
Abstract
Introduction
Early Primary percutaneous coronary intervention (pPCI) is the preferred reperfusion therapy for most patients with ST-segment elevation myocardial infarction (STEMI), and the European guidelines recommend pPCI to occur within 120 min of first medical contact. However, this is not always available.
Methods
We performed a retrospective study of patients admitted for STEMI to a level I cardiac intensive care unit in a developing country, to analyze the efficacy of the pharmaco-invasive (PI) strategy versus late PCI over a 2-year follow-up.
Results
Four hundred and thirty-nine STEMI patients presented within the first 12 h of symptom onset, pPCI was performed in 154 patients, PI-strategy in 185 patients, and finally Late PCI in 100 patients. All-cause mortality at 2-year risk was statistically significant associated with cardiogenic shock during initial hospitalization, LM and ostio-proximal left anterior descending artery as the culprit artery, severe conductance disorders requiring the use of a temporary pacemaker, and acute kidney disease with glomerular filtration rate < 30 ml/min/1.72 m2 . For the revascularization strategy, there as a well-demonstrated benefit of the pPCI versus Late PCI strategy with (hazard ratio (HR) = 0.293; 95% confidence interval (CI) 0.11–0.737; P = 0.009), as well as a benefit of the PI-strategy versus Late PCI strategy with (HR = 0.433; 95%CI 0.21–0.87; P = 0.02). However, there was no difference between the pPCI and PI-strategy.
Conclusion
The PI-strategy remains a reasonable alternative for pPCI when the latter is not available, with a prognosis almost identical to pPCI in the long term whenever patients are treated early after the onset of symptoms.
Introduction
Primary percutaneous coronary intervention (pPCI) is the preferred reperfusion therapy for most patients with ST-segment elevation myocardial infarction (STEMI). 1 European guidelines recommend pPCI to occur within 120 min of first medical contact (FMC). 2
Due to the location of some patients developing STEMI with respect to pPCI centers, where timely pPCI is not an option, fibrinolytic therapy is recommended. 3 An important subsequent development has been pharmaco-invasive (PI) strategy and with subsequent early angiography/PCI following lytic success. 4 Some data support PI as being equal or better than primary PCI. Other studies indicate that there is a direct link between infarct size and that mortality rates increase the longer it takes to deliver P-PCI. 5
The meta-analysis of Keeley et al 6 reported the superiority of pPCI compared with fibrinolytic therapy, when followed by variable rates of coronary angiography, though the comparison of primary angioplasty and pre-hospital fibrinolysis in acute myocardial infarction (CAPTIM) study, being the first trial comparing pPCI to a PI strategy was not included. 6 This strategy involved emergency angiography and rescue PCI for those who failed pharmacologic reperfusion and, for others, transfer to a PCI facility for early angiography and PCI if indicated. The safety and efficacy of PI PCI compared with pPCI have been supported by the strategic reperfusion early after myocardial infarction trial (STREAM-1) and registry data from Alberta (Canada) and France. Indeed, recent registries from France and Norway reported better outcomes among patients who underwent PI-PCI compared with late pPCI. 2
The aim of our study is to evaluate the late outcome of patients admitted for ACS in the acute phase (<12hours), according to the type of revascularization strategy used.
Materials and Methods
Rationale and Design of the Study
The rationale for our study is based on the idea that pPCI cannot be offered to all patients, especially in countries with limited resources, and given that the time to revascularization in myocardial infarction is a determining factor in prognosis, thrombolysis may be a therapeutic alternative, although its efficacy in terms of successful revascularization is much lower than that of primary angioplasty, and with more significant hemorrhagic events. For these reasons, there is debate about the true benefit of a so-called PI strategy, which consists of thrombolysis of patients presenting with STEMI within the first 12 h after the onset of symptoms, followed by facilitated angioplasty within 24 h of admission, versus the strategy referred to as delay, which consists of delayed PCI (late PCI) within 24 h.
We conducted a retrospective study over a period of 4 years, which included patients admitted to a cardiac intensive care unit (CICU) for STEMI within the first 12 h after the onset of symptoms, and who had undergone revascularization by angioplasty, pPCI, LatePCI, or as a PI strategy.
Study Population
Among the patients included in our study, we defined three groups of patients: Firstly, those who had undergone pPCI with a door-to-balloon time of less than 120 min after the FMC, then the group who had undergone LatePCI with a door-to-balloon time of >120 min and who had not received thrombolytic treatment either because of a medical decision or because the patient refused, and finally, patients who first received thrombolytic treatment with intravenous tenecteplase, respecting the contra-indications as well as the doses, which were adjusted according to the patient's weight and age followed by PCI within 24 h. Patients who died within 24 h of admission were excluded from the study.
Outcomes
The primary endpoint of our study was all-cause mortality after 2 years. The secondary endpoint is a composite of major hemorrhagic and ischemic events and cardiogenic shock during hospitalization, and readmission for myocardial infarction during follow-up. Events were recorded and collected from patient follow-up by the doctors in charge, or by a family contact or the patient himself/herself for the primary endpoint, and from the patients’ electronic medical records for the secondary endpoints.
Statistical Analysis
The categorical variables were reported as numbers and percentages, then Pearson's chi-square test or Fisher's exact test was used for comparison between the different groups. For continuous variables, normality was first analyzed using the Shapiro–Wilk test, then the variables were reported as mean and standard deviation (SD) or median and interquartile range and compared using the t-student test or non-parametric tests depending on whether or not the distribution was normal.
All-cause mortality at 2 years was studied using a Cox proportional hazards regression model to estimate hazard ratios (HRs) and 95% confidence intervals (CIs), adjusting for variables described in the literature as predictors of mortality. Kaplan–Meier analysis was used to compare mortality rates and readmission for re-infarction between the different groups, with significance between groups being assessed by the log-rank test (Mantel-Cox). All P-values were calculated using two-sided tests, and P-values less than 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS version 26 (SPSS, Inc., Chicago, IL).
Ethical Approval
This study did not require formal ethics approval. Access to patient data was authorized by the Mohammed VI University Hospital and approved by the head of department, given the retrospective design of this study. The requirement for patient consent was waived. Data anonymity was respected in accordance with national and international guidelines.
Results
General Characteristics
Between March 2017 and March 2021, 439 STEMI patients presented within the first 12 h of symptom onset, pPCI was performed in 154 patients, PI-strategy in 185 patients, and finally Late PCI in 100 patients.
The mean age between the different groups varied between 60.8 years (SD = 10) and 63.57 years (SD = 10.5) (P < 0.103), with a male predominance (P = 0.026).
The mean time between onset of symptoms and consultation was 6.14 h (SD = 2.66) in the pPCI strategy, 5.55hours (SD = 2.55) in the PI-strategy, and 7.66 h (SD = 3.08) in those who underwent late PCI (P < 0.09). (Table 1).
Showing the General Characteristics of Patients According to Revascularization Strategy.

Bold indicates the result is significant.
Abbreviations: LAD, left anterior descending artery; RCA, right coronary artery; LCX, left circumflex artery; GFR, glomerular filtration rate.
Hypertension and type II diabetes were the most frequent risk factors in our cohort, accounting for 32.6% and 33% respectively, with no significant difference between the different strategies. Previous coronary artery disease was found in 23 patients.
The mean of length of stay of our patients in the CICU ranged from 3.45 days (SD = 1.35) to 4 days (SD = 2.24) (P < 0.063). On admission to the CICU, 30 patients were in acute heart failure with KILLIP stage III or IV, ie, 6.8%. (P < 0.44). The ECG showed persistent ST-segment elevation, mainly in the anterior territory, followed by the inferior territory and finally the lateral territory, with respective percentages of 56.9%, 41%, and 9.8%. Right ventricular infarction was associated with 58 patients.
On echocardiography, the mean ejection fraction (EF) at discharge was 47.35% (SD = 11.99) in the pPCI strategy, 45.95% (SD = 9.98) in the PI-strategy, and 47.13% (SD = 10.28) in the late pPCI strategy. Left ventricular systolic dysfunction with an EF < 35% at discharge was present in 72 patients, ie, 16.4% (Table 1).
At coronary angiography, 334 patients had a significant lesion of left anterior descending artery (LAD), 215 patients had a right coronary artery (RCA) with a significant lesion, the left circumflex artery (LCX) was stenotic or occluded in 137 patients, and the left main (LM) in 13 patients. Multivessels disease was present in 195 patients (44.4%). For the culprit artery, LAD came first, followed by the RCA, the LCX and finally the LM.
Coronary flow was restored in 280 patients, ie, 63.8% between the different groups, with the majority of patients having benefited from a PI-strategy (P < 0.001). It should be noted that 89.2% of patients who benefited from a PI-strategy had an open artery with a TIMI (thrombolysis in myocardial infarction) II or III flow before PCI (Table 1).
Biological work-up revealed anemia in 16.9% of patients admitted, and acute kidney disease with a glomerular filtration rate (GFR) of less than 30 ml/min in 11.8%, with no difference between the different strategies. With regard to intra-CICU management, there was no difference between the different groups in the use of vasopressor drugs (P = 0.539), the use of a central line (P = 0.348), and the use of a temporary pacemaker (P = 0.432) (Table 1).
During the stay in the CICU, 28 patients developed acute heart failure requiring oxygenation support with injectable diuretics, with no impact on the revascularization strategy (P = 0.659). Threatening arrhythmias were observed in 15 patients (P = 0.27), severe conductance disorders in 21 patients (P = 0.674), mechanical complications in four patients (P = 0.156), and finally in-hospital mortality in seven patients, again with no impact of the type of revascularization strategy (P = 0.708) (Table 1).
Outcomes study (Table 2)
For the primary outcome, 38 deaths from all causes at 2 years were noted, ie, 8.7% of all patients, with 1.4% in the pPCI strategy, 3% in the PI strategy, and 4.3% in the Late pPCI strategy, with a significant difference between the different groups (P < 0.001). The Kaplein–Meier survival analysis showed a significant difference in survival rate with a significant Lok-rank test (P = 0.005) (Figure 1, Table 2).
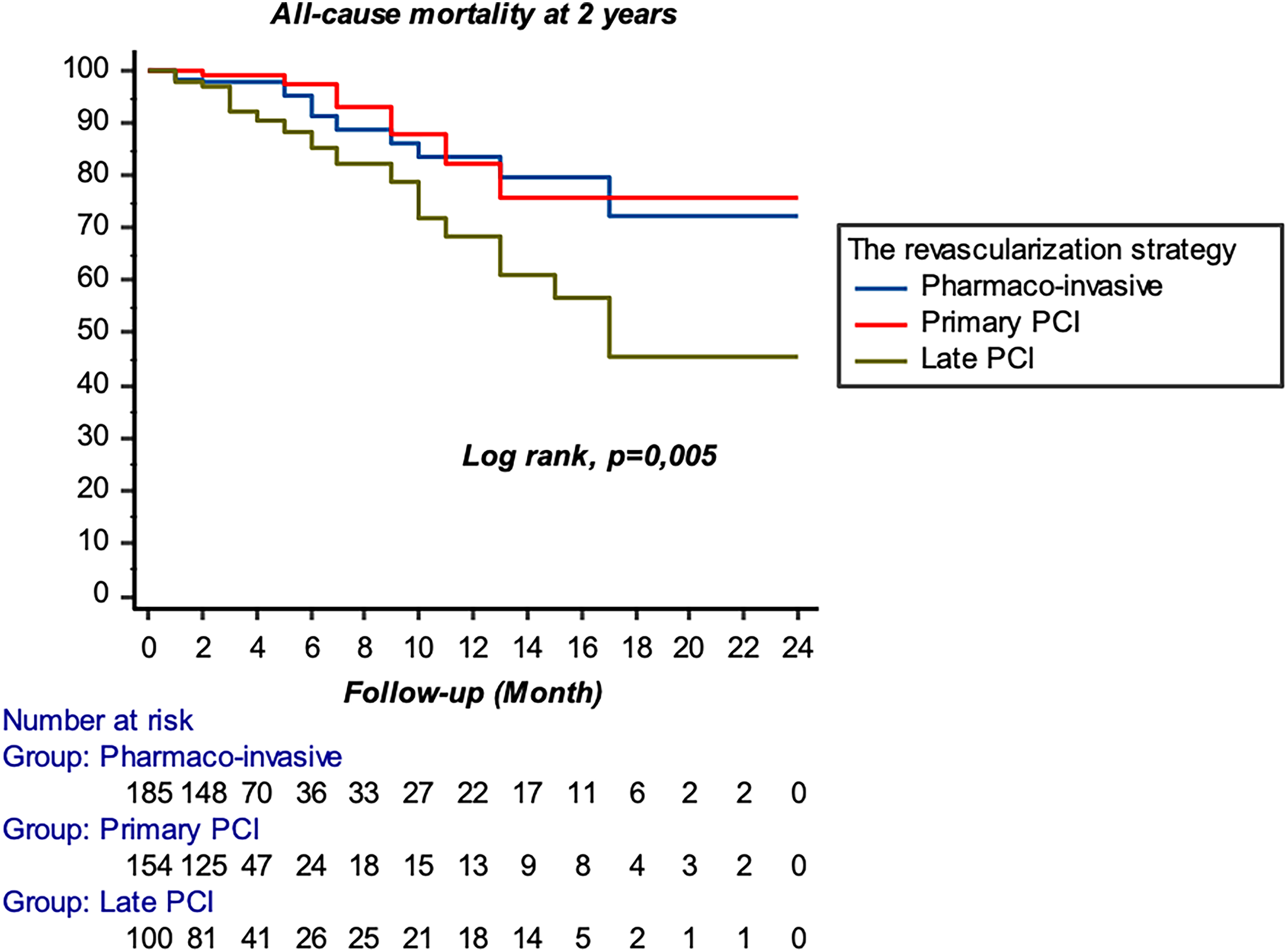
Kaplan–Meier curve for all-cause mortality at 2 years according to revascularization strategy.
Showing Primary and Secondary Composite Outcomes of Patients According to Revascularization Strategy.

Bold indicates the result is significant.
For the secondary outcome, 26 patients were readmitted for a new myocardial infarction during the follow-up period, with 0.9% in the pPCI strategy, 2.1% in the PI-strategy, and 3% in the Late PCI strategy, with a difference between the different groups (P = 0.002). Similarly, for the primary outcome, the Kaplein–Meier survival analysis showed a significant difference with a Lok-rank test á (P = 0.02) (Figure 2, Table 2).

Kaplan–Meier curve for readmission for myocardial infarction at 2 years as a function of revascularization strategy.
For serious ischemic and hemorrhagic events, as well as in-CICU cardiogenic shock, there was no significant difference with respective P-values of 0.819, 0.64, and 0.78 between the different strategies (Table 2).
Multivariable Analysis
For the primary outcome, the factors associated with a statistically significant risk of all-cause mortality at 2 years were cardiogenic shock during initial hospitalization (HR = 5.75; 95%CI 1.47–9.92; P = 0.001), LM and ostio-proximal LAD as the culprit artery (HR = 2. 86; 95%CI 1.28–6.41; P = 0.01), severe conductance disorders requiring the use of a temporary pacemaker (HR = 4.83; 95%CI 1.94–6.14; P = 0.004), and acute kidney disease with a GFR < 30 ml/min/1.72 m2 (HR = 3.81; 95%CI 1.45–7.05; P = 0.007) (Table 3).
Showing the Results of Multivariate Regression-Adjusted Analysis of Cox Proportional Risks for all-Cause Mortality at 2 Years According to Revascularization Strategy

Bold indicates the result is significant.
Abbreviation: GFR, glomerular filtration rate.
For the revascularization strategy, there was a well-demonstrated benefit of the pPCI versus Late PCI strategy with (HR = 0.293; 95%CI 0.11–0.737; P = 0.009), as well as a benefit of the PI-strategy versus Late PCI strategy with (HR = 0.433; 95%CI 0.21–0.87; P = 0.02). However, there was no difference between the pPCI and PI-strategy with (HR = 0.676; 95%CI 0.25–1.78; P = 0.429) (Table 4).
Showing the Results of Comparison Between the Different Strategies for the Main Outcome According to Cox Regression.

Abbreviation: LAD, left anterior descending artery.
Discussion
Since the introduction of PCI, the revascularization strategy for STEMI has been revolutionized, with pPCI demonstrating its effectiveness, as shown by the results published in the landmark meta-analysis by Keeley et al. 1 However, this procedure is not always available, since the proportion of patients treated after 120 min from the onset of symptoms and after the diagnostic ECG ranges from 25% to 50%, depending on the country and the organization of care. 3
Other strategies have been proposed, with the common aim of restoring coronary flow while awaiting PCI. These include PI-strategy or, as an alternative, Late PCI. If the choice between these three strategies is mainly in favor of pPCI, then the debate still remains between the PI-strategy and the Late PCI strategy, in the case of non-availability of a pPCI. 7
In the study by Javeria et al, which included 2091 patients with STEMI within 12 h of symptom onset who underwent PCI during hospitalization at Liverpool Hospital (Sydney), the mortality rate during follow-up was higher in patients who underwent late PCI compared with those who underwent a PI-strategy; however, the rates of re-infarction, ischemic stroke, intracranial hemorrhage and major hemorrhage were similar between the two reperfusion strategies. 8
Doo Sun Sim and his team used the Korean acute myocardial infarction registry to compare two groups of patients who received either a PI-strategy defined as fibrinolysis followed by PCI (n = 708) versus the late PCI (n = 8878). In this study, patients who received a PI-strategy benefited from a shorter reperfusion time and a greater permeability of the culprit vessel compared with patients who had late PCI, but with a similar clinical outcome at 12 months. 9
In the Canadian STEMI registry, among the 5583 STEMI patients in the Alberta Vital Heart Response program, they compared two groups, 3287 patients who received a PI-strategy with tenecteplase and a group who received Late PCI, a PI-strategy was associated with better ST-segment resolution and better outcomes at 1 year compared to late PCI. 10
The STREAM-2 (Strategic Reperfusion Early after Myocardial Infarction) trial randomized 604 patients with STEMI within 3 h of symptom onset and unable to receive pPCI within this timeframe to late PCI or Tenecteplase fibrinolysis followed by early coronary angiography within 6–24 h. Composite of all-cause death, shock, heart failure, and recurrent MI at 30 days were similar in the fibrinolysis and PPCI groups (12.8% vs 13.3%), but given the limited follow-up time of 1 month, this trial is still very limited. 11
In a large Norwegian prospective registry of patients admitted for STEMI, Kvakkestad et al studied the characteristics and short- and medium-term prognosis of 3534 (87%) patients treated with pPCI and 527 (13%) treated with PI-strategy, with 30-day mortality and long-term survival as primary outcomes. The results showed no difference in 30-day mortality between the two strategies, but the PI-strategy group was associated with better overall survival than the pPCI group during 8-year follow-up, even after adjustment (HR adjusted at 0.72; 95% CI 0.53 to 0.99). 12
These results allow us to deduce that the PI-strategy can be an effective alternative option for the treatment of STEMI when primary angioplasty is not readily available, particularly in patients with early symptoms, since this strategy reduces the time and size of ischemia, and therefore a good prognosis, especially in the middle and long term.
Conclusion
Early revascularization in STEMI remains the keystone of treatment, and this through pPCI. However, the latter is not always available, so the PI-strategy remains a reasonable alternative, with a prognosis almost identical to pPCI in the long term whenever patients are treated early after the onset of symptoms.
Footnotes
Author Contributions
S.B and A.B developed the project idea, writing and revising the proofs. ZB, NI and NE supervised the project. All authors contributed to the article and approved the submitted version.
Data Availability
The data underlying this article are available in the article and in its online Supplemental material.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.