
Abstract
In-stent restenosis (ISR) is a limitation of percutaneous coronary intervention and has been linked to specific clinical and angiographic variables. The aim of the present study was to investigate the predictive value of preprocedural CHA2DS2-VASc score on ISR in patients undergoing revascularization with bare-metal stent (BMS) implantation for stable coronary artery disease or acute coronary syndrome. In the years 2012 to 2014, a total of 358 consecutive patients (mean age: 62.36 ± 11.28 years and 62.2% men) who had undergone successful BMS implantation were included in the study. All patients underwent stent implantation at admission to our center and had another coronary angiography performed due to recurrence of the symptoms consistent with myocardial ischemia and/or a stress test indicating ischemia. The patients were divided into 2 groups—ISR (n = 166) and non-ISR (n = 192). Angiographic ISR was defined as narrowing ≥50% in the stented coronary artery segment at follow-up angiography. The mean CHA2DS2-VASc score was 3.42 ± 1.35 (range 1-7). The CHA2DS2-VASc scores and high-sensitivity C-reactive protein (hs-CRP) levels were higher in the ISR group compared to the non-ISR group. At multivariable analysis, CHA2DS2-VASc score (odds ratio [OR]: 2.004, 95% confidence interval: 1.361-2.949, P < .001), total stent length (OR: 1.093, P = .001), stent diameter (OR: 0.129, P < .001), and hs-CRP (OR: 1.224, P < .001) emerged as independent risk factors for ISR. In conclusion, preprocedural CHA2DS2-VASc is an easily calculated score that provides an additional level of risk stratification beyond that provided by conventional risk factors. Thus, this score can be used as a simple and effective tool to predict ISR in patients undergoing BMS implantation.
Introduction
In spite of new medications and development of revascularization techniques, in-stent restenosis (ISR) after successful percutaneous coronary intervention (PCI) remains one of the most challenging problems in interventional cardiology and limits the efficacy of the procedure. 1 Bare-metal ISR is not a benign entity and has been associated with both poor survival and acute coronary syndromes (ACSs). 2 –4 The development of ISR has been linked to several specific clinical, laboratory, and angiographic variables. The CHA2DS2-VASc score (congestive heart failure [CHF]; hypertension; age ≥75 years [doubled]; type 2 diabetes; previous stroke or transient ischemic attack [doubled]; vascular disease; age 65-74 years; and sex [female] category) has been initially recommended for the assessment of thromboembolic risk in patients with atrial fibrillation (AF). 5 At the same time, it has recently been used to predict not only thromboembolic risk in AF but also adverse events in various cardiovascular diseases, irrespective of the presence or absence of AF. In recent years, several studies have demonstrated an association of the CHA2DS2-VASc score with cardiovascular prognosis and adverse outcomes in different patient populations, including heart failure, stable coronary artery disease (CAD), and ACS beyond the original AF field. 6 –12 The predictive value of CHA2DS2-VASc score on ISR still remains unclear, although all of the components of the CHA2DS2-VASc score are important risk factors for ISR. For this reason, the present study was designed to evaluate the predictive value of the preprocedural CHA2DS2-VASc score on the development of ISR in patients who undergoing revascularization with bare-metal stent (BMS) by reason of the both stable CAD and ACS.
Methods
Patients and Definitions
From December 2012 to April 2014, a total of 406 consecutive patients who underwent coronary angiography (CA) for the evaluation of CAD with the diagnosis of both stable angina pectoris and ACSs (including patients with unstable angina, non-ST-segment elevation and ST-segment elevation myocardial infarction) and subsequently underwent BMS implantation at our hospital, then accepted CA follow-up for ISR examination, were retrospectively recruited in this study. Indications for follow-up CA were either of the following: complaints consistent with myocardial ischemia and/or a stress test indicating myocardial ischemia. Inclusion criteria were broad to reflect routine clinical practice. Exclusion criteria were few and included patients with severe renal disease, acute/chronic inflammatory/infectious disease, and coronary artery bypass graft disease. After excluding 48 patients, remaining 358 patients’ information were eventually analyzed in detail to gather data on medical history, including information about traditional cardiovascular risk factors (gender, age, smoking status, hypercholesterolemia, hypertension, prior stroke, and diabetes mellitus), current medications, and laboratory data. The preprocedural CHA2DS2-VASc scores were calculated for each patient according to their echocardiographic and demographic characteristics. Based on this score, patients were given 1 point for CHF, hypertension, aged 65 to 74 years, diabetes mellitus, vascular disease, and female gender and 2 points for age ≥75 years and previous stroke or transient ischemic attack. 5 All patients had at least a score of 1 since all of them underwent PCI, and thus they had vascular atherosclerosis. As part of our preprocedural protocol, complete blood count and biochemical parameters had already been available before BMS implantation for all patients. The study protocol was approved by local ethic committee of our hospital. All patients provided written informed consent for participation in the study.
