
Abstract
Pulmonary embolism (PE) is an important cause of sudden death and is difficult to diagnose. Therefore unnecessary radiological investigations are often resorted to. Although some inflammatory parameters in the hemogram have been found to play a role in the diagnosis of PE, many parameters have not been adequately investigated. We aimed to evaluate potential inflammatory parameters in hemogram in the diagnosis of PE and to determine the parameters with the highest diagnostic value. This single-center, retrospective study was performed by evaluating 114 cases with suspected PE admitted to the emergency department between January 2017 and June 2022. Among 114 cases, 62 cases with a definitive diagnosis of PE by pulmonary computed tomography angiography served as the PE group and 52 cases without PE served as the control group. Admission hemogram parameters of both groups were recorded. Potential chronic diseases and acute conditions affecting hemogram were excluded from the study
Introduction
Pulmonary embolism (PE) most commonly develops when a thrombus ruptures from a lower extremity vein and occludes branches of the pulmonary artery. The annual incidence is 6 to 120 per 10 000 people. It has been determined to cause 60 000 to 100 000 deaths per year in the United States. 1 Due to its nonspecific clinical presentation PE is difficult to diagnose. One of the main challenges in daily clinical practice is actually to determine when PE should be suspected. Because of these difficulties unnecessary thorax computed tomography (thorax CT) has increased in recent years. 2 However, these examinations are relatively costly, less feasible, and have limited use in primary care hospitals. 3 D-dimer, one of the laboratory parameters is commonly requested in the diagnostic phase but its poor specificity has limited its diagnostic efficiency. Therefore hemogram parameters have been investigated in the diagnosis of PE recently because they are cheap and easily accessible. Potential inflammatory biomarkers in the hemogram can guide as useful markers both for explaining the pathogenesis of thrombosis and for diagnosis in PE.4–6
In one study, it was found that mean platelet volume (MPV) and platelet distribution width (PDW) levels were significantly higher in patients with PE and the use of MPV together with D-dimer helped to diagnose PE. 7 In another study, neutrophil/lymphocyte ratio (NLR) and platelet/lymphocyte ratio (PLR) showed significant efficacy in the diagnosis of high-risk PE. 8
If hemogram parameters with high specificity can be determined, diagnostic difficulty will decrease and high probability cases can be identified. For this purpose in our study, we aimed to evaluate potential inflammatory parameters in hemogram (such as neutrophil, monocyte, lymphocyte, platelet indices, NLR, PLR, and immature granulocyte) in the diagnosis of PE and to determine the parameters with the highest diagnostic differentiation.
Material and Methods
Patient Population and Study Design
This single-center, retrospective study was performed by evaluating the cases who presented to the emergency department of Medipol University Hospital between January 2017 and June 2022 and suspected PE. The study was approved by the ethics committee of Medipol University (E-10840098-772.02-3115). Among 114 cases with suspected PE, 62 cases with PE served as PE group and 52 cases without PE served as control group. Demographic data of the cases, admission hemogram parameters, and CT pulmonary angiography (CTPA) reports were recorded.
Inclusion and Exclusion Criteria
Cases who were over 18 years of age had complete file and laboratory records and underwent CTPA scan with suspicion of PE at emergency department presentation were included in the study.
Exclusion criteria were being under 18 years of age, missing data (incomplete file, laboratory, or imaging records), acute or chronic renal failure, bone fractures, hematologic disease, rheumatic disease, significant active cardiac disease such as arrhythmia and valvular heart disease, infection, and drug use affecting hemogram parameters.
Computed Tomography Pulmonary Angiography
PE was confirmed by CTPA according to European Society of Cardiology guidelines. 9 After the reports were provided by the radiologist, they were checked and confirmed by 2 pulmonologists.
Complete Blood Count and Inflammatory Marker Evaluation
Hemogram data of the cases were obtained at the emergency service application. Hemogram parameters were analyzed by Hematology Analyzer (XN-1000, SYSMEX, Osaka, Japan). Hematological parameters at the time of admission were recorded. NLR was calculated as neutrophil count divided by lymphocyte count and PLR was calculated as platelet count divided by lymphocyte count.
