine serum PSA levels in patients with PE, which may be helpful in improving clinical evaluation in screening for prostate diseases in those with PE. Clinical data from 61 consecutive male patients with PE and 113 age-matched healthy male controls were retrospectively analyzed. The pulmonary artery obstruction index (PAOI) was used to evaluate the pulmonary embolic burden. Compared with healthy controls, serum total PSA (tPSA) levels were significantly increased (P = .003), and free PSA (fPSA)/tPSA ratio was significantly decreased in patients with PE (P < .001). There was no significantly difference in serum fPSA levels between patients with PE and healthy controls (P = .253). A significant positive association was observed between serum tPSA levels and PAOI in patients with PE (β = .270, P = .036). Multivariable linear regression analysis revealed that serum tPSA levels were independently associated with PAOI in patients with PE (β = .347, P = .003). Serum tPSA levels were higher in male patients with PE than those in healthy controls, but fPSA was not affected. These findings highlight that PE may elevate serum tPSA levels, and that measures of tPSA should be interpreted with caution in screening for prostate diseases in patients with PE.
Keywords
Introduction
Prostate-specific antigen (PSA) is a serine protease produced by prostate epithelial cells
It has been suggested that elevated serum PSA levels are associated with ischemic conditions, including coronary artery disease, cardiogenic shock, and prolonged cardiopulmonary resuscitation.7–9 Notably, hypoxemia increases serum PSA levels during acute exacerbation of chronic obstructive pulmonary disease (COPD). 10 Pulmonary embolism (PE) is caused by partial or complete obstruction of the pulmonary artery 11 and, as a pulmonary thromboembolic disease, PE is often involved in hypoxemia. 12 As such, we aimed to investigate serum PSA levels in patients with PE, which may be beneficial for improving the clinical evaluation of prostate diseases screening in individuals with PE.
Methods
Patients and Controls
The medical records of 61 consecutive male patients with PE were reviewed retrospectively from the Affiliated Hospital of Youjiang Medical University for Nationalities, and 113 consecutive, age-matched, healthy males who visited the Affiliated Hospital of Youjiang Medical University for Nationalities for health checkup were included as controls retrospectively. The diagnosis of PE was confirmed in all patients using computed tomography pulmonary angiography (CTPA), 13 all of whom underwent a thorough evaluation for pulmonary disease. Patients with prostate diseases, coronary heart disease, renal or hepatic disturbances, malignant tumors, or urinary tract infections were excluded. Furthermore, patients with a history of prostate biopsy, urinary tract treatment, and medical or surgical treatment of the prostate were also excluded. This study was approved by the Ethics Committee of the Affiliated Hospital of Youjiang Medical University for Nationalities and conformed to the principles of the Declaration of Helsinki. Requirements for informed consent were waived by the Ethics Committee of the Affiliated Hospital of Youjiang Medical University for Nationalities due to the retrospective design of the study.
Data Collection
Clinical data were extracted from electronic medical records. Clinical and demographic characteristics, disease history, laboratory investigations, and imaging examination results were obtained upon admission. Blood samples were collected for laboratory investigations, which included
Sample Size and Power
The sample size required for this study was determined using PASS version 21.0.3. The sample size was calculated using the primary variable, tPSA, in patients with PE and controls. It was estimated that 61 patients and 113 controls would be required to achieve 90% power to detect differences.
Pulmonary Artery Obstruction Index (PAOI)
In this study, the PAOI was used to assess the pulmonary embolic burden. The PAOI was calculated in patients with PE after CTPA examination. The PAOI is based on the degree of obstruction and location of the thrombus in CTPA results. 14
Statistical Analysis
Continuous data are expressed as median (interquartile range) for non-normally distributed data, whereas categorical data are expressed as frequency (percentage). Differences in continuous variables between the two independent groups were examined using the Mann–Whitney U test. Normal transformation of the dependent variable was performed before univariable and multivariable linear regression analyses. Univariable linear regression analysis was used to assess whether PSA-related parameters were associated with age, body mass index (BMI), histories of smoking, LEDVT, and COPD, and LVEF, PAOI, and
Results
Features of Patients With PE and Controls
Patient and healthy control characteristics are summarized in Table 1. Results of analysis revealed that serum tPSA levels were significantly elevated in patients with PE compared with healthy controls (P = .003), and that the fPSA/tPSA ratio was significantly reduced in patients with PE compared with healthy controls (P < .001). However, serum fPSA levels were not significantly different between patients with PE and healthy controls (P = .253).
Main Clinical Features in Patients With PE and Healthy Controls.
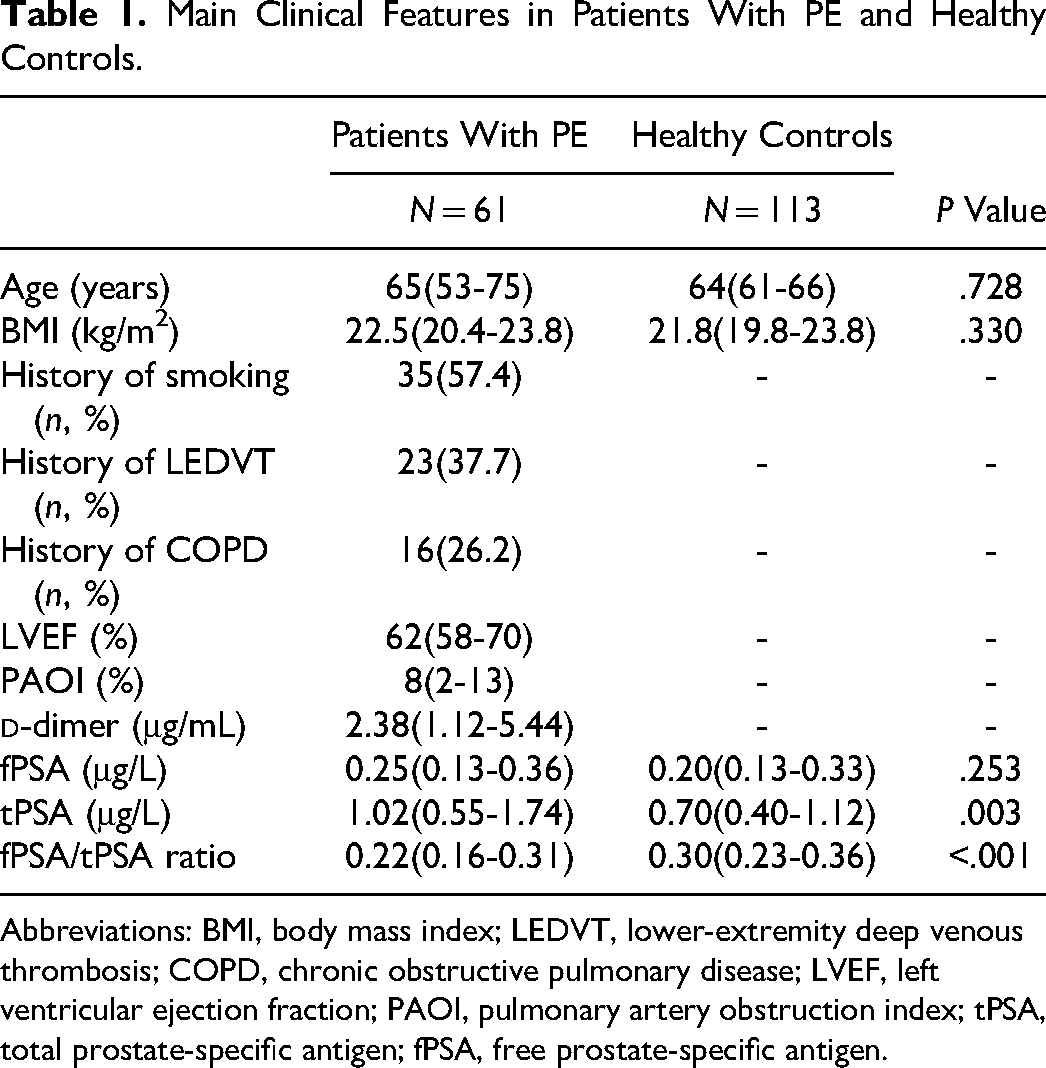
Abbreviations: BMI, body mass index; LEDVT, lower-extremity deep venous thrombosis; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; PAOI, pulmonary artery obstruction index; tPSA, total prostate-specific antigen; fPSA, free prostate-specific antigen.
Variables Affecting PSA-Related Parameters in Patients With PE
Results of univariable linear regression analysis of PSA-related parameters and clinical variables in patients with PE are summarized in Table 2. Serum tPSA levels were significantly and positively associated with age (β = .469, P < .001), history of COPD (β = .305, P = .017), and PAOI (β = .270, P = .036) in patients with PE. Serum fPSA levels were significantly and positively associated with age (β = .333, P = .009) and history of COPD (β = .267, P = .038) in patients with PE. A significant negative association between fPSA/tPSA ratio and age was observed in patients with PE (β = −.282, P = .028). However, both serum fPSA levels (β = .219, P = .090) and fPSA/tPSA ratio (β = −.125, P = .338) had no significant association with PAOI in patients with PE.
Univariable Linear Regression Analysis Between PSA-Related Parameters and Clinical Variables in Patients With PE.
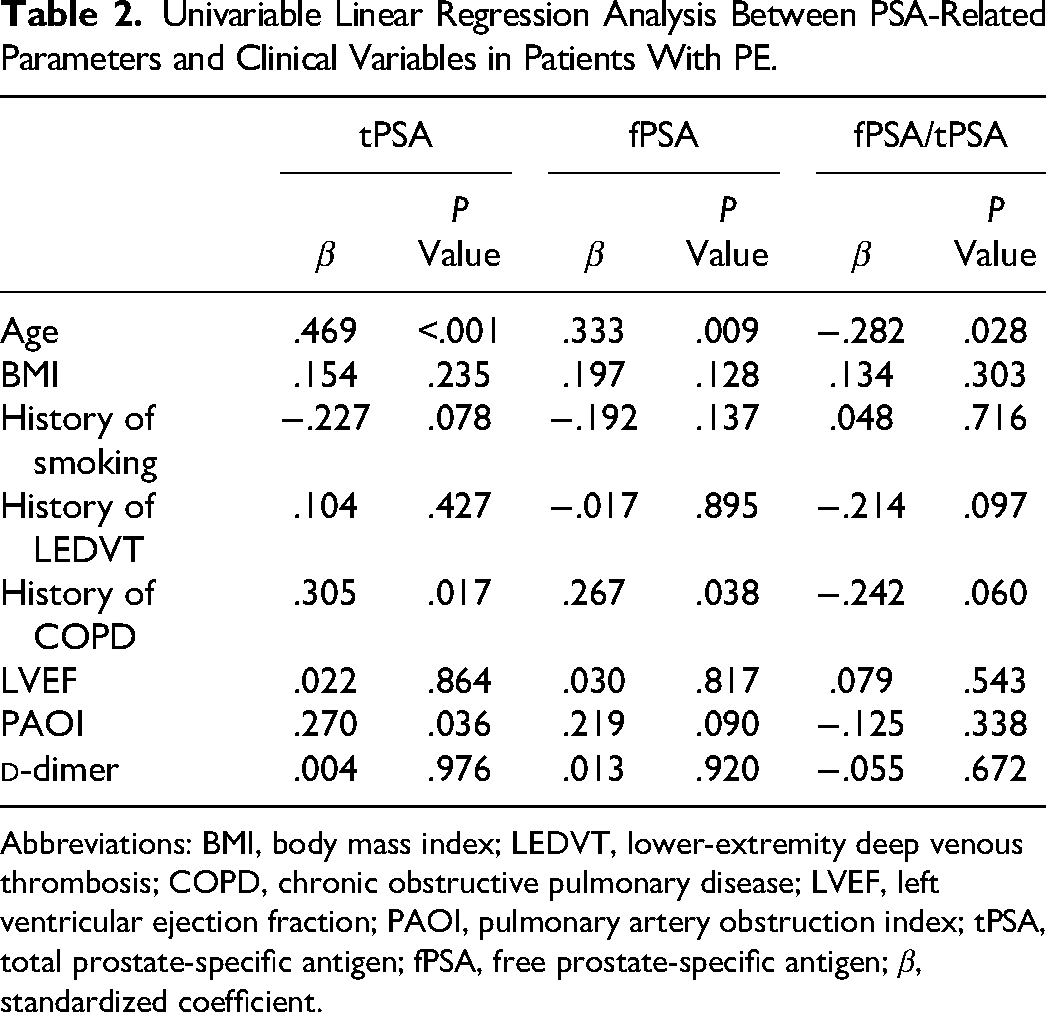
Abbreviations: BMI, body mass index; LEDVT, lower-extremity deep venous thrombosis; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; PAOI, pulmonary artery obstruction index; tPSA, total prostate-specific antigen; fPSA, free prostate-specific antigen; β, standardized coefficient.
Independent Factors Associated With PSA in Patients With PE
Serum tPSA levels were significantly associated with PAOI in patients with PE in univariable linear regression analysis; as such, after adjusting for potential confounding factors, multivariable linear regression analysis revealed that serum tPSA levels were independently associated with PAOI in patients with PE (β = .347, P = .003), and that increase in serum tPSA levels was also independently associated with history of smoking (β = −.291, P = .017), and history of COPD (β = .339, P = .015) in patients with PE.
Discussion
The present study examined serum PSA levels in males with PE. Results suggested that serum tPSA levels were elevated in patients with PE compared with healthy controls and that serum tPSA levels were independently associated with histories of smoking and COPD in these patients. Importantly, a significant positive association between serum tPSA levels and PAOI was observed in patients with PE after adjusting for underlying confounding factors in multivariable linear regression analysis, indicating that pulmonary embolic burden increases serum tPSA levels in patients diagnosed with PE.
Prostatic ischemia damages epithelial cells of the prostate, resulting in elevated serum PSA levels. 15 It has been widely reported in the literatures that serum PSA levels are associated with ischemic conditions.7–9 Hypoxemia is more common in patients with PE due to impaired hemodynamics, gas exchange, and mechanical capacity of the lungs. 12 An association between hypoxemia and elevated serum PSA levels has been demonstrated in patients with acute exacerbations of COPD. 10 It has been highlighted that hypoxia can induce the expression of PSA in human prostate carcinoma cells. 16 It has also been reported that hypoxia facilitates PSA transcription by inducing histone acetylation of PSA enhancers. 17 Moreover, hypoxia increases the androgen receptor-induced promoter activity of the human PSA gene. 18 Therefore, acute hypoxemia may promote the expression and release of PSA in prostatic epithelial cells and elevate serum tPSA levels in patients with PE.
Elevated serum tPSA levels may not only be explained by hypoxemia but also by systemic inflammation, which may also contribute to increased serum PSA levels in patients with PE. Systemic pro-inflammatory cytokines are critical factors in acute PE. 19 The systemic immune inflammatory index, as an inflammatory marker, is a predictor of disease severity in patients with acute PE, and serum C-reactive protein (CRP) is independently associated with massive acute PE. 19 Ma et al suggested that increased serum CRP was a useful screening marker for patients with PE. 20 Therefore, these studies support the possibility that a systemic inflammatory cascade facilitates the development of PE. Interesting, a positive association between serum PSA levels and systemic inflammatory markers has been demonstrated in healthy population. 21 Similarly, systemic inflammatory markers are associated with elevated serum PSA levels in males without known prostatic diseases. 22 Serum PSA levels have been suggested to be positively correlated with CRP levels in the general population. 23 These evidences hence suggest that systemic inflammation may increase serum PSA levels.
In this study, we observed increased serum tPSA levels in patients with PE, but not serum fPSA. When PSA, a kallikrein-like serine protease, is secreted by prostate epithelial cells into the peripheral circulation and rapidly binds to protease inhibitors, primarily alpha1-antichymotrypsin, and a fraction is inactivated by proteolysis and circulates as fPSA. 24 Protease activity has been implicated in the pathogenesis of thrombosis, and proteolysis is associated with the regulation of blood coagulation function.25,26 Thus, abnormal proteolysis may inhibit the formation of fPSA in patients with PE.
Our study also found a significant association between elevated serum tPSA levels and a history of COPD in patients with PE, some of whom may experience more severe hypoxia, which may further increase tPSA levels. Li et al 27 found an inverse association between serum tPSA and smoking. Results of the current study confirmed that smoking may reduce serum tPSA levels in patients with PE. This may be related to the toxic effects of harmful cigarette substances on prostate epithelial cells.
The present investigation had several limitations, the first of which was its small sample size. Second, this study did not directly assess prostate volume in patients with PE. However, we adjusted for age and BMI in the multivariate analysis to minimize the effects of prostate volume on serum PSA levels because age and BMI are closely associated with prostate volume.28,29 Third, serum PSA is also expressed in females 30 ; however, the serum PSA levels were not measured in female patients with PE. Fourth, we did not examine serum PSA levels in patients with PE after treatment.
Conclusion
In summary, elevated serum tPSA levels were observed in male patients with PE compared with healthy controls; however, fPSA was not affected, suggesting that PE may increase serum tPSA levels and that measures of tPSA should be interpreted with caution for prostate disease screening in patients with PE. However, further investigations with larger sample sizes are needed to confirm these findings.
Footnotes
Availability of Data and Material
The data can be obtained by corresponding author upon reasonable request.
Consent to Participation
Informed consent was waived by the Ethics Committee of the Affiliated Hospital of Youjiang Medical University for Nationalities due to the retrospective nature of the study.
Consent for Publication
All authors agreed with publish this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of the Affiliated Hospital of Youjiang Medical University for Nationalities, and conformed to the principles of the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.