Congestive heart failure was defined as a low ejection fraction (left ventricular ejection fraction [LVEF] <40%) and clinical signs or chest X-ray findings of congestion. Hypertension was defined as a systolic pressure value of >140 mm Hg and/or a diastolic pressure value of >90 in at least 2 separate measurements or being on an antihypertensive therapy. Diabetes mellitus was defined as a previous diagnosis if a patient followed a diet or used antidiabetic medication or had a fasting venous blood glucose level of 126 mg/dL in 2 separate measurements in previously untreated patients. Hypercholesterolemia was based on the presence of a total cholesterol level of ≥200 mg/dL in the fasting state. The estimated glomerular filtration rate (eGFR) was calculated by the modification of diet in renal disease formula, 13 and severe renal disease was defined as an eGFR <30 mL/min/1.73 m2, either with or without preexisting dialysis. Echocardiography was performed blindly by an experienced echocardiographer using the standard techniques. Left ventricular ejection fraction was calculated using Simpson method.
Coronary Angiography
Coronary interventions were performed by using 6F or 7F guiding catheters and recorded in digital storage for further analysis. All of the patients received chewable aspirin (300 mg) and oral clopidogrel (600 mg loading dose) before or immediately after CA. Procedural anticoagulation was achieved with unfractionated heparin at a dose of 5.000 IU or 70 to 100 IU/kg of body weight; the use of glycoprotein IIb/IIIa inhibitors and predilatation or postdilatation after BMS implantation of the lesion was left to the operator’s discretion. After the procedure, clopidogrel (75 mg/d) was prescribed for at least 1 month, but preferably up to 1 year (especially in patients with ACS), and aspirin (100 mg/d) was continued indefinitely. All patients were encouraged to take guideline-recommended medications including statins, angiotensin–aldosterone system inhibitors, and β-blockers unless contraindicated. Follow-up CA (Siemens Axiom Artis Zee 2011, Germany) was performed with standard techniques via the femoral or radial approach due to clinical indications. Angiographic analyses were performed by 2 experienced interventional cardiologists who were blinded to patient data. In the event of disagreement, the assessment was then carried out by a third interventional cardiologist, and the final analysis was then considered. Intraobserver variability was 96% and 97.5%, and interobserver variability was 95% and 96%. Angiographic ISR was defined as ≥50% luminal diameter narrowing of the stented or peri-stent segment (defined as a length of 5 mm proximal and distal to the stent edge) at follow-up CA, whereas non-ISR was defined as <50% or no stenosis. 14
Statistical Analysis
Continuous variables were presented as mean (standard deviation) if normally distributed or median (interquartile range) if nonnormally distributed. Categorical variables were expressed as numbers and percentages. Continuous variables with normal distribution were compared using unpaired Student t test and with nonnormal distribution were compared using Mann-Whitney U test or Wilcoxon signed rank test. Categorical variables were compared using χ2 test or Fisher exact test if necessary. Receiver operating characteristic (ROC) curve analyses were constructed to determine the predictive value of CHA2DS2-VASc score on ISR. To prepare for potential confounding, it was considered the following clinical and laboratory factors, which are not included in the elements of the CHA2DS2-VASc score and are generally known or suspected to be associated with the risk of ISR: total stent length per lesion, average stent diameter, fasting glucose, current smokers, CHA2DS2-VASc score, hemoglobin, triglyceride, high-sensitivity C-reactive protein (hs-CRP), eGFR, red cell distribution width (RDW), and neutrophil/lymphocyte ratio. All these possible variables were assessed using univariable and multivariable logistic regression analysis. A P value <.05 was considered statistically significant. All statistical analyses were performed using SPSS (version 18.0 for Windows, SPSS, Inc, Chicago, Illinois).