Statistical Analysis
SPSS 28.0 program was used in the analysis. Mean, standard deviation, median minimum-maximum, frequency, and ratio values were used in descriptive statistics of the data. The distribution of variables was measured with the Kolmogorov Simirnov test. Independent sample t test and Mann-Whitney U test were used to analyze quantitative independent data. Chi-square test was used to analyze qualitative independent data. The effect level was investigated by univariate and multivariate logistic regression. The effect level and cut-off value were investigated by receiver operating characteristic (ROC) curve. Cut-off values were determined by Youden Index. Kappa agreement test was used for agreement analysis. A value of
Results
The main characteristics of the cases are summarized in Table 1.
Demographic and Laboratory Data of the Cases.
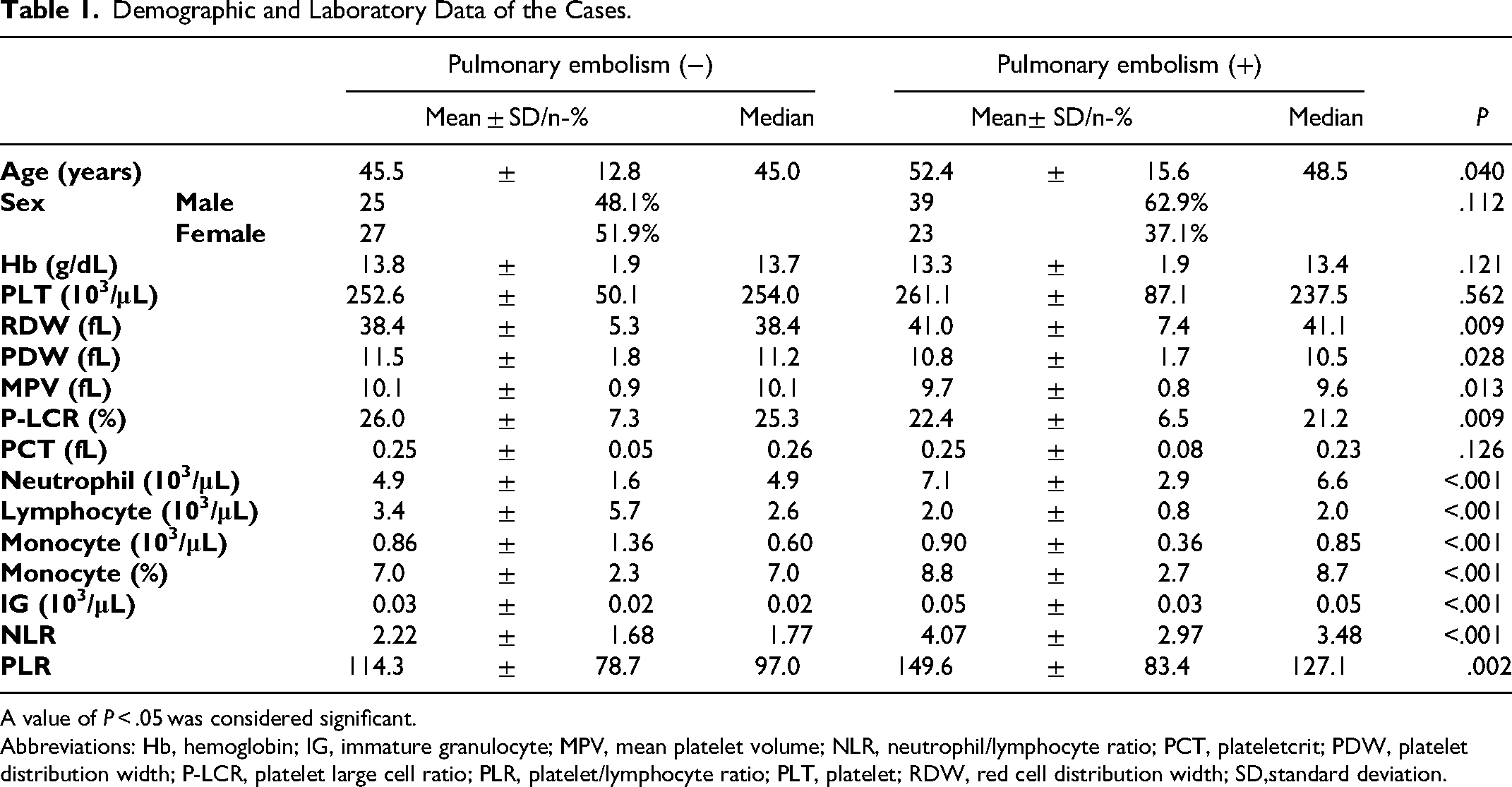
A value of P < .05 was considered significant.
