
Abstract
The presence of both atrial fibrillation (AF) and heart failure (HF) increases the risk of an ischemic cerebrovascular event (CVE) by roughly fivefold. The HATCH score is a score used to predict new-onset AF. Although there are some differences, it contains risk factors similar to the CHA2DS2-VASc score. Our study aimed to investigate the relationship between the HATCH score and ischemic CVE. This retrospective study obtained data from 1719 HF patients between 2015 and 2022. About 673 patients with AF were included in the study. In the univariate and multivariate Cox regressions, we found that CHA2DS2-VASc and HATCH scores were independent predictors of ischemic CVE (
Introduction
Heart failure (HF) and atrial fibrillation (AF) are common cardiovascular diseases in daily life. Both diseases have similar risk factors that can be modified, such as atherosclerosis, hypertension (HT), diabetes mellitus (DM), and myocardial ischemia, and non-modifiable, such as age and gender. Although they are two separate diseases, they can often coexist and aggravate the clinical situation. 1 Undoubtedly, ischemic cerebrovascular event (CVE) is one of the negative consequences of the coexistence of two diseases. 2 Ischemic CVE is a common cause of death and disability in adults. 3 Research has concluded that the presence of both AF and HF raises the risk of ischemic CVE by a factor of approximately five. 4 Patients who recover from ischemic CVE are more likely to experience ischemic stroke again. 5 Even if patients experience a transient ischemic attack (TIA) or minor ischemic stroke, they may experience recurrent ischemic CVE, increasing the likelihood of poor outcomes. 6 Oral anticoagulants (OACs) have been identified as the main treatment strategy for preventing ischemic complications, including CVE, in AF patients. OACs reduced the risk of stroke by 64% and the mortality rate by 26.1%, although they slightly increased the risk of bleeding. 7 Different scoring systems have been developed for ischemic and cardiovascular complications resulting from AF. 8 The CHA2DS2-VASc score identifies patients at high risk of ischemic complications in AF and prescribes OACs to protect them from ischemic complications. 9 OACs are generally recommended for those with risk factors for ischemic stroke with a CHA2DS2-VASc score of 2 or higher. 10 The HATCH score is a predictor of new AF and was used to assess the probability of permanent AF. 11 The HATCH score is a score that includes parameters for HT, age, TIA or ischemic CVE, chronic obstructive pulmonary disease (COPD), and HF. While the predictive role of the CHA2DS2-VASc score in adverse ischemic events has been proven, 12 it is not yet clear on the ischemic CVE predictive role of the HATCH score, which includes similar risk factors as the CHA2DS2-VASc score. Our study aimed to examine the relationship between HATCH and CHA2DS2-VASc scores and ischemic CVE.
Materials and Methods
Study Design and Patient Selection
This study reviewed the retrospective records of 1719 HF patients who applied to Erzurum Regional Training and Research Hospital between 2015 and 2022. Data on 673 patients with both HF and AF were obtained. Patients under 18 years of age, with liver cirrhosis, heart transplant history, acute coronary syndromes, and malignancy were excluded from the study. The CHA2DS2-VASc score and the HATCH score were calculated for the patients. This study was performed in accordance with the Declaration of Helsinki and with the approval of the local ethics committee. Previous medical history, drug use history, clinical and demographic characteristics, and hematological and biochemical parameters of the patients were recorded in electronic medical records.
Definitions
Computed tomography and/or Magnetic resonance imaging data were used to diagnose ischemic CVE. 13 A history of coronary artery disease (CAD) was defined as patients with invasive or non-invasive imaging studies showing evidence of coronary artery disease. HT was defined as systolic blood pressure > 140 mm Hg and/or diastolic blood pressure > 90 mm Hg or an antihypertensive medication. 14 The definition of DM was determined according to American Diabetes Association guidelines. 15
Risk Scores
The HATCH score was obtained by assigning one point each for patients over 75 years of age, HT, and COPD, and two points each for Previous ischemic CVE or TIA and HF. 11
The CHA2DS2-VASc score was calculated by giving one point each for age 65–74, HT, DM, HF, CAD, female gender, and vascular disease including peripheral arterial disease, and two points each for a previous ischemic CVE or TIA, age 75 and over. 9
Statistics
Data were analyzed using the SPSS 22.0 version (IBM, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation or median (interquartile range), and categorical variables were expressed as percentages. Continuous variables fit the normal distribution and were determined using the “Kolmogorov–Smirnov” test. Continuous variables were compared using “Student's t-test” and “Mann–Whitney U test” as appropriate. Categorical variables were compared using the “chi-square” test. The Cox regression model was performed to find independent predictors of ischemic CVE, and scores that were significant in univariate analysis were included in the regression model. The receiver operating characteristics (ROC) curve analysis was performed to determine scoring systems’ sensitivity and specificity values in predicting ischemic CVE. Variables were considered statistically significant when the P value was < .05.
Results
A total of 673 patients with HF and AF who applied to our hospital between 2015 and 2022 were included in the study. The mean age of the patients was 72.66 ± 10.24, and 43.2% (291 patients) were male. The mean follow-up period was 75.33 ± 20.06 months. HT, DM, CAD, and COPD were 86.8% (584 patients), 19% (128 patients), 56.5% (380 patients), and 28.1% (189), respectively. A previous history of ischemic CVE was found in 3.7% (25 patients). The mean ejection fraction (EF) was 48 ± 13.12%. In the general population studied, the mean CHA2DS2-VASc score was 4 ± 1.2, and the HATCH score was 3 ± 0.9. The CHA2DS2-VASc and HATCH score distributions of the patients are shown in Figure 1. While 70% (471 patients) of the patients were using direct oral anticoagulants, 21.5% (145 patients) were using acetylsalicylic acid, and 10.7% (72 patients) were using clopidogrel. In our study, ischemic CVE occurred in 5.8% (39 patients) during follow-up. In patients with ischemic CVE, the CHA2DS2-VASc score was 6.09 ± 1.33; the HATCH score was 5.27 ± 0.66 (
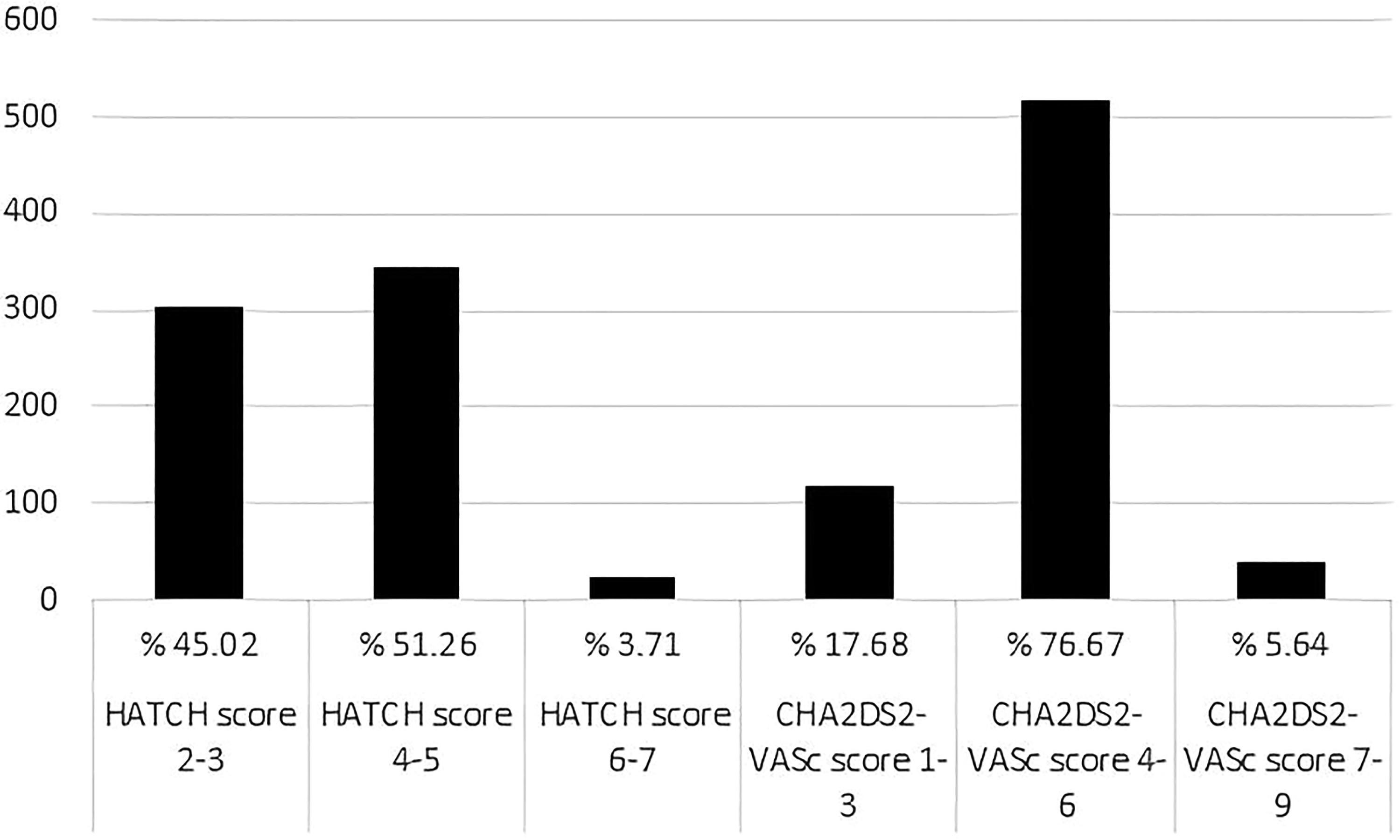
Distribution of scores in the general population.
Baseline Demographic Parameters of all Cohort.
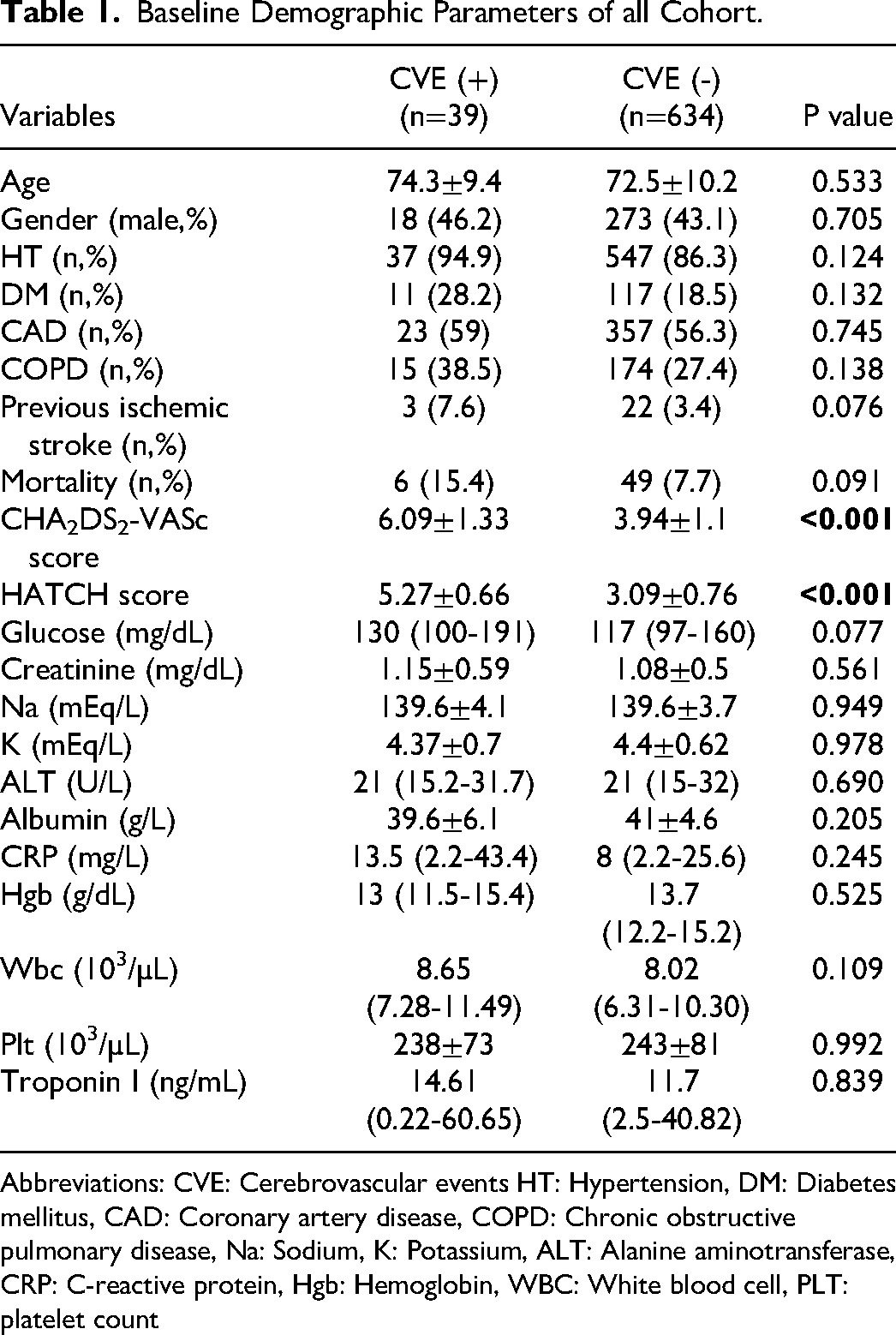
Abbreviations: CVE: Cerebrovascular events HT: Hypertension, DM: Diabetes mellitus, CAD: Coronary artery disease, COPD: Chronic obstructive pulmonary disease, Na: Sodium, K: Potassium, ALT: Alanine aminotransferase, CRP: C-reactive protein, Hgb: Hemoglobin, WBC: White blood cell, PLT: platelet count
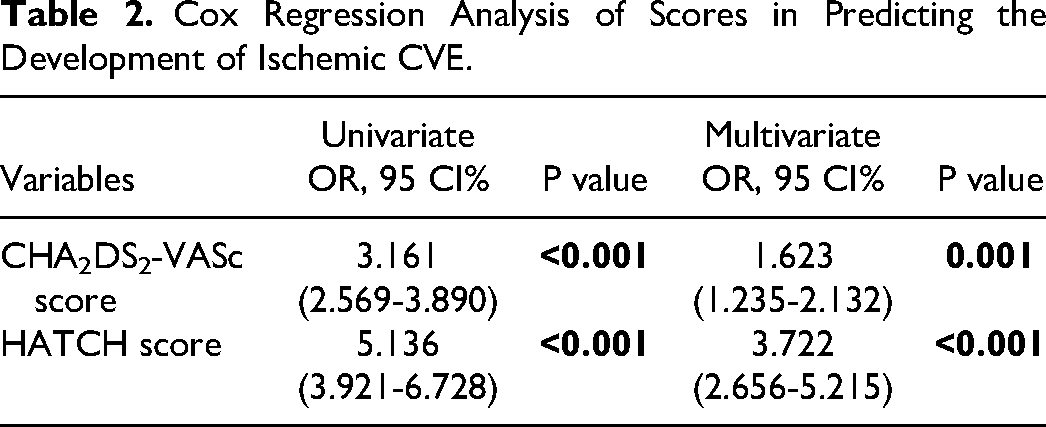
In the univariate and multivariate Cox regression analysis, we found that the CHA2DS2-VASc and HATCH scores were independent predictors of ischemic CVE (
Cox Regression Analysis of Scores in Predicting the Development of Ischemic CVE.
ROC analysis was used to evaluate the discrimination of ischemic CVE prediction ability of the CHA2DS2-VASc and the HATCH scores. The HATCH score showed the highest area under the curve (AUC) value to predict ischemic CVE. The ROC analysis, AUC for the CHA2DS2-VASc score was 0.884 (95% CI 0.828-0.940,
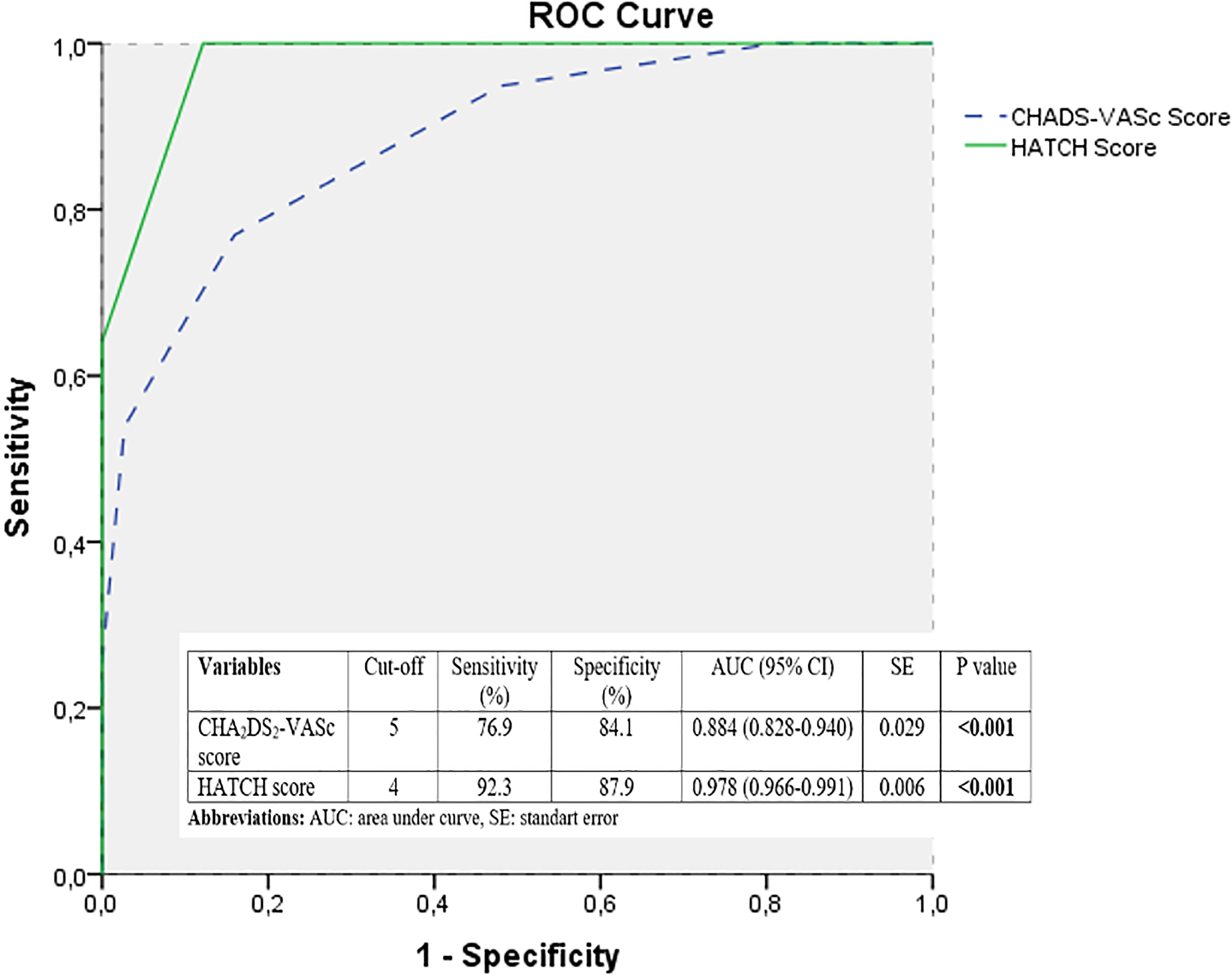
ROC curve analysis.
Discussion
Our study determined that the HATCH score could be a good predictor of the development of ischemic CVE in HF patients with AF. Although previous studies have emphasized the power of this score in detecting the development and recurrence of AF, our study pointed to its potential power in predicting the development of ischemic CVE.
Many scores have been used to predict the development of ischemic CVE in patients with AF. One of the most widely used is the CHA2DS2-VASc score. 8 The CHA2DS2-VASc score has been used for years to assess thromboembolic risk, including ischemic CVE, in patients with AF. 16 Some studies have even highlighted the power of the score in predicting mortality in cardiovascular diseases.17,18
The HATCH score was initially studied as a predictor of AF development. 19 In a later study, it was associated with an increased frequency of hospitalization and higher mortality in patients with acute HF. 20 The risk factors in both scores are similar. While DM was a risk factor in the CHA2DS2-VASc score, it was defined as a risk factor for COPD in the HATCH score. These two risk factors are the main features that distinguish the two scores from each other. At the same time, two points are given to HF in the HATCH score.
HF is a common cause of ischemic CVE. 21 The main mechanisms of HF causing ischemic CVE are AF and left ventricular thrombus due to hypokinesia in the left ventricular myocardium. 22 Chaotic atrial constrictions caused by AF likely trigger atrial thrombus. In addition, hypercoagulation, increased platelet aggregation, and decreased fibrinolysis caused by the renin-angiotensin-aldosterone system activated as a result of increased sympathetic activity may contribute to this situation. 23 When both AF and HF are present, the likelihood of an ischemic CVE occurring increases by about five times. 4 In our study, we had participants with both HF and AF. The fact that HF, a significant risk factor for ischemic CVE, received two points in the HATCH score may have caused this score to be a better predictor of ischemic CVE in our study.
In our study, DM and HT, both traditional stroke risk factors, did not demonstrate statistical significance. While some studies found that DM was a predictor of ischemic CVE in patients with AF,24,25 one study found that DM without any risk factors other than AF was not a predictor of ischemic CVE. 26 In addition, in a study involving a population of patients with atrial flutter, DM could not be identified as a predictor of ischemic CVE. 27 In terms of HT, it is a risk factor for ischemic CVE, according to most studies. However, some studies have found a significantly increased risk of ischemic CVE in patients with AF who are not under control or have blood pressure >160/90 mm Hg.24,28 In our study, HT and DM were not found to be predictive of ischemic CVE, which can be attributed to these circumstances. We could not obtain follow-up blood pressure measurement data of the patients.
COPD, which is a risk factor in the HATCH score, is a progressive disease and increases the risk of cardiac arrhythmia, especially AF. COPD patients with AF face higher complication rates. 29 Likewise, the presence of AF in COPD patients was found to be associated with more frequent hospitalizations. 11 COPD could be a significant contributor to the risk of all-cause death, stroke, extra-central nervous system embolism, and major bleeding in individuals with AF. 30 However, the evidence for an increased risk of ischemic CVE and systemic embolism in COPD patients with AF is unclear. It has been suggested that COPD can lead to platelet and cerebral artery dysfunction by raising the systemic inflammatory response via oxidative stress. In addition, the study suggested that smoking, which is a traditional risk factor for the development of COPD, increases the development of ischemic CVE because it increases the risk of cardiovascular disease. 31 A few studies have suggested that COPD may increase ischemic CVE in AF patients; however, other studies have not found an increased risk.32,33 In our study, COPD was not a predictor of ischemic CVE in patients with AF and HF.
Conclusion
Our study showed that the HATCH score can be an independent predictor of the development of ischemic CVE in HF patients with AF. This scoring system, which includes easy-to-use and easily accessible risk parameters, showed better sensitivity and specificity than the CHA2DS2-VASc score in HF patients with AF. For this reason, just as anticoagulant is started in HF patients with AF and a high CHA2DS2-VASc score, anticoagulant initiation may be considered in patients with a high HATCH score. However, randomized prospective studies are needed.
Limitations
Our study is retrospective-designed. The sample size of our study was relatively small. Since our study was single-centered, it may only partially reflect the general population. We think a prospective study of this subject in the larger AF population may yield more effective results.
Footnotes
Author Contribution
S. Aydin, E. Aksakal made substantial contributions to conception and design, acquisition of data, and analysis and interpretation of data. S. Aydin, E. Aksakal contributed to drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.