Results
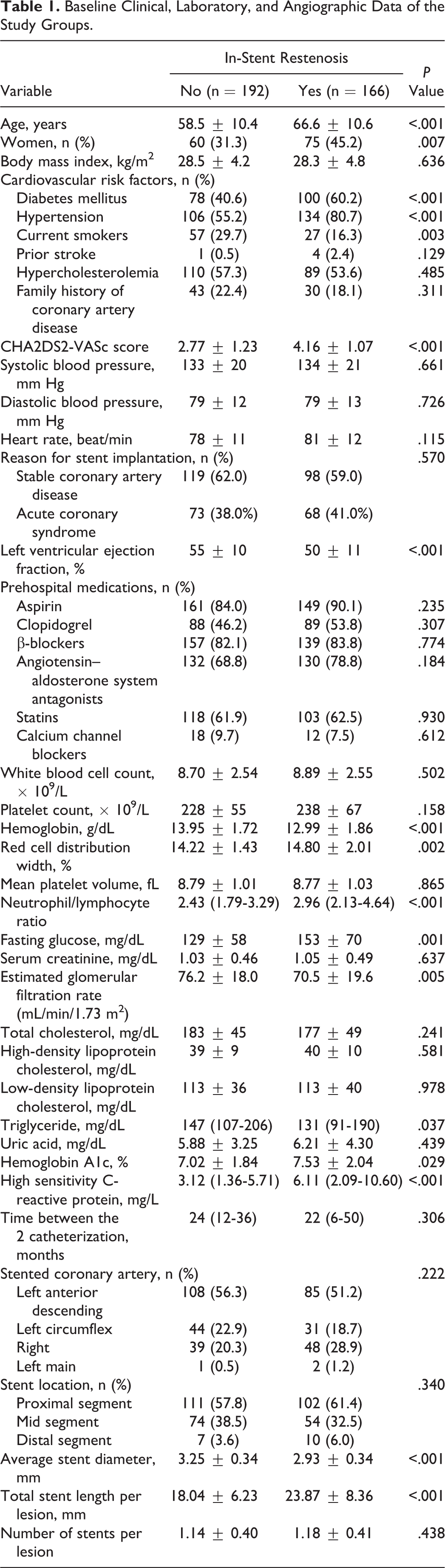
The 358 patients had a mean age of 62.36 ± 11.28 years and included 37.7% women. The mean CHA2DS2-VASc score was 3.41 ± 1.35 years (range 1-7). As indicated in Table 1, many of the components constituting CHA2DS2-VASc score, such as age, prevalence of hypertension, diabetes mellitus, and female gender were observed to be higher, but LVEF and frequency of current smokers were lower in the ISR group, as expected. The median time to assessment of restenosis was 24.0 months (range 6-60) following the stent implantation. In terms of the time between the 2 catheterization, there was no significant difference between non-ISR group and ISR group (24 [12-36] months vs 22 [6-50] months, respectively, P = .306). Total stent length per lesion was significantly higher, and average stent diameter was significantly lower in patients with ISR compared to those with non-ISR. There was no statistical difference with regard to prehospital medications between the groups. The basic biochemical and hematologic parameters are also listed in Table 1. The ISR group had lower levels of hemoglobin, eGFR, triglyceride, and higher levels of fasting glucose, RDW, neutrophil/lymphocyte ratio, hs-CRP, and hemoglobin A1c than the non-ISR group. As shown in Figure 1, the percentages of ISR were gradually increased as the CHA2DS2-VASc score increased. In the ROC curve analysis, the number of CHA2DS2-VASc score (Figure 2A) and the presence of CHA2DS2-VASc score ≥4 (Figure 2B) were identified as effective predictive cutoff points for ISR (area under the curve [AUC] = 0.784, 95% confidence interval [CI]: 0.737-0.830, P < .001 and AUC = 0.714, 95% CI: 0.660-0.768, P < .001, respectively), with a sensitivity of 74.1% and a specificity of 68.7%, for both of them.
Baseline Clinical, Laboratory, and Angiographic Data of the Study Groups.
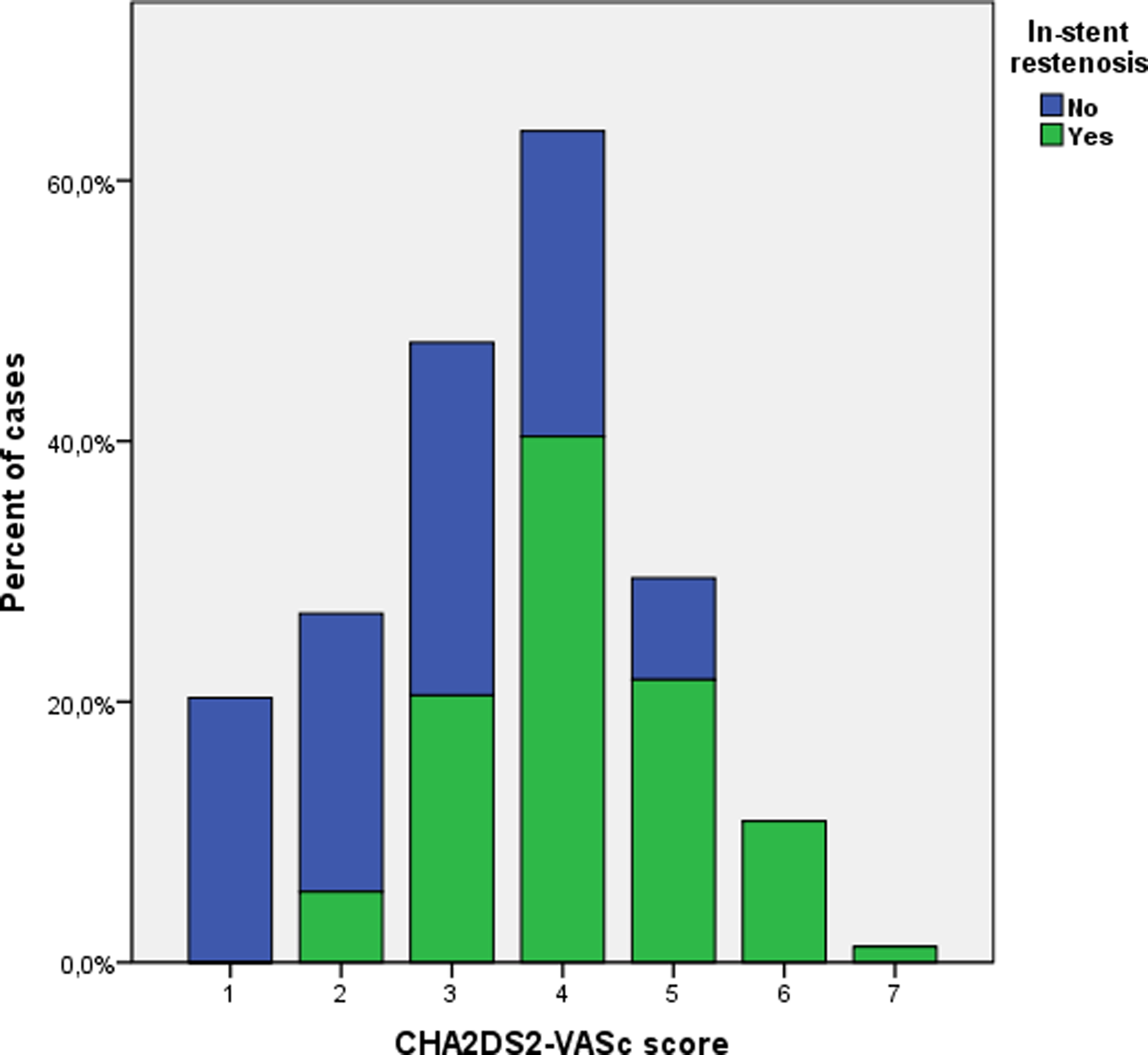
Comparison of in-stent restenosis percentages according to the CHA2DS2-VASc scores.
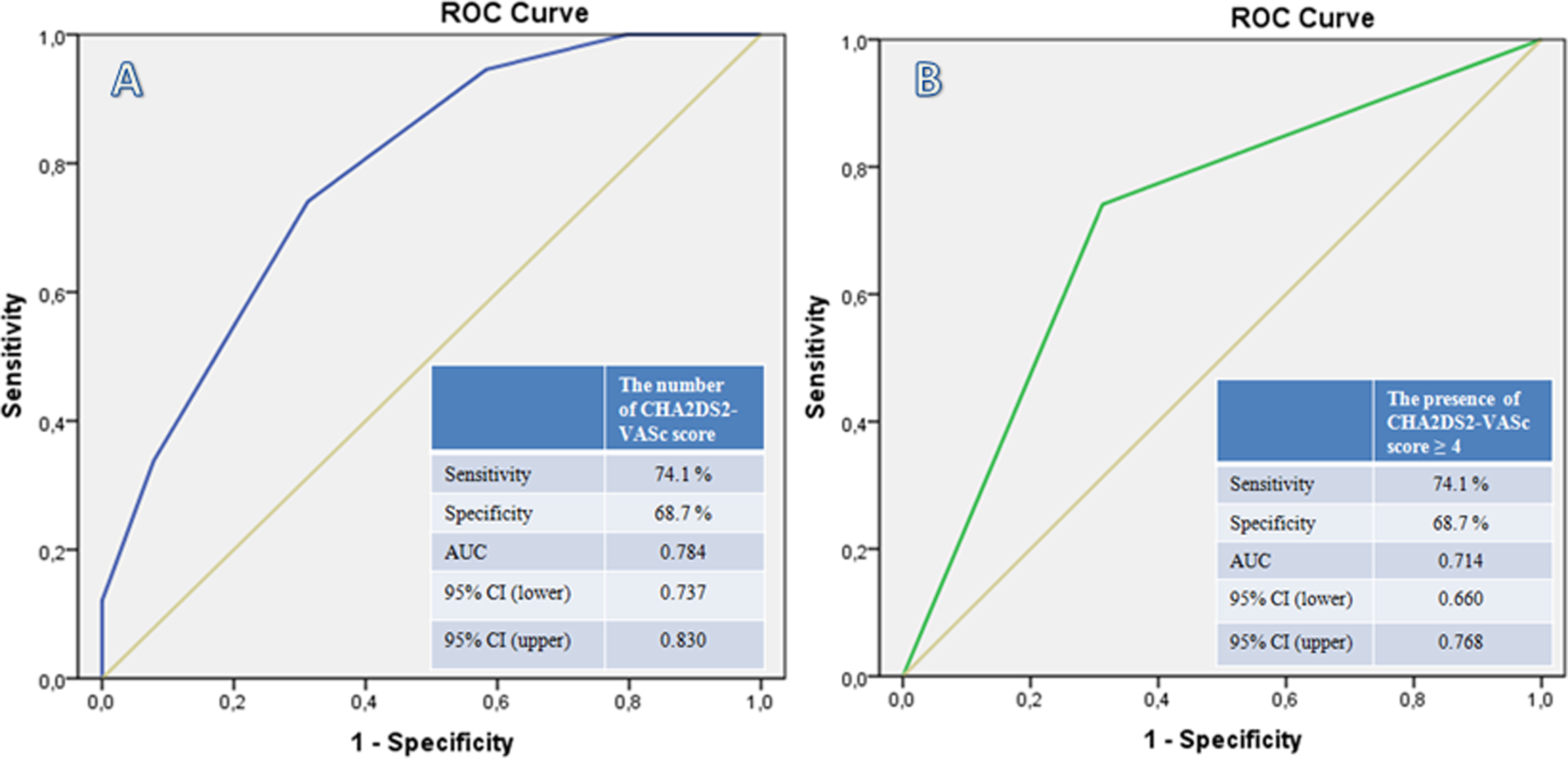
The ROC curve analyses for the number of CHA2DS2-VASc score (A) and the presence of CHA2DS2-VASc score ≥4 (B) for predicting in-stent restenosis. AUC indicates area under the curve; CI, confidence interval; ROC, receiver operating characteristic.
In the multivariable logistic regression analysis to determine the predictors of ISR, total stent length per lesion (odds ratio [OR]: 1.093, 95% CI: 1.039-1.151, P = .001), average stent diameter (OR: 0.129, 95% CI: 0.045-3.67, P < .001), CHA2DS2-VASc score (OR: 2.004, 95% CI: 1.361-2.949, P < .001), and hs-CRP (OR: 1.224, 95% CI: 1.107-1.354, P < .001) were independent risk factors for ISR in patients who underwent BMS implantation (Table 2).
Univariate and Multivariate Predictors of In-Stent Restenosis in Patients Undergoing Revascularization With Bare-Metal Stents.
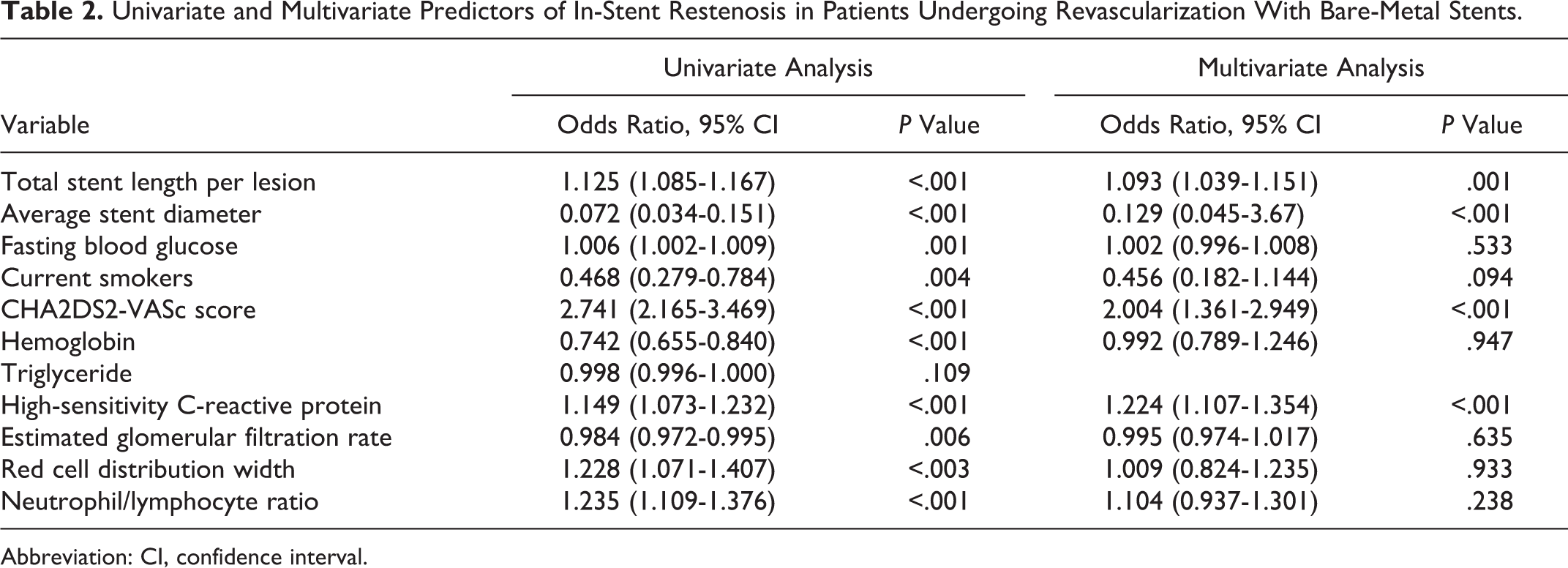
Abbreviation: CI, confidence interval.
Discussion
The main finding of this study is that the CHA2DS2-VASc score is independently and positively associated with an increased risk of ISR in patients undergoing revascularization with BMS in the settings of stable CAD and ACS. The optimal cutoff value of CHA2DS2-VASc score in the prediction ISR is ≥4, with a good sensitivity and specificity. In contrast to other available ISR risk stratification tools, the CHA2DS2-VASc score is a reliable and easily calculated scoring tool and therefore may be applied in daily practice to predict bare-metal ISR.
Coronary stenting is the most common approach of PCI. However, ISR remains an unresolved issue and it limits the efficacy of the procedure. 1 In spite of major improvements in stents material, interventional techniques, and drug therapies, the incidence of ISR still ranged from 20.0% to 50.3% depending on clinical and procedural factors, and the stent type implanted. 15 It was shown that ISR with BMS is significantly associated with long-term adverse clinical outcomes. 2 –4 Therefore, ISR is considered the Achilles heel of interventional cardiology. The development of ISR following BMS implantation has been linked to several clinical, lesion, and procedural factors and, most importantly, patient-related factors. These include demographic factors such as age, diabetes, hypertension, CHF, renal failure, female gender, and angiographic factors, such as vessel reference diameter and stent length. 16 –22 The CHA2DS2-VASc score combines the predictive risk of many of these factors instead of a single risk factor. Indeed, the CHA2DS2-VASc score was initially suggested as a risk assessment tool for thromboembolic events in patients with AF. 5 However, it has recently been used to predict prognosis and adverse clinical events in numerous cardiovascular diseases, including heart failure, stable CAD, and ACS, irrespective of the presence or absence of AF. 6 –11 Recently, in a study by Ünal et al, 12 a CHA2DS2-VASc score of >2 has been found to be an independent predictor for incidence of stent thrombosis. More recently, we have shown that CHA2DS2-VASc score independently predicts contrast-induced nephropathy in patients with ACS treated by PCI. 23 As mentioned above, although the CHA2DS2-VASc score includes potential risk factors for ISR, whether CHA2DS2-VASc score may predict the development of ISR has not been investigated yet. Therefore, the present study, to the best of our knowledge, was the first analysis aimed at finding out the relationship between CHA2DS2-VASc score and ISR using conventional CA. In the light of this study, it can be said that preprocedural CHA2DS2-VASc score independently predicts bare-metal ISR in patients with both stable CAD and ACS.
Kastrati et al reported the predictive role of diabetes mellitus and hypertension in ISR after BMS placement confirms previous data after various PCIs. 15 Through different mechanisms, both diabetes mellitus and arterial hypertension are associated with endothelial dysfunction and overexpression of several growth factors that promote muscle cell proliferation, 24 –26 the principal mechanism of lumen renarrowing after BMS implantation. 27 Inflammation also plays a pivotal role in the development of ISR by acting on the neointimal tissue at the sites of coronary stenting. 28 In a meta-analysis, it was shown that preprocedural CRP, widely accepted an inflammatory marker, levels were significantly associated with ISR after BMS implantation. 29 We previously demonstrated that increased RDW, another inflammatory marker, is associated with BMS restenosis in patients with stable CAD. 30 Similarly, Zhao et al 31 found the association of RDW with ISR in patients with unstable CAD. In accordance with the previous studies, in the present study, it was also shown that hs-CRP was independently associated with the development of bare-metal ISR. Expression of various factors associated with inflammatory cell infiltrates may affect the development of neointimal proliferation, which is main mechanism for the development of ISR. So, elevated hs-CRP levels may reflect the pathological process of ISR via different inflammation pathways.
Taken together, this study suggests that the CHA2DS2-VASc is a simple and comprehensive risk assessment score that provides an additional level of risk stratification beyond that provided by conventional risk scores in predicting ISR in patients undergoing revascularization with BMS. Because high CHA2DS2-VASc scores are associated with a higher risk of bare-metal ISR, patients with high CHA2DS2-VASc score undergoing stent implantations should be considered for drug-eluting stents and other measures to reduce ISR.
There were some limitations to this study. First, enrollment was a single-center, retrospective observational design. Second, the definition of ISR was based on visual assessment. Although this visual assessment of ISR is easily to be incorporated into the routine clinical practice, the degree of in-stent renarrowing may be more accurately assessed by intravascular ultrasound or optical computed tomography. Finally, the angiographic follow-up was not available for all included patients. Notwithstanding these limitations, this is reportedly the first study focusing on the CHA2DS2-VASc score with regard to its predictive value in ISR after BMS implantation.
In conclusion, the CHA2DS2-VASc score is an independent risk factor for ISR in patients who underwent BMS for both stable CAD and ACS. This score provides an additional level of risk stratification beyond that provided by conventional risk factors.
Footnotes
Authors’ Note
All authors have substantial contributions to conception and design, or acquisition of data, and analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.