Abbreviations: Hb, hemoglobin; IG, immature granulocyte; MPV, mean platelet volume; NLR, neutrophil/lymphocyte ratio; PCT, plateletcrit; PDW, platelet distribution width; P-LCR, platelet large cell ratio; PLR, platelet/lymphocyte ratio; PLT, platelet; RDW, red cell distribution width; SD,standard deviation.
Sixty-four (56.1%) male and 50 (43.9%) female of 114 cases were evaluated in the study. The mean age of 52 patients without PE was 45.5. The mean age of 62 patients with PE was 52.4 (median 48.5). The age of the cases in the group with PE was significantly higher than the group without PE (P < .05). The gender of the cases in with and without PE did not differ significantly (P > .05).
Red cell distribution width (RDW), neutrophil, monocyte, monocyte %, immature granulocyte (IG), NLR, and PLR parameters were significantly higher in the group with PE than in the group without PE (P < .05). PDW, MPV, platelet large cell ratio (P-LCR), and lymphocyte value were significantly lower in the group with PE than in the group without PE (P < .05). Hemoglobin, platelet, plateletcrit (PCT), and other hemogram parameters were not significantly different in the group with and without PE (P > .05).
Logistic regression analysis of risk factors predicting PE is given in Table 2. Significant and independent efficacy of P-LCR, monocyte %, IG, and NLR values was observed in separating cases with and without PE in the multivariate model (P˂.05).
Logistic Regression Analysis of Risk Factors Predicting Pulmonary Embolism.
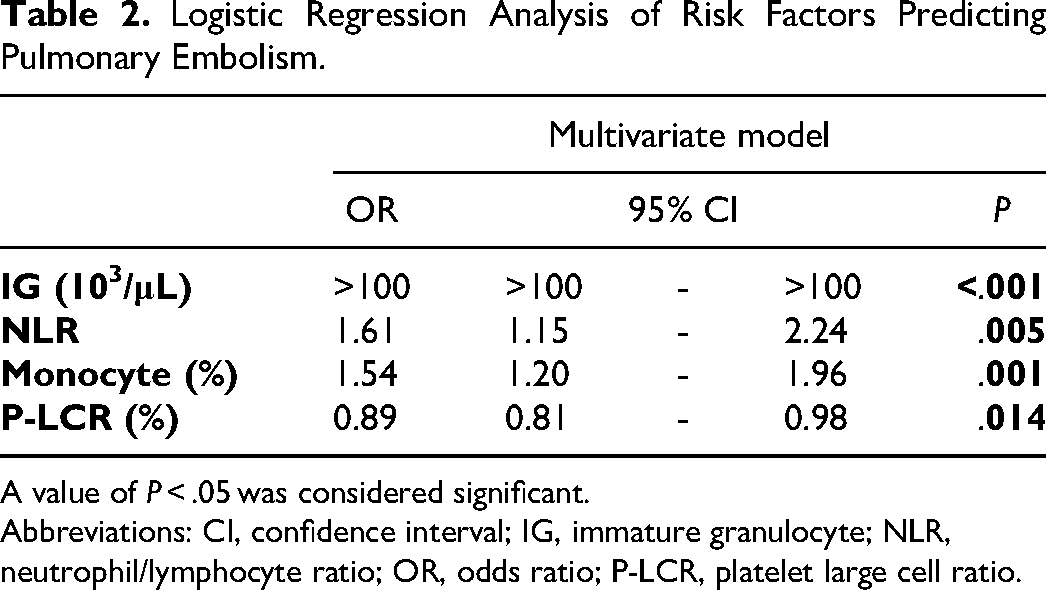
A value of P < .05 was considered significant.
