
Abstract
Aim:
We aimed to investigate the 6-month efficacy and safety of postprocedural 12-hour tirofiban administration versus 24-hour tirofiban administration in patients with ST-segment elevated myocardial infarction (STEMI) who underwent primary percutaneous coronary intervention (PCI).
Methods:
This retrospective study enrolled 349 patients with STEMI who underwent primary PCI. Following the administration of bolus tirofiban after primary PCI, those receiving a 12-hour tirofiban infusion as the maintenance dose were classified as group 1 (n = 123) while those receiving a 24-hour infusion were classified as group 2 (n = 226). In-hospital and 6-month major adverse cardiac events were recorded.
Results:
There were no statistically significant differences between the 2 groups regarding in-hospital efficacy (in-hospital death: 4.4% vs 5.7%, P = .600 and stent thrombosis 1.8% vs 1.6%, P = .921) and in-hospital safety (2.6% vs 1.6% for major bleeding and 5.3% vs 4.1% for minor bleeding, P = .562). During the 6-month follow-up period, the incidence of the recurrent revascularization (16.1% vs 15.5%, odds ratio [OR] = 1.05 [0.47-3.67]), the repeated nonfatal acute coronary syndrome and/or stent thrombosis (27% vs 24.4%, P = .598, OR = 1.02 [0.42-2.48]), and the cardiovascular deaths (6.6% vs 6.5%, P = .943, OR = 1.03 [0.43-2.43]) were comparable between group 1 and group 2.
Conclusion:
Our study revealed that 12-hour tirofiban administration versus 24-hour tirofiban administration in STEMI who underwent primary PCI was similar with respect to in-hospital efficacy and safety and major adverse cardiac events during 6-month follow-up.
Keywords
Introduction
The platelets have a central role in thrombus formation and thus inhibition of the platelet functions is essential to effectively treat the patients with ST-segment elevated myocardial infarction (STEMI) undergoing percutaneous coronary intervention (PCI). 1 Platelet aggregation is the final step in thrombus formation. By inhibiting this step, the glycoprotein IIb/IIIa inhibitors prevent the formation of thrombus in the acute period and reduce the frequency of the adverse cardiovascular (CV) events in the short- and long-term follow-up in patients undergoing PCI. 2,3 Tirofiban, a glycoprotein IIb/IIIa receptor inhibitor, is used commonly in the treatment of patients with STEMI undergoing PCI. 4 There is no established standard duration of tirofiban administration. Although the duration of tirofiban infusion ranged from 12 to 48 hours in the studies, infusion duration was mostly left to the discretion of the primary operator. Consequently, no consensus exists on the duration of tirofiban administration. 5 –7 Long-duration infusion leads to both an increase in the drug-related side effects and the treatment costs. Therefore, a short-duration infusion that would provide the same effect could be more rational. In this study, we aimed to investigate the 6-month efficacy and safety of postprocedural 12-hour tirofiban administration versus 24-hour tirofiban administration in patients with STEMI who underwent primary PCI.
Materials and Methods
Study Population
This study was performed by conducting a retrospective screening of the file records from patients who were referred to our hospital with the diagnosis of acute STEMI within 12 hours after the onset of pain between January 2004 and December 2007 and received tirofiban infusion following primary PCI. A total of 2557 consecutive patients with STEMI were screened to constitute the study population. Patients who did not receive tirofiban (n = 1906) or receiving >24 hours tirofiban infusion (n = 44), patients received thrombolytic treatment (n = 57), those without adequate file data or 6-month follow-up records (n = 66), conservatively treated patients (n = 32), those with left main coronary artery (n = 32) or saphenous graft lesion (n = 25), and those with Killip class 3 to 4 (n = 46) were excluded. Finally, the study population consisted of 349 patients (Figure 1).
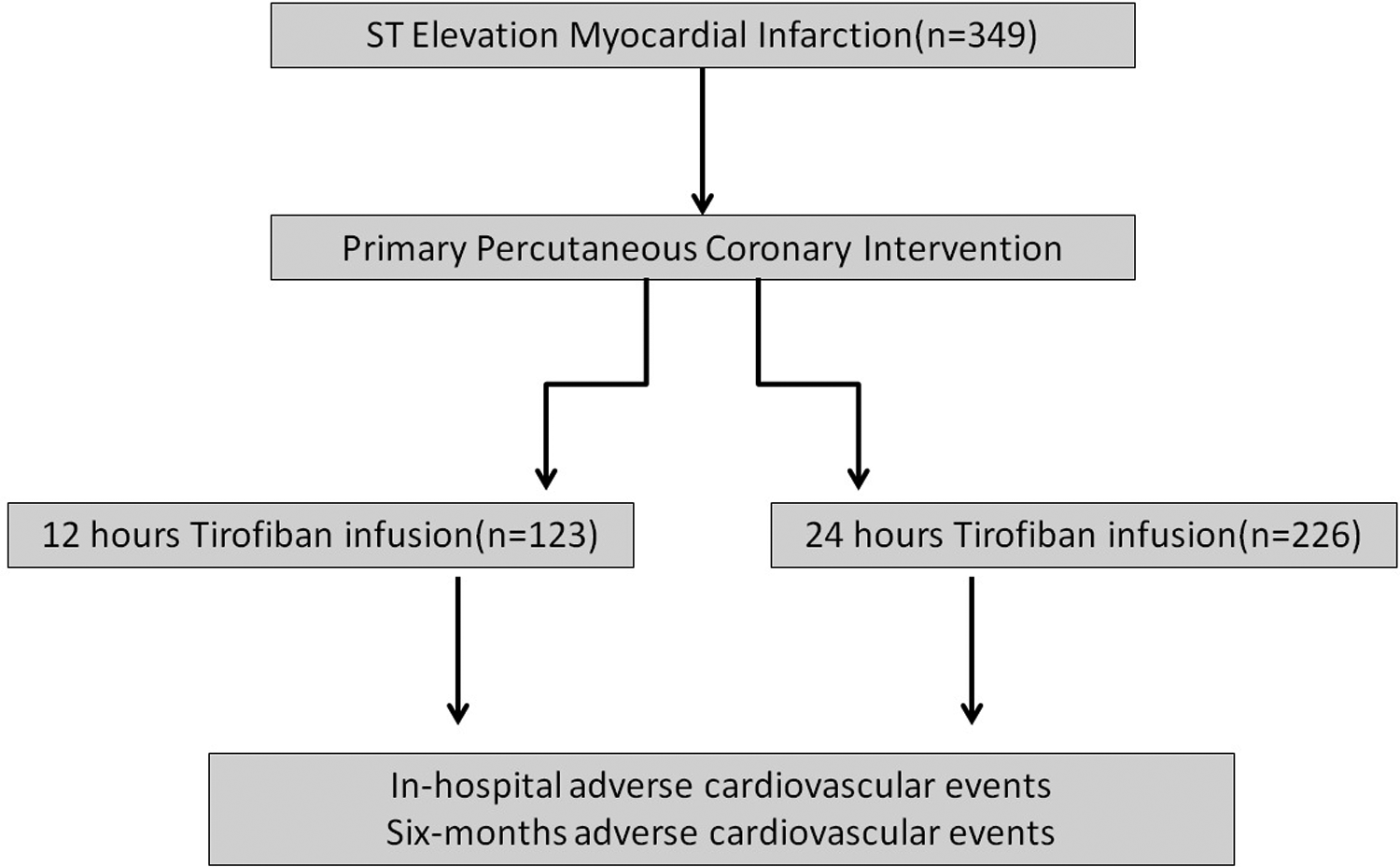
Flow chart of our study.
Tirofiban Infusion and Group Formation
Following the administration of bolus tirofiban after primary PCI (10 μg/kg), those receiving a 12-hour tirofiban infusion as the maintenance dose were classified as group 1 (n = 123) while those receiving a 24-hour infusion were classified as group 2 (n = 226). The maintenance dose was determined to be 0.15 μg/kg/min in both the groups.
Basic Clinical and Biochemical Definitions
The data of the patients concerning age, gender, height, weight, hypertension, diabetes mellitus, family history, dyslipidemia history, previous coronary artery disease history, smoking status, electrocardiography (ECG), lipid profile, creatinine, blood glucose, troponin-I, creatine kinase (CK), and CK-MB at the time of diagnosis were obtained from the patient file records, the hospital database, and the archive data. On the ECGs examined, myocardial infarction (MI) localization sites were classified as anterior and inferior based on the derivations. Hypertension was defined as having at least 2 blood pressure measurements >140/90 mm Hg or using antihypertensive drugs, whereas diabetes mellitus was defined as having at least 2 fasting blood sugar measurements >126 mg/dL, a hemoglobin A1c level above 6.5 mg/dL or using antidiabetic drugs. History of dyslipidemia was defined as the previous use of lipid-lowering drugs or a low-density lipoprotein measured above 100 mg/dL at any time before hospitalization. Body mass index values were calculated based on the height and weight of each patient. The left ventricular ejection fraction was evaluated on the first day of hospitalization. All the lipid parameters from the patients were obtained within the first 8 hours following hospitalization. To detect the peak CK, CK-MB, and troponin values, these enzymes were closely monitored during the intensive care stay.
Angiographic Definitions
All patients underwent primary PCI (stent placement and/or balloon angioplasty) following coronary angiography via standard femoral route. Infarct-related arteries were classified as left anterior descending artery, circumflex artery, and right coronary artery. Coronary flow before and after primary PCI was graded visually according to the following thrombolysis in myocardial infarction (TIMI) classification 8 :
TIMI 0: There is no antegrade flow beyond the point of occlusion.
TIMI 1: The contrast material passes beyond the area of obstruction but “hangs up” and fails to opacify the entire coronary bed distal to the obstruction for the duration of the cineangiographic filming sequence.
TIMI 2: The contrast material passes across the obstruction and opacifies the coronary bed distal to the obstruction. However, the rate of entry of the contrast material into the vessel distal to the obstruction or its rate of clearance from the distal bed (or both) is perceptibly slower than its entry into or clearance from comparable areas not perfused by the previously occluded vessel—for example, the opposite coronary artery or the coronary bed proximal to the obstruction.
TIMI 3: Antegrade flow into the bed distal to the obstruction occurs as promptly as antegrade flow into the bed proximal to the obstruction, and clearance of contrast material from the involved bed as rapid as clearance from an uninvolved bed in the same vessel or the opposite artery.
The Definition of the In-Hospital and 6-Month Adverse CV Events
The diagnosis of stent thrombosis was made according to the Academic Research Consortium definitions, including definite, probable, or possible. 9 The determination of definite stent thrombosis required the presence of a coronary syndrome with angiographic or autopsy evidence of thrombus or occlusion. Probable stent thrombosis included unexplained deaths within 1 month after the procedure or acute MI involving the target-vessel territory without angiographic confirmation, and possible stent thrombosis was described as unexplained death occurring after 30 days.
Bleeding events were classified in accordance with the criteria of TIMI classification. 10,11 Thrombolysis in Myocardial Infarction major bleeding was defined as intracranial bleeding or a reduction in the hemoglobin values of >5 g/dL or fatal bleeding (bleeding that directly results in death within 7 days), while TIMI minor bleeding was defined as clinically overt resulting in hemoglobin drop of 3 to 5 g/dL or requiring medical attention.
Statistical Analysis
All the statistical analyses were performed with SPSS 17.0 statistical package software. Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as frequency or percentage. The difference between the numerical variables was measured by independent samples t test or Mann-Whitney U test. Categorical variables were evaluated by chi-square test or Fisher exact test. In all statistical analyses, P < .05 was considered as statistically significant. Kaplan-Meier survival analysis was used to evaluate the 6-month frequency of the adverse CV deaths.
Results
The study population consisted of a total of 349 patients with STEMI who underwent primary PCI (mean age: 57.4 ± 11.4 years and 85.4% males). The basic clinical, biochemical, and angiographic characteristics of group 1 and group 2 are shown in Tables 1 to 3. There were no statistically significant differences between the 2 groups, regarding in-hospital efficacy (in-hospital death: 4.4% vs 5.7%, P = .600 and stent thrombosis 1.8% vs 1.6%, P = .921) and in-hospital safety (2.6% vs 1.6% for major bleeding and 5.3% vs 4.1% for minor bleeding, P =. 562; Table 4 and Figures 2 and 3). Six patients had stent thrombosis during in-hospital follow-up. Among these, 2 were in group 1 while 4 were in group 2. The comprehensive analysis of the patients with stent thrombosis revealed that 2 patients in group 1 and 3 patients in group 2 had stent thrombosis within 24 hours of the primary PCI and 1 patient in group 2 developed stent thrombosis on the third day. Bleeding complication was observed in a total of 25 patients in the overall population. In all, 7 patients in group 1 and 18 patients in group 2 developed bleeding complication. In group 1, 2 patients developed major bleeding (upper gastrointestinal system [GIS] bleeding) and 5 patients developed minor bleeding (access site bleeding and epistaxis). In all, 6 patients developed major bleeding (1 intracranial bleeding, 4 upper GIS bleeding, and 1 lower GIS bleeding) and 12 other patients experienced minor bleeding (access site bleeding, hematuria, and epistaxis) in group 2. The incidence of adverse CV events during the 6-month follow-up is shown in Table 5 and Figures 4 and 5. During the 6-month follow-up period, the incidence of the recurrent revascularization (16.1% vs 15.5%, odds ratio [OR] = 1.05 [0.47-3.67]), repeated nonfatal acute coronary syndrome and/or stent thrombosis (27% vs 24.4%, P = .598, OR = 1.02 [0.42-2.48]), and the CV deaths (6.6% vs 6.5%, P = .943, OR = 1.03 [0.43-2.43]) were comparable between group 1 and group 2.
Baseline Clinical Parameters of Study Population.
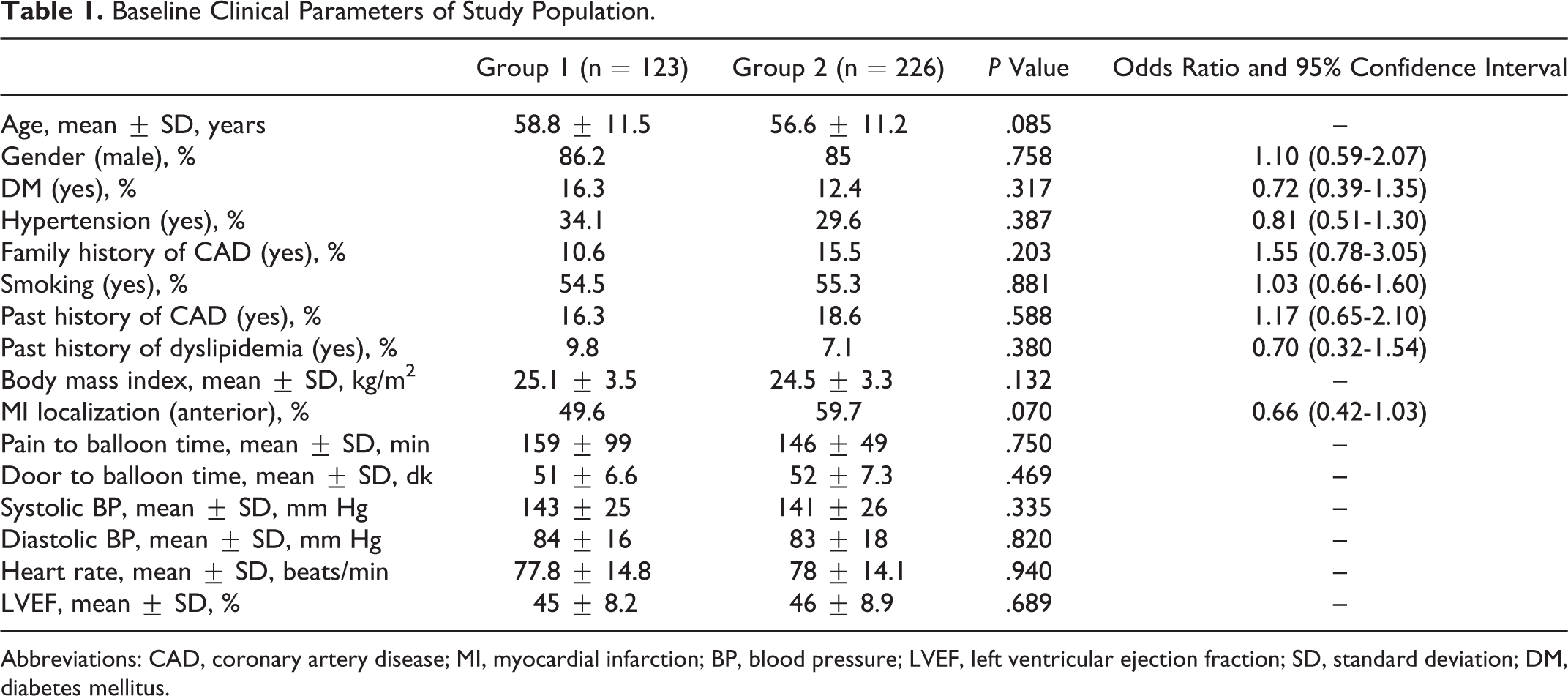
Abbreviations: CAD, coronary artery disease; MI, myocardial infarction; BP, blood pressure; LVEF, left ventricular ejection fraction; SD, standard deviation; DM, diabetes mellitus.
Baseline Biochemical Parameters of Study Population.
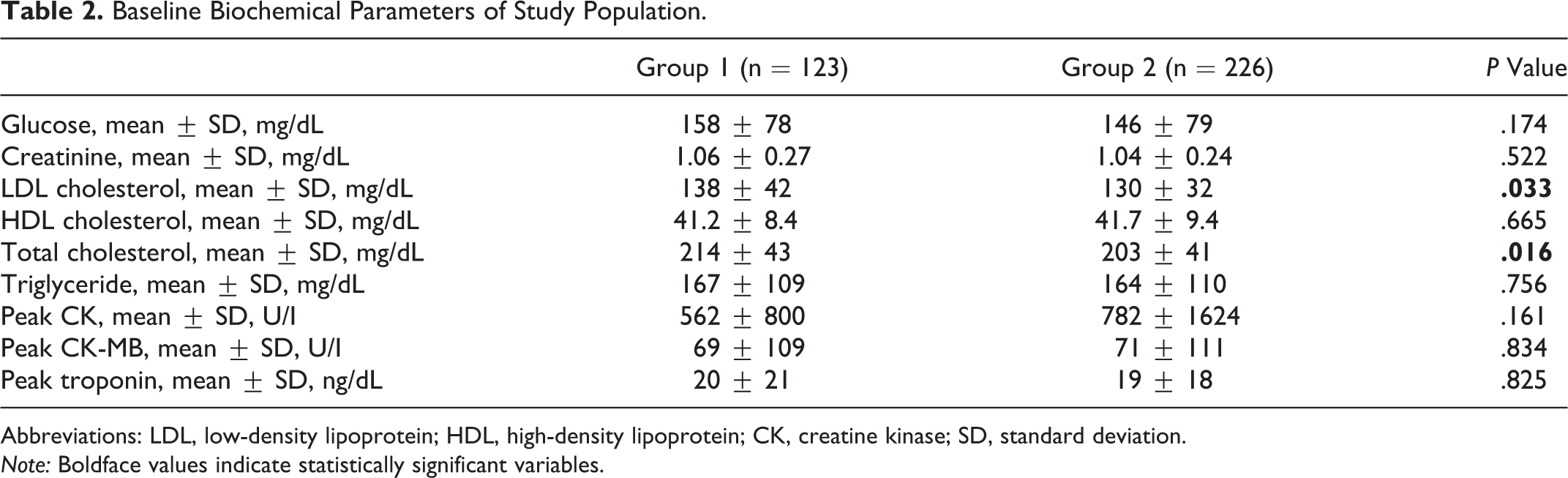
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; CK, creatine kinase; SD, standard deviation. Note: Boldface values indicate statistically significant variables.
Baseline Angiographic Parameters of Study Population.
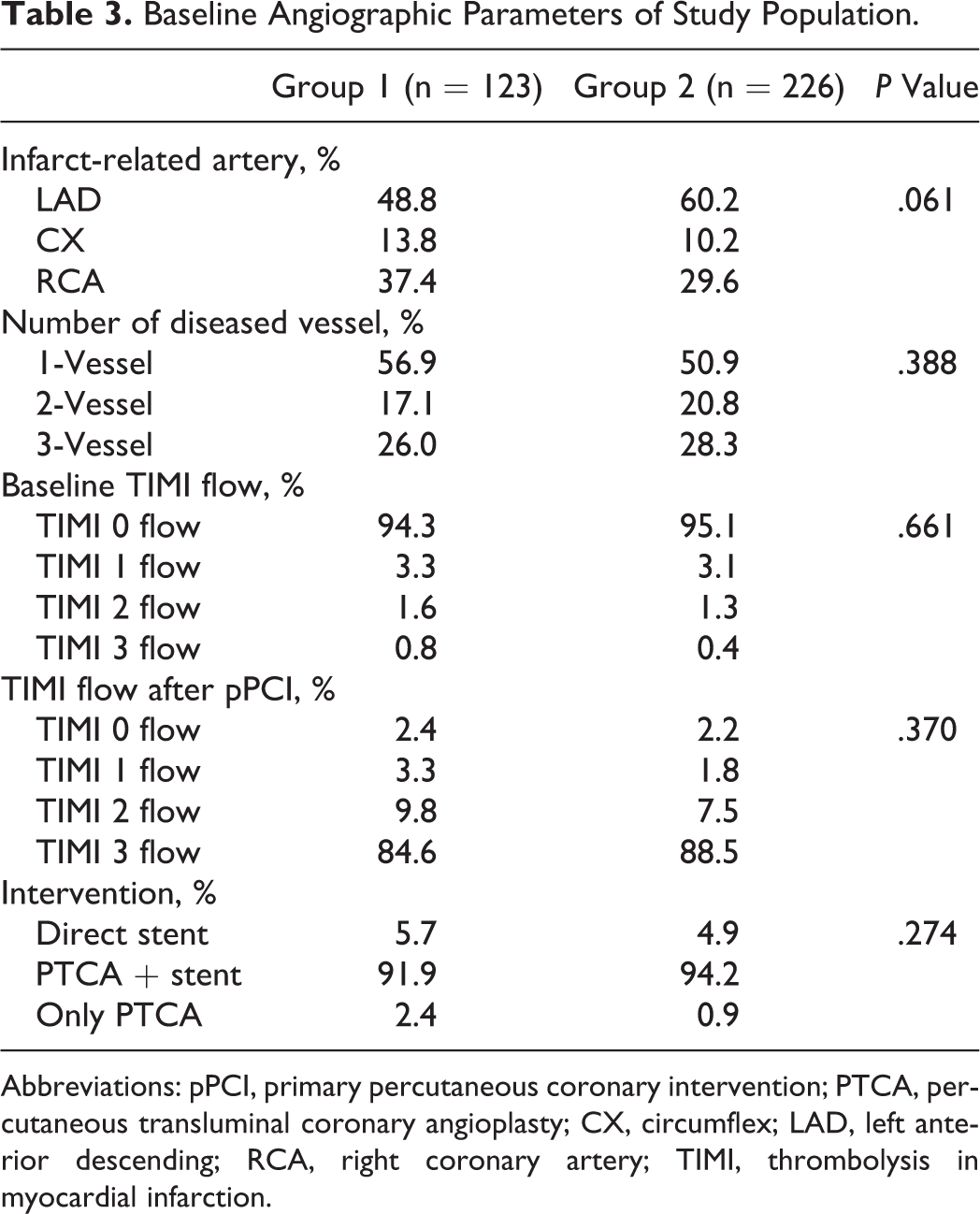
Abbreviations: pPCI, primary percutaneous coronary intervention; PTCA, percutaneous transluminal coronary angioplasty; CX, circumflex; LAD, left anterior descending; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
Comparison of the In-Hospital Complications of Group 1 and Group 2.
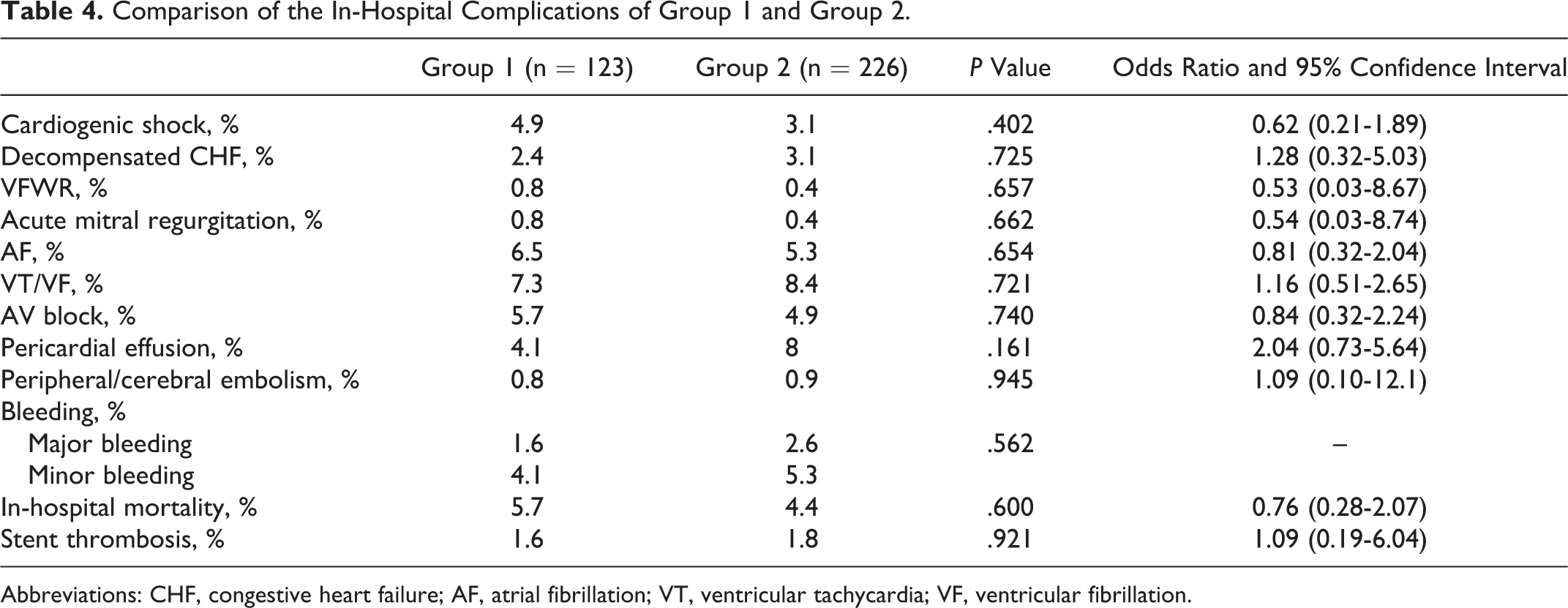
Abbreviations: CHF, congestive heart failure; AF, atrial fibrillation; VT, ventricular tachycardia; VF, ventricular fibrillation.
Comparison of 6-Month Adverse Cardiovascular Events of Study Groups.

Abbreviations: ACS, acute coronary syndrome; ST, stent thrombosis.
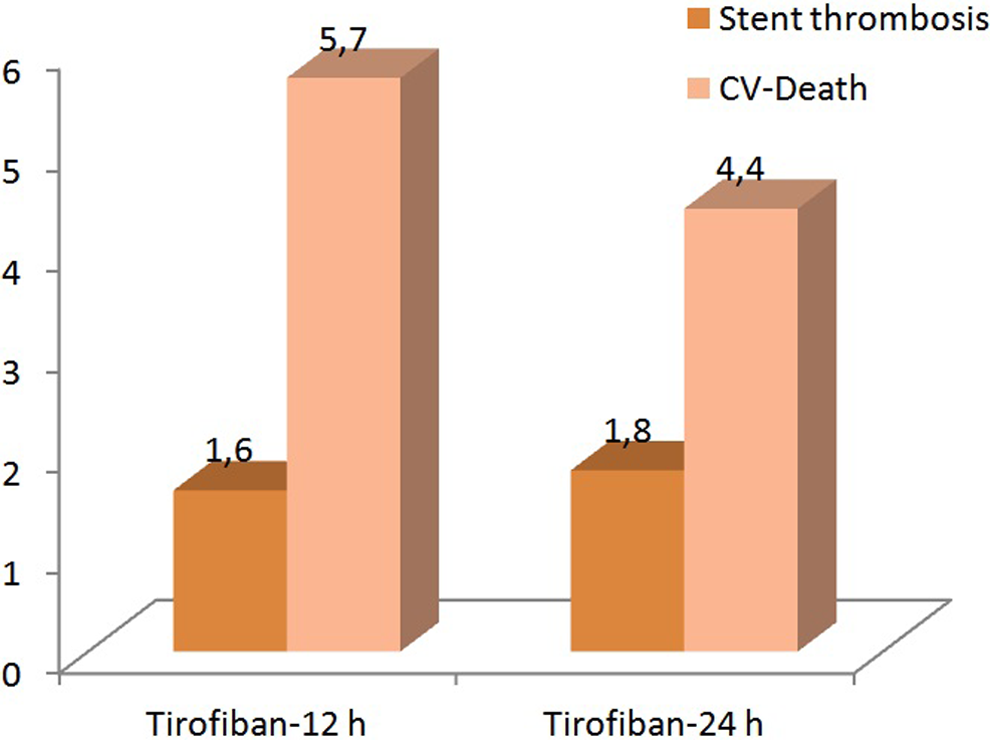
Incidence of in-hospital cardiovascular mortality and stent thrombosis.
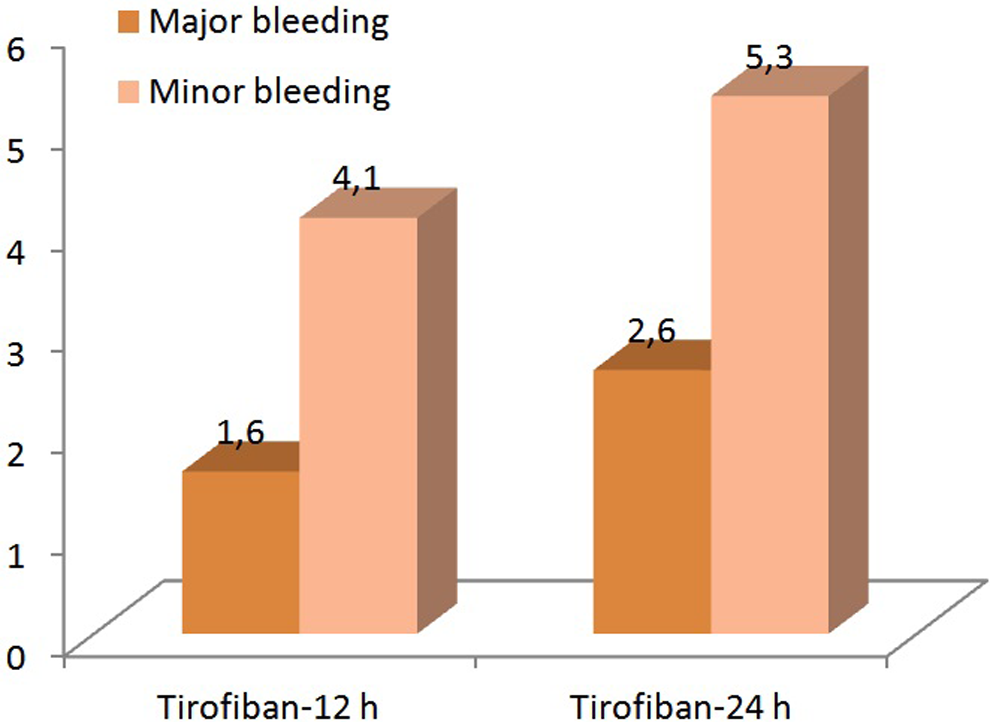
Incidence of in-hospital major and minor bleeding.
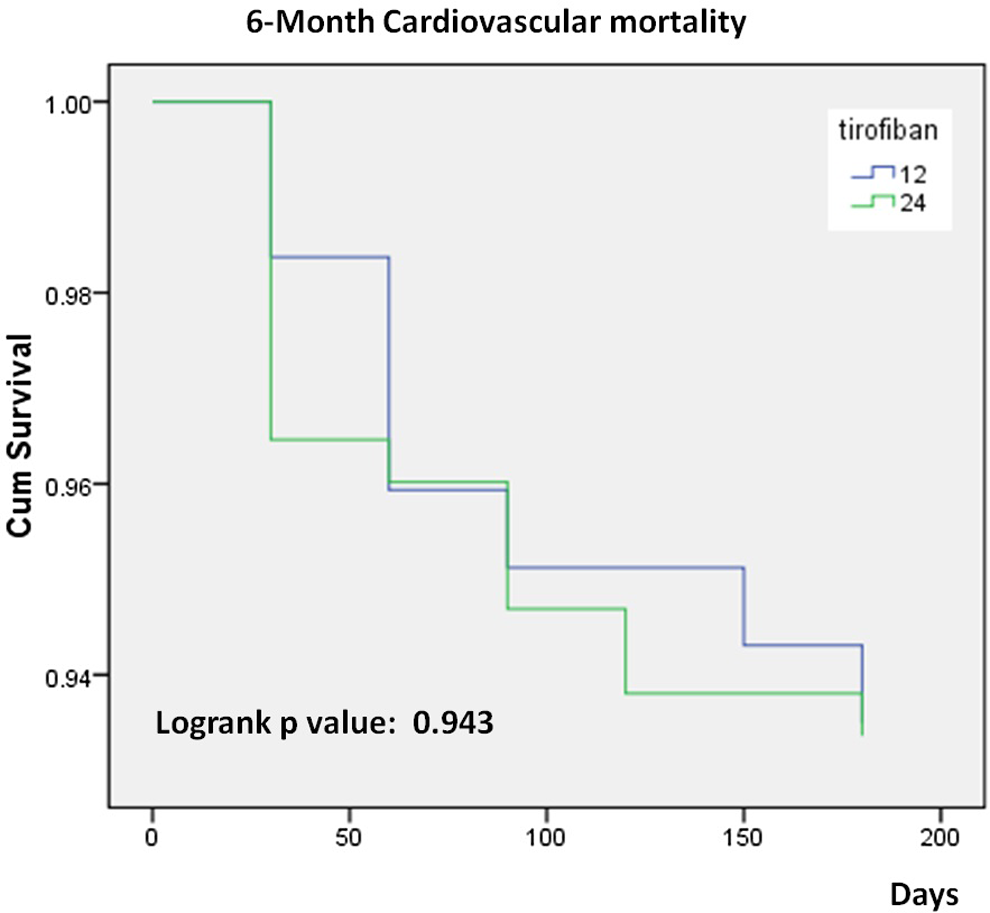
Six-month cardiovascular mortality of study population.
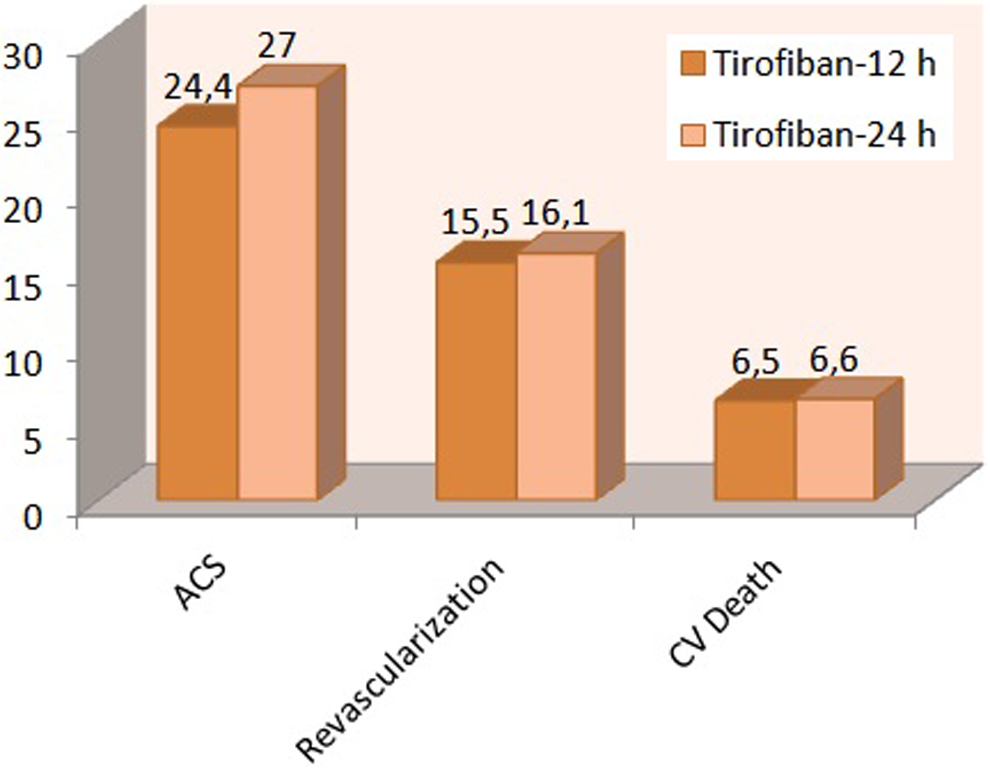
Six-month adverse cardiovascular outcomes of study population.
Discussion
The result of our study revealed that 12-hour tirofiban administration versus 24-hour tirofiban administration in patients with STEMI who underwent primary PCI was similar with respect to (1) in-hospital CV complications such as death, stent thrombosis, and bleeding and (2) CV death, recurrent revascularization, and the incidence of nonfatal acute coronary syndrome and/or stent thrombosis during 6-month follow-up. Glycoprotein IIb/IIIa receptors represent the most abundant protein found on the platelet surface. 12 The platelets become activated as a result of the manifestation of the subendothelial matrix due to endothelial injury. 13 As the platelets become activated, a change occurs in the shape and the structure of the glycoprotein IIb/IIIa receptors. Thus, the receptors become ready to bind to fibrinogen. The activated receptors establish connection with the other platelets and subendothelial matrix through the fibrinogen. 14 Irrespective of the route, the final common route of the platelet activation and aggregation is the binding of fibrinogen to the glycoprotein IIb/IIIa receptor. Glycoprotein IIb/IIIa receptor inhibitors block this final common route, that is, the binding of fibrinogen to glycoprotein IIb/IIIa receptors, thereby providing a strong antiplatelet efficacy in acute coronary syndrome. The most commonly used glycoprotein IIb/IIIa receptor inhibitors include abciximab, eptifibatide, and tirofiban. Tirofiban (2 hours) and eptifibatide (2.5 hours) have a longer plasma half-life compared to abciximab (30 minutes). 15
In-Hospital and 6-Month Efficacy
The benefit of using additional glycoprotein IIb/IIIa receptor inhibitors in patients with STEMI is still controversial. In the European Society of Cardiology (2010) myocardial revascularization guideline, a class IIa recommendation exists for abciximab and eptifibatide, while a class IIb recommendation exists for tirofiban in STEMI among the glycoprotein IIb/IIIa receptor inhibitors. 16 In a meta-analysis covering 11 trials and 12 253 patients, the glycoprotein IIb/IIIa receptor inhibitors in STEMI were found to reduce the 30-day reinfraction by 62%, 30-day repeated PCI by 42%, short-term mortality by 53%, and the long-term mortality by 62%. 17 Similarly, a systematic review analysis involving 10 studies revealed that tirofiban reduced ST-segment resolution and the nonfatal MI risk together with short-term mortality in patients with STEMI. 18 Although tirofiban is being used commonly for different clinical conditions for nearly 10 years, the appropriate dose regimen and protocols have not yet been identified in patients undergoing PCI. 19 However, in a majority of the tirofiban trials, tirofiban was administered for more than 18 hours. In the present study, we compared the short-term (12 hours) tirofiban infusion treatment to the standard dose (24 hours) tirofiban infusion treatment with previously established efficacy for the first time in the literature. We could not find any difference between the 2 treatment modalities in the incidence of CV death and stent thrombosis, which were the indicators of efficacy for the drug, at in-hospital or 6-month follow-up. The most probable reason for the lack of difference between the 2 treatment regimens with regard to efficacy may be the fact that the risk of acute occlusion and thrombotic complications is the highest within the first 12 hours. 20 As known, stent thrombosis and the associated CV deaths mostly occur within the first 24 hours following PCI. 21 It takes 4 to 8 hours for the platelets to restore their normal function after discontinuation of tirofiban. 22 When the 12-hour infusion period is added to this period, the patients remain under the antiplatelet efficacy of tirofiban in the first 12 to 24 hours, which is considered as the risky period following PCI. We propose that the above-mentioned mechanism is the most probable reason for the equivalency between the short- and long-duration infusions.
In-Hospital Safety
Glycoprotein IIb/IIIa receptors belong to a large family of cell-surface receptor glycoproteins called integrin. Fibrinogen binds to this receptor and thus leads to platelet aggregation and coronary thrombosis. 23 In the cases where this receptor is totally deficient (Glanzmann thrombasthenia) or is partially inactive (glycoprotein IIb/IIIa receptor inhibitors), the platelet aggregation decreases and the bleeding risk increases. This interaction between these receptors and the glycoprotein IIb/IIIa receptor inhibitors helps us understand the bleeding complication: as the antiplatelet effect induced by the glycoprotein IIb/IIIa receptor inhibitors increases, the tendency of bleeding may increase; and this paradoxical effect is similar to the antiplatelet efficacy of the P2Y12 inhibitors and the bleeding relation. Many studies reported that the use of glycoprotein IIb/IIIa receptor inhibitors did not induce an increase in the major bleeding risk; however, increased the risