
Abstract
Background:
Risk stratification for stroke in patients with atrial fibrillation is a vital step in identifying whether antithrombotic therapy is indicated for stroke prevention in this common arrhythmia.
Purpose:
The aim of this study was to determine adherence to guideline-directed antithrombotic therapy based on Congestive Heart Failure (1 point), Hypertension (1 point), Age (≥75 years old is 2 points and 65-74 is 1 point), Diabetes (1 point), prior Stroke (2 points), Vascular Disease (1 point), and Sex Category (1 point if female; CHA2DS2–VASc) score in patients with atrial fibrillation (AF) on hospital discharge.
Methods:
A total of 293 patients discharged from this academic medical center with a history of atrial fibrillation from June 2014 to June 2016 were enrolled. Demographic data and indicators for antithrombotic therapy based on the CHA2DS2–VASc score were recorded, and factors that affected adherence to guideline-directed therapy, such as bleeding risk, falls, and alcohol abuse, were collected and analyzed.
Results:
At hospital discharge, 63% of patients with AF were on appropriate antithrombotic therapy, 50% with a CHA2DS2–VASc score ≥2. The odds ratio of appropriate therapy in patients with a CHA2DS2–VASc score ≥2 was 1.17 (95% confidence interval [CI]: 0.95-1.30; P = .18). When chart documentation for reasons to withhold anticoagulation was considered as appropriate therapy, 81% of patients with AF were discharged on appropriate antithrombotic therapy with an odds ratio of 1.57 (95% CI: 1.26 -1.96, P < .0001), with bleeding and falls risk as the most common reasons to withhold anticoagulation.
Conclusion:
Based on risk stratification of stroke through the CHA2DS2–VASc score, the majority of patients with AF were discharged from the hospital on appropriate antithrombotic therapy. Withholding anticoagulation due to falls risk should be reconsidered as a result of the known benefits of stroke prevention in atrial fibrillation.
Keywords
Atrial fibrillation (AF) is the most common cardiac arrhythmia impacting between 2.7 and 6.1 million Americans and leading to significant morbidity and mortality. 1 One of the most devastating complications of AF is thromboembolism. The risk of stroke associated with AF is 5 times higher than without AF and proportionally increases with age. 2,3 However, stroke is largely preventable as a result of the efficacy of oral anticoagulants (OACs) such as a vitamin K antagonist (VKA) or direct oral anticoagulants (DOACs). 3
Recognizing the risk of stroke is the first step to reducing stroke burden associated with AF. Risk stratification using the Congestive Heart Failure (1 point), Hypertension (1 point), Age (≥75 years old is 2 points and 65-74 is 1 point), Diabetes (1 point), prior Stroke (2 points), Vascular Disease (1 point), and Sex Category (1 point if female; CHA2DS2–VASc) score estimates a patient’s annual risk for stroke. The CHA2DS2–VASc score can be calculated using patient-specific information. This tool has been validated and incorporated into the American College of Cardiology (ACC)/American Heart Association (AHA) guidelines for the assessment of stroke risk in patients with AF. Based on the risk score, patients who would benefit from guideline-directed antithrombotic therapy can be identified. 4,5
Antithrombotic therapy for AF is underutilized. In a large quality improvement registry of outpatients with AF, Hsu et al found that <50% of patients who were determined to be the highest risk of stroke were prescribed an OAC. 6 Xian et al identified that 84% of patients admitted to the hospital with acute ischemic stroke, and a known history of AF did not receive therapeutic anticoagulation prior to hospital admission. However, evidence supports that with preceding antithrombotic therapy, such as antiplatelet therapy, a VKA, or a DOAC, patients have a lower odds of moderate or severe stroke when compared to patients on no antithrombotic therapy upon hospital admission. 7
The AHA Get With the Guidelines—AFIB performance improvement program assists hospital care teams in enhancing patient care and improving outcomes of patients with AF. This hospital-based performance initiative is designed to improve adherence to the AF guidelines. One of the program’s achievement measures is Food and Drug Administration (FDA)-approved anticoagulation prescribed prior to discharge according to CHA2DS2–VASc score risk stratification. 8
As an academic health center committed to providing quality health care, the importance of adherence to the guidelines in patients with AF is critical. Discharging patients with AF who meet criteria for antithrombotic therapy based on CHA2DS2–VASc score is an essential component in stroke prevention in the management of AF. 4 The purpose of this study was to determine adherence to guideline-directed antithrombotic therapy based on CHA2DS2–VASc score in patients with AF on hospital discharge.
Methods
Patient Population and Study Design
This was a retrospective, observational study in an academic medical center of patients admitted with a documented history of AF between June 2014 and June 2016. Any patient discharged from any inpatient unit with an International Classification of Disease-9 (ICD-9) Code of 427.31 (AF) was included if they were 18 years or older. Patients excluded were those with another indication for anticoagulation (eg, venous thromboembolism, mechanical heart valve) and those patients who were incarcerated, pregnant, or enrolled in an active research study mandating antithrombotic therapy.
Demographic data and indicators for antithrombotic therapy based on the CHA2DS2–VASc score were recorded at baseline, and factors that could affect adherence to guideline-directed therapy, such as bleeding risk, falls, and alcohol abuse, were collected through retrospective record review. A documented medical history of hypertension, diabetes mellitus, heart failure, stroke or transient ischemic attack (TIA), myocardial infarction (MI), chronic kidney disease, liver disease, vascular disease, and/or peripheral artery disease was collected. The occurrence of cardioversion and/or ablation during hospital admission was recorded, along with documentation of acute kidney injury. During hospital admission and at discharge, the receipt of antithrombotic therapy was collected including OAC (warfarin, apixaban, rivaroxaban, or dabigatran) and antiplatelet therapy (aspirin, clopidogrel, ticagrelor, or prasugrel). The combination of antiplatelet therapy and anticoagulant therapy was also documented. Food and Drug Administration-approved doses for antiplatelet and anticoagulant therapy were utilized, accounting for renal insufficiency. If antiplatelet or anticoagulant therapy was not prescribed, the electronic health record was reviewed, and a reason was recorded if present; if the reason recorded was related to the risk of anticoagulant use (ie, bleeding, falls), it was deemed appropriate in a separate analysis. Hospital readmission within 30 days was collected in addition to the reason for readmission, such as bleeding, arrhythmia, venous thromboembolism, and so on.
Study End Points and Statistical Analysis
The primary objective was to determine whether appropriate antithrombotic therapy based on CHAD2S2–VASc score was prescribed for patients with AF upon hospital discharge. Appropriate therapy was defined based on the AHA/ACC AF guidelines for risk-based antithrombotic therapy in the prevention of thromboembolism. Appropriate therapy for CHA2DS2–VASc score of 2 or greater was defined as oral anticoagulants; for CHA2DS2–VASc score of 1, no therapy or antiplatelet therapy or an OAC could have been considered and for CHA2DS2–VASc score of 0, therapy could be omitted; however, if the patient was cardioverted or ablated during hospitalization, oral anticoagulation was deemed appropriate. 5 Inappropriate therapy was defined as no anticoagulation therapy with a CHA2DS2–VASc score ≥2 or any anticoagulation therapy with a CHA2DS2–VASc score of 0. The secondary outcome was to review the incidence of 30-day hospital readmission.
Descriptive summaries are frequencies and percentages for categorical variables and medians, and minima and maxima for numeric variables. Groups were compared using the Pearson χ2 test (or Fisher exact test if some expected cell frequencies are small) for categorical data and using Wilcoxon rank sum tests for continuous data. The magnitude of the associations are described using odds ratio (OR) along with their 95% confidence interval (CI). The level of significance is 5%. All analyses were performed with SAS for Windows Version 9.4.
Results
A total of 293 patients were screened for study enrollment with 246 meeting inclusion criteria. The most common reasons for exclusion (43%) was another indication for anticoagulation, predominantly venous thromboembolism. Baseline characteristics are listed in Table 1. Patients were predominantly male (58.4%), with a median age of 67, and discharged from internal medicine services (52%). The majority of patients had a history of hypertension (89%), followed by diabetes (39.4%), and heart failure (39.4%). A CHA2DS2–VASc score of ≥2 was calculated for most patients who met inclusion criteria (91.1%), followed by a CHA2DS2–VASc score of 1 (6.5%), and a CHA2DS2–VASc score of 0 (2.4%). When considering baseline characteristics, there was no difference between appropriate and inappropriate therapy; however, discharge service had a trend toward significance (P = .06; Table 1).
Baseline Characteristics.

Abbreviation: TIA, transient ischemic attack.
a Between patients with previous stroke/TIA when compared to patient with no previous stroke/TIA.
Bold face means p-value < 0.05.
Choice of antithrombotic therapy is listed in Table 2. On hospital discharge, aspirin was the preferred antiplatelet agent (50%) for patients with CHA2DS2–VASc score of 0 (n = 6). For patients with CHA2DS2–VASc score of 1 (n = 16), 50% of patients were prescribed an OAC with or without ASA. Warfarin was the most commonly prescribed anticoagulant in 21% of patients with a CHA2DS2–VASc score ≥2 when utilized as monotherapy or in combination with an antiplatelet agent, followed by rivaroxaban (17%), apixaban (11%), and dabigatran (9%). Combination antiplatelet therapy with aspirin and clopidogrel was prescribed in 5% of patients with a CHA2DS2–VASc score ≥2.
Antithrombotic Therapy According to CHA2DS2–VASc Score.

Abbreviations: Apix, apixaban; ASA, aspirin; CHA2DS2–VASc, Congestive Heart Failure (1 point), Hypertension (1 point), Age (≥75 years old is 2 points and 65-74 is 1 point), Diabetes (1 point), prior Stroke (2 points), Vascular Disease (1 point), and Sex Category (1 point if female); Dab, dabigatran; P2Y12, clopidogrel, Riv, rivaroxaban, Warf, warfarin.
a Triple therapy (Warf+ASA+ P2Y12), n = 1.
b Triple therapy (Riv+ASA+P2Y12), n = 1.
The primary end point of appropriate antithrombotic therapy at hospital discharge occurred in 154 (63%) patients with AF (Table 3). However, 92 (37%) patients with AF were discharged on inappropriate antithrombotic therapy, and 78% of those patients had a CHA2DS2–VASc score between 2 and 5. The OR of appropriate therapy in patients with a CHA2DS2–VASc score ≥2 was 1.17 (CI: 0.95-1.30; P = .18).
Appropriate Antithrombotic Therapy Based on CHA2DS2–VASc Score.

Abbreviation: CHA2DS2–VASc, Congestive Heart Failure (1 point), Hypertension (1 point), Age (≥75 years old is 2 points and 65-74 is 1 point), Diabetes (1 point), prior Stroke (2 points), Vascular Disease (1 point), and Sex Category (1 point if female).
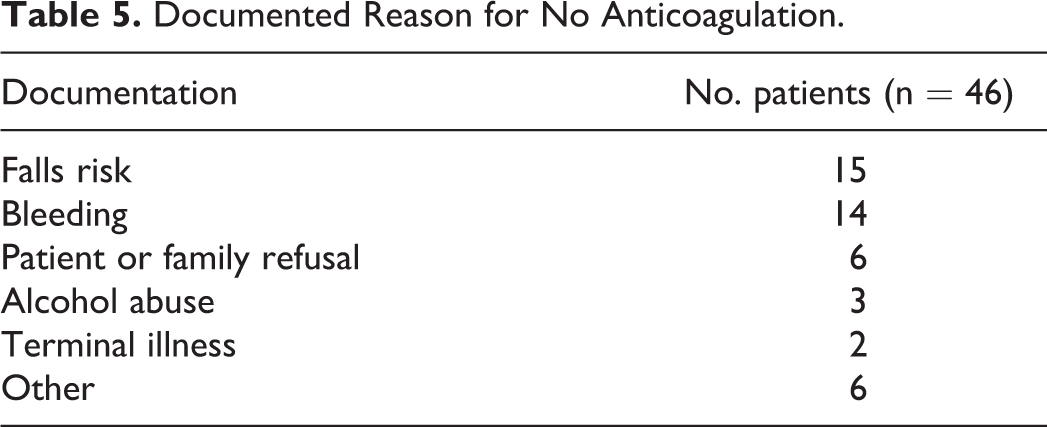
In a separate analysis, chart documentation of reasons to withhold anticoagulation at discharge was considered as appropriate therapy for an additional 46 patients with a CHA2DS2–VASc score ≥2 (Table 4). With consideration of chart documentation, appropriate antithrombotic therapy at hospital discharge occurred in 200 (81%) patients . The documented reasons to withhold anticoagulation at discharge included bleeding, falls risk, patient or family refusal, alcohol abuse, and terminal illness (Table 5). Sixty-three percent of patients did not receive anticoagulation because of bleeding and falls risk. The odds of appropriate therapy, when reasons to withhold anticoagulation were considered as appropriate therapy, in patients with CHA2DS2–VASc score ≥2 was 1.57 (CI: 1.26-1.96; P < .0001).
Appropriate Antithrombotic Therapy (documentation considered) Based on CHA2DS2–VASc Score.

Abbreviation: CHA2DS2–VASc, Congestive Heart Failure (1 point), Hypertension (1 point), Age (≥75 years old is 2 points and 65-74 is 1 point), Diabetes (1 point), prior Stroke (2 points), Vascular Disease (1 point), and Sex Category (1 point if female).
Documented Reason for No Anticoagulation.
The secondary end point assessed the rate of hospital readmission at 30 days, which was 15%. Reasons for readmission for all patients included arrhythmia (n = 5), bleeding (n = 5), and venous thromboembolism (n = 2), among others not associated with complications from anticoagulation therapy or atrial fibrillation (n = 24), such as infection, heart failure exacerbation, and acute kidney injury. Thirty-five (14%) patients with CHA2DS2–VASc score ≥2 were readmitted. At hospital discharge, 22 (61%) of those readmitted patients were discharged on appropriate anticoagulation based on CHA2DS2–VASc score. Only 1 readmitted patient with a CHA2DS2–VASc score of 5 had been discharged on an inappropriate dose of apixaban and was readmitted with altered mental status secondary to hyponatremia, unrelated to the anticoagulant.
In the current study, upon hospital discharge, patients who had a documented contraindication of bleeding to anticoagulation were elderly patients (ie, average age 69) and had an average Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History/Predisposition, Labile International Normalized Ratio (INR), Elderly, Drugs/Alcohol Concomitantly (HAS-BLED) score of 3.3, which validated the concern for a high risk of bleeding and withholding anticoagulation. 9 The average CHA2DS2–VASc score for these patients ranged from 2 to 8 (median, 4). When correlating CHA2DS2–VASc score and HAS-BLED score in terms of anticoagulation decision, those patients with higher CHA2DS2–VASc scores (4-8) were classified as a high bleeding risk per HAS-BLED score (≥3), and the majority were discharged on aspirin.
Of the 5 patients readmitted to the hospital with bleeding, the average age was 68 years with a CHA2DS2–VASc score between 2 and 6. Three of the 5 patients had a gastrointestinal bleed on readmission, 1 a hematoma, and 1 patient was bleeding from the arteriovenous fistula site. Two of the 5 patients were on warfarin with an INR of 1.0 and 4.1, respectively. The other 3 patients were only on aspirin upon readmission. During medication reconciliation, it was discovered that 1 of the 3 aspirin patients, as an outpatient, had been started on rivaroxaban and ibuprofen in addition to the aspirin which led to the admission for a gastrointestinal bleed.
Discussion
The underuse of oral anticoagulants in patients with AF has been highlighted in several studies. In a review of 54 studies of patients with AF treated with oral anticoagulants, over two-thirds of analyzed studies reported adherence to anticoagulation guidelines for patients with AF under 60%. This study’s adherence to anticoagulation was 63% when not accounting for documentation; however, it increased to 81% when accounting for documentation. Nine studies determined guideline-based treatment based on stroke risk scoring, the CHADS2 score, and treatment of high-risk patients with anticoagulants ranged from 39% to 92%. Of note, as CHADS2 scores increased, the use of oral anticoagulants rose. 10 In the current study, 58% of patients were discharged on anticoagulants and, overall, anticoagulant use increased as CHA2DS2–VASc scores increased.
Results from the Get with the Guidelines-Stroke (GWTG-Stroke) Program assessed the use of anticoagulation at hospital discharge in patients with AF admitted with stroke or TIA and over a 6-year period, an increase in prescribing in patients without contraindications to anticoagulation at hospital discharge was reported in over 90% of patients. Over one-third of patients had documented contraindications to anticoagulation at discharge which included bleeding (36.1%), falls risk (20.5%), and patient refusal (6.8%) most commonly reported. The GWTG-Stroke Program did not include DOACs, as at the time of publication, DOACs had not been incorporated into the AF guidelines. During the study period, documentation of the specific contraindications to anticoagulation improved, and one observation of patients with diabetes and advanced age in the setting of stroke was that anticoagulation was less frequently prescribed. 11 This observation was not uncovered in the current study. However, the current study not only assessed prescribing practices but also the appropriateness of the agent(s), including antiplatelet(s), VKA, and/or DOAC, prescribed based on the CHA2DS2–VASc score. When contraindications to withhold anticoagulation were included as appropriate therapy for patients with CHA2DS2–VASc score ≥2, statistical significance resulted. Documented contraindications leading to withhold anticoagulation were present in about 20% of patients; one-third (33%) of those patients had the documented contraindication of falls risk closely followed by bleeding (30%). The average CHA2DS2–VASc score of patients with contraindications due to falls risk and bleeding was 4.5 and 4.6, respectively, whereas, for the other documented contraindications to anticoagulation, the average CHA2DS2–VASc score was 3.7.
Withholding anticoagulation for a high risk of falling is controversial. Although it is reported that 30% to 40% of adults aged 65 and older will have at least 1 fall in the preceding year, this rate exceeds 50% in nursing home residents. 12 Man-Son-Hing et al utilized a Markov decision analysis to determine antithrombotic drug efficacy in patients with AF aged 65 and older and discovered an individual would have to fall 295 times in 1 year for the risk of major bleeding from the fall to outweigh the benefits of warfarin in stroke reduction. 13 A large, matched cohort study by Kooistra et al determined the risk of bleeding in patients treated with a VKA was not significantly increased in patients aged 90 or older when compared to those aged 70 to 79 (hazard ratio [HR]: 1.26; CI: 1.05-1.5) and was comparable to that of patients aged 80 to 89 (HR: 1.07; CI: 0.89-1.27). However, the risk of developing thrombosis was higher for patients aged 90 or older (HR: 2.14; CI: 1.22-3.75) and patients aged 80 to 89 (HR: 1.75; CI: 1.002-3.05) over patients in their 70s. 14 In the current study, the average age of patients with a documented fall risk was 79 years, and 80% were discharged home on antiplatelet therapy alone with an average CHA2DS2–VASc score of 4.5. Although the risk of falls is an important assessment in anticoagulation management, literature supports that the benefits of anticoagulation in stroke prevention in AF outweigh the risk of bleeding, particularly with close monitoring in the elderly population, and falls alone should not be justification to withhold anticoagulation. 12,15 In the current study, this would have allowed 15 patients with AF with a 4.5% risk of stroke based on their average CHA2DS2–VASc score to be prescribed guideline-directed anticoagulant therapy for AF at hospital discharge.
Concerns about bleeding have also led to the underutilization of anticoagulants in AF, particularly in the elderly patients, as the prevalence of AF and stroke increase with age. 5 It is well documented that the risk of bleeding in patients taking a VKA increases with age. 16 –18 In a retrospective, propensity-matched study of DOACs by Abraham et al, gastrointestinal bleeding events increased in patients with AF aged 75 years or older with a mean CHA2DS2–VASc score between 3.2 and 4. Apixaban had a lower risk of gastrointestinal bleeding in the very elderly patients when compared to dabigatran or rivaroxaban. 19 Noseworthy et al had similar findings in a propensity-matched cohort study, where apixaban had a lower risk of major bleeding and trended toward a lower risk of intracranial bleeding. 20
The concern of bleeding is enhanced when patients with AF are on combination therapy with an anticoagulant and antiplatelet(s) in AF. Combination therapy is considered reasonable if clopidogrel is prescribed with oral anticoagulants, but without aspirin, after coronary revascularization in patients with CHA2DS2–VASc score ≥2. 5 In patients with AF having stable coronary artery disease, the Danish cohort study reported that the risk of MI and/or coronary death or thromboembolism was no different when a VKA alone was compared to a VKA with aspirin or clopidogrel; however, the risk of bleeding was greater with the addition of either antiplatelet agent. 21 Twenty-two patients with a CHA2DS2–VASc score ≥2 were discharged on warfarin in combination with aspirin or clopidogrel in the current study, and 91% of those patients were discharged on appropriate therapy. Of the 22 patients, 19 had an appropriate indication for antiplatelet therapy, which included primary prevention of coronary artery disease with diabetes (n = 14), followed by peripheral artery disease (n = 3), and a documented MI (n = 2). The majority (69%) of patients in the WOEST trial received anticoagulation for AF. All patients undergoing percutaneous intervention (PCI) received either dual therapy with warfarin and clopidogrel or triple therapy with warfarin, clopidogrel, and aspirin. Dual therapy was associated with a lower rate of bleeding events compared to triple therapy (P < .0001), and there was no difference in the rate of thrombotic and thromboembolic events. 22 Three patients in the current study were discharged on warfarin and clopidogrel; none of the patients had a history of PCI or had a PCI during hospital admission. Unlike the WOEST trial, the PIONEER AF-PCI study incorporated a DOAC and included patients with AF undergoing a PCI with stent placement. Rivaroxaban 15 mg daily in combination with clopidogrel was associated with a lower rate of clinically significant bleeding when compared to warfarin plus dual antiplatelet therapy for 1, 6, or 12 months. 23 The combination of rivaroxaban and aspirin or clopidogrel was prescribed to 4 patients with AF at hospital discharge in the current study; 2 of the 4 patients had a MI and PCI during hospital admission. Similar to the PIONEER AF-PCI study, the RE-DUAL PCI study included patients on a DOAC, dabigatran, who had AF and were undergoing PCI with stent placement. For bleeding and ischemic outcomes, this study found dabigatran 110 mg or 150 mg twice daily in addition to clopidogrel to be noninferior to triple therapy with warfarin, aspirin, and either clopidogrel or ticagrelor. 24 There was 1 patient in the current study on dabigatran with clopidogrel, and it was considered appropriate therapy in the setting of a MI and PCI. Although the PIONEER AF-PCI and RE-DUAL PCI studies only included patients with AF, both were published after the study period of patients who met inclusion criteria for the current study. Therefore, antiplatelet and anticoagulant decisions for these patients were not made based on the results from either of these 2 trials. However, the WOEST trial was published before the study period and could have impacted antithrombotic therapy decisions for patients discharged with AF.
This study is not without limitations. The retrospective nature of this study relied on chart documentation within the electronic health record. Diagnosis of AF was based on ICD coding and confirmed upon further chart review of documentation during the admission. Additionally, the patient population was predominantly medical inpatients, and the cardiology service is a medically focused service providing comprehensive cardiovascular care. When considering the prevalence of postoperative AF and the few surgical patients included, the majority of surgical patients were taking an anticoagulant prior to admission; therefore, the incidence of postoperative AF would have been low.
Conclusion
Our study aligns with the literature documenting adherence to anticoagulation guidelines for AF. However, a further step assessed was CHA2DS2–VASc score (vs CHADS2 score) and the antithrombotic agent(s) prescribed at hospital discharge, which included DOACs, based on the patients’ CHA2DS2–VASc score. As this study was able to determine and highlight the appropriateness of the agent(s) prescribed, patients were able to receive the highest benefit of therapy for preventable thromboembolic complications of AF, while circumventing unwanted adverse events.
Our study results showed that, although the majority of patients with AF were discharged from the hospital on anticoagulation, there is room for improvement in adherence and a renewed commitment to the Get With the Guidelines approach. When documentation was considered, there was a significant difference in those patients who left the hospital on appropriate therapy. Reassessing the appropriateness of documented reasons not to anticoagulate patients when an anticoagulant is indicated needs to be revisited, particularly when the reason is falls risk, knowing patients experience more benefit than risk especially in advanced age. Because stroke is the most feared and devastating complication of AF, antithrombotic therapy has an important role in thromboembolic risk reduction when appropriately prescribed in patients with AF.
Footnotes
Authors’ Note
L. Dupree contributed to conception and design; contributed to interpretation; drafted the manuscript; crtically revised the manuscript; gave final approval. C. Smotherman contributed to analysis and interpretation; crtically revised the manuscript; gave final approval. Both the authors agree to be accountable for all aspectsof work ensuring itergriy and accurarcy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.