Abbreviations: CI, confidence interval; IG, immature granulocyte; NLR, neutrophil/lymphocyte ratio; OR, odds ratio; P-LCR, platelet large cell ratio.
An ROC curve analysis of IG, NLR, monocytes %, and P-LCR parameters was performed to predict PE (Figure 1). Significant efficiency of IG (area under the curve 0.777 [0.688-0.867]), NLR (area under the curve 0.778 [0.686-0.871]), monocyte % (area under the curve 0.684 [0.581-0.788]), and P-LCR (area under the curve 0.643 [0.537-0.750]) parameters was observed in the differentiation of PE and non-PE cases.
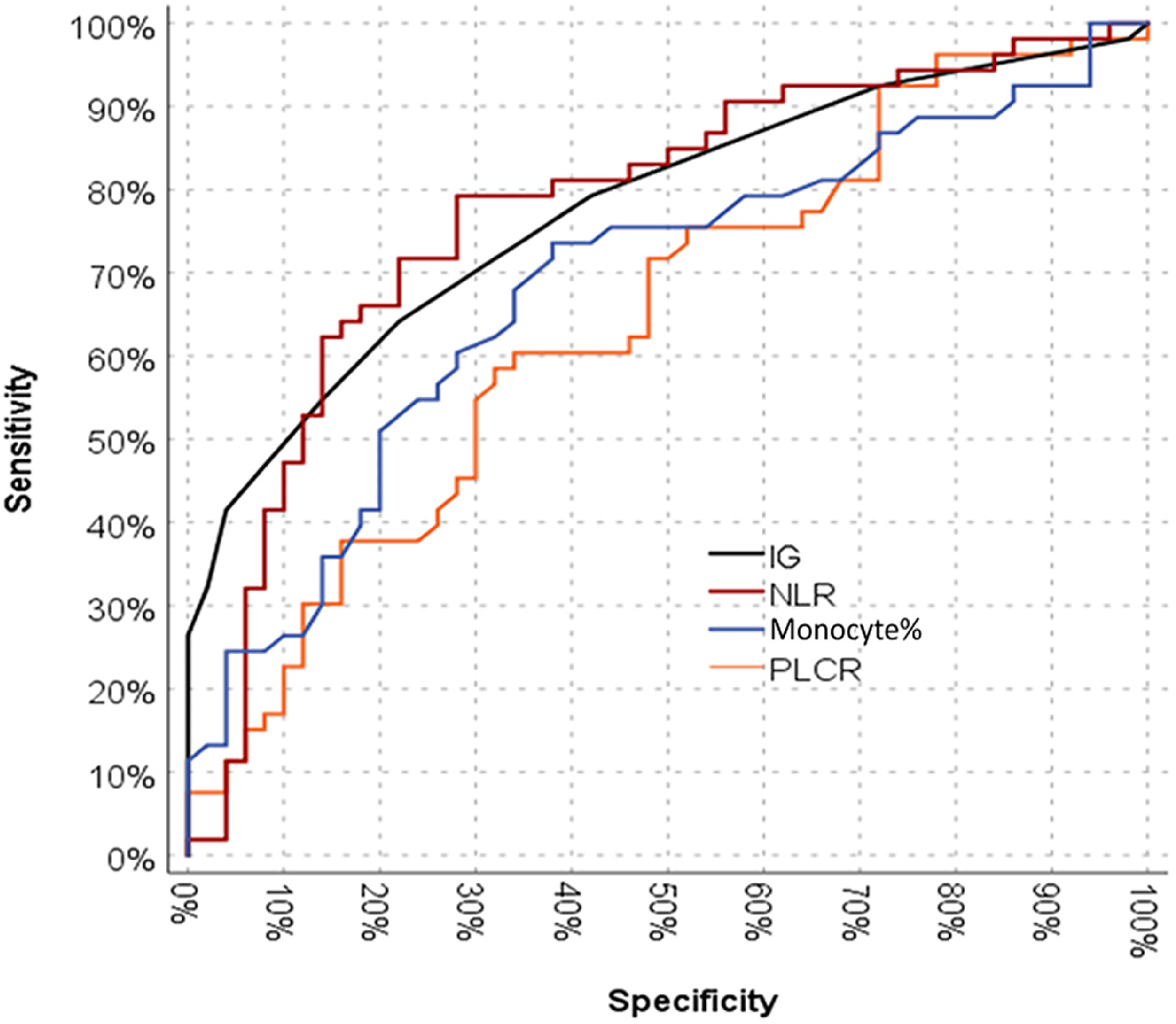
ROC curve of IG, NLR, monocyte %, and P-LCR to predict PE. IG is presented with an AUC of 0.777 with sensitivity of 64.2% and specificity of 76.5%. NLR is presented with an AUC of 0.778 with sensitivity of 80.6% and specificity of 69.2%. Monocyte % is presented with an AUC of 0.684 with sensitivity of 74.2% and specificity of 63.5%. P-LCR is presented with an AUC of 0.643 with sensitivity of 58.5% and specificity of 68%. Abbreviations: AUC, area under the curve; IG, immature granulocyte; NLR, neutrophil/lymphocyte ratio; PE, pulmonary embolism; P-LCR, platelet large cell ratio; ROC, receiver operating characteristic curve.
The cut-off value for IG was 0.035 (sensitivity 64.2% and specificity 76.5%). The cut-off value for NLR was 2.13 (sensitivity 80.6% and specificity 69.2%). The cut-off value for monocyte % was 7.25 (sensitivity 74.2% and specificity 63.5%). The cut-off value for P-LCR was 22.05 (sensitivity 58.5% and specificity 68.0%).
The relationship between IG, NLR, monocyte %, and P-LCR parameters and the probability of PE is shown in Figure 2. It was observed that the probability of PE increased as IG, NLR, and monocyte % increased. It was observed that as P-LCR decreased, the probability of PE increased.
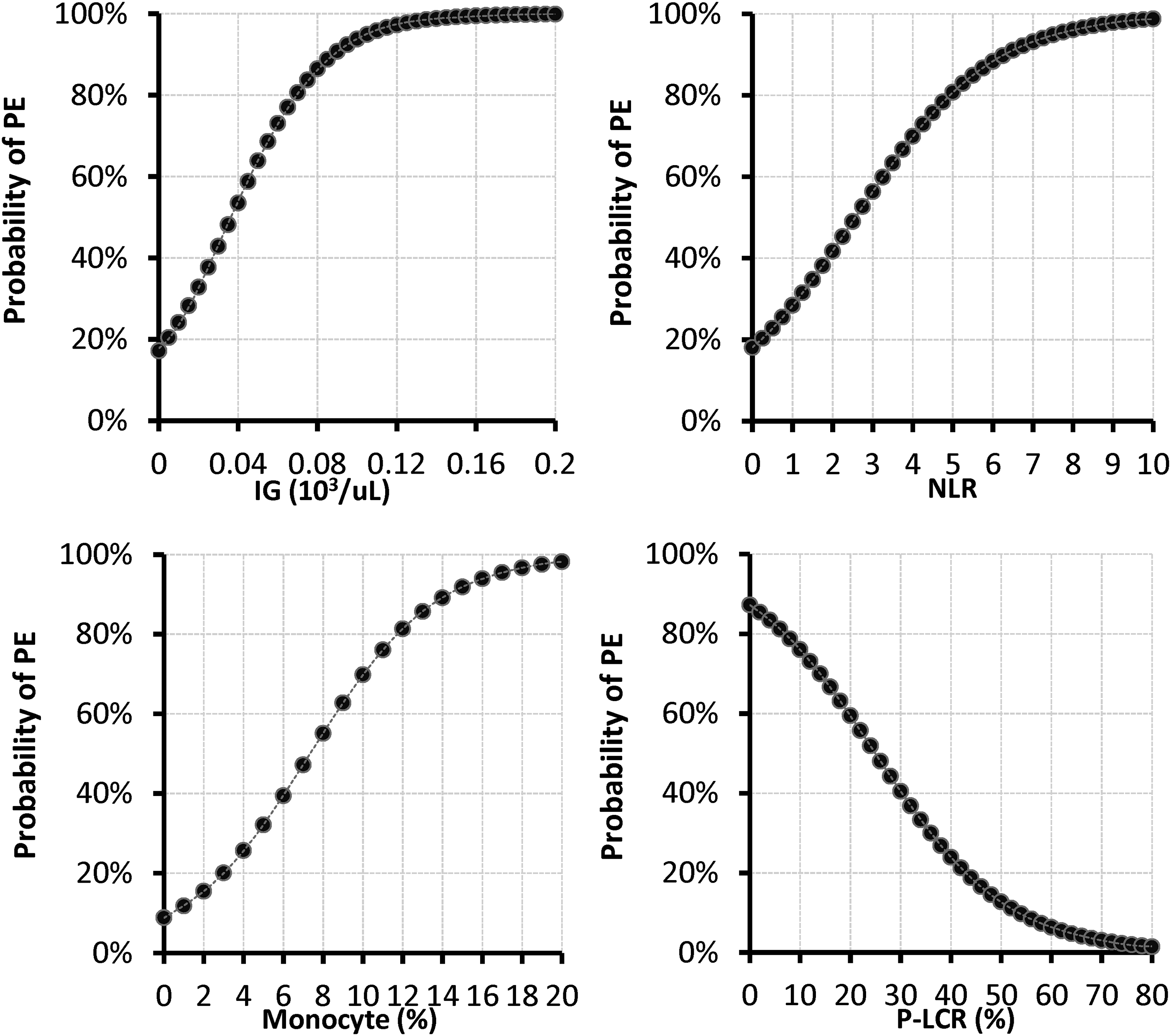
IG, NLR, monocyte %, and P-LCR values to estimate the probability of PE. Abbreviations: IG, immature granulocyte; NLR, neutrophil/lymphocyte ratio; PE, pulmonary embolism; P-LCR, platelet large cell ratio.
Discussion
In our study, the role of potential inflammatory hemogram parameters in the diagnosis of PE was investigated. We found a significant and independent relationship between IG, NLR, monocyte %, and P-LCR values in predicting PE.
IG are neutrophil precursors including metamyelocytes, myelocytes, and promyelocytes and high IG values indicate an enhanced bone marrow activity.10,11 It has been previously investigated as a prognostic inflammatory parameter in sepsis, acute respiratory distress syndrome, pancreatitis, coronavirus disease 2019 (COVID-19).11–13 Kong et al 14 found that immature granulocytes were associated with early mortality in PE. However to our knowledge, IGs have not been investigated in the diagnosis of PE. In our study, we found that IG count was a significant and independent parameter in the diagnosis of PE. High IG count in hemogram may be a new inflammatory parameter in the diagnosis of PE.
In PE, there is evidence of neutrophil and macrophage infiltration in the pulmonary artery wall. 15 The inflammatory response from platelets, leukocytes, and endothelial cells leads to an increase in platelet activation and neutrophil recruitment.7,16,17 In some studies conducted in this context, NLR and PLR were found to be significant in PE severity assessment.7,18 We have not yet identified enough research in diagnostic evaluation. In one study, NLR was found to be a significant parameter in the diagnosis of venous thromboembolism (VTE) while PLR was not evaluated. 19
Although Çelik et al 20 found these 2 parameters higher in the PE group they did not find a significant relationship in the diagnosis of PE. In our study, we found NLR as a significant and independent parameter in predicting PE. NLR may be a guide in diagnosis as well as in PE severity.
Monocytes are known to express tissue factor, represent approximately 30% of leukocytes in venous thrombus and are involved in the modulation of venous thrombus resolution. 21 Monocyte count has been investigated in studies to assess the severity of PE and it has been emphasized that it may have some predictive value for VTE. 22 Wypasek et al 23 found that VTE was associated with increased monocyte count. Rojnuckarin et al 24 found that monocyte counts were significantly higher in solid tumor patients with VTE compared to patients without VTE. These studies were not specific for PE. In our study, we found a significant and independent relationship between the increase in monocyte percentage and the presence of PE. Our findings and the literature suggest that the number and percentage of monocytes in hemogram may be a parameter worth investigating in the diagnosis of PE.
One of the key factors for the development of PE is the contribution of platelet to clot formation. 25 Thrombus formation is the result of abnormalities of blood flow, vascular wall, and blood components. Inflammation causes endothelial damage and affects blood components by increasing procoagulants and inhibiting anticoagulant pathways.25–27 From this point of view, platelet indices which are markers of platelet activation, may guide the diagnosis of PE.
Braekkan et al 25 identified high MPV as a risk factor for unprovoked PE in their study. However in some studies no significant association was found between MPV and PE diagnosis.28,29 In their systematic review, Lin et al 3 stated that although MPV is predictive in the diagnosis and severity assessment of PE, there may be research results resulting from different effects of MPV in patients with different risk levels for PE. In another study, Moharamzadeh et al 30 found no increase or difference in MPV, PDW, and P-LCR among platelet indices in patients with PE.
In our study, we did not find a significant relationship between the diagnosis of PE and platelet markers such as MPV, PDW, and PCT. However there was a significant and independent relationship between the diagnosis of PE and low P-LCR. P-LCR is the percentage of all platelets with a volume greater than 12 fL in the bloodstream and appears to be more sensitive to changes in platelet size than MPV.5,31 This parameter which has not been adequately researched about PE, may guide the diagnosis of PE.
The biomolecular mechanism underlying the association between RDW and PE is unknown and is thought to be due to its association with acute inflammatory markers and changes in blood viscosity. 32 It has generally been investigated as a prognostic marker, but Çelik et al 20 found that RDW predicts the diagnosis of PE with high specificity. To our knowledge, this parameter has not been investigated in another study in terms of PE diagnosis. In our study, we found no significant association between RDW and the presence of PE. This result shows that the available evidence is insufficient for the evaluation of the diagnostic value of RDW.
Our study had some limitations: being retrospective, exclusion of a high number of patients because hemogram parameters are affected by many diseases, and being single centered. However, its strengths include reviewing many parameters emphasized to be missing in the literature and mentioning new parameters that have not been investigated. New markers and prospective, multicenter studies are needed to confirm or exclude PE.
Conclusion
In conclusion, this study examined the relationship between parameters that can be obtained from complete blood count and the diagnosis of PE. We found that high IG, high NLR, high monocyte %, and low P-LCR values have diagnostic value in suspected PE cases. The usability of IGs in the diagnosis of PE is a new finding. However further research is needed to determine its reliability and stability. In this way, physicians can increase their vigilance with hemogram data to detect suspected PE.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Because all patient data were de-identified in this retrospective study, patients’ informed consent was waived.
Author Contribution
GK contributed to writing—original draft, formal analysis, data curation, and conceptualization; OG to writing—review & editing, formal analysis, and conceptualization; EA to writing—review & editing, methodology, and formal analysis; BK to review & editing, visualization, and conceptualization; GS to review & editing and visualization; and MD to formal analysis and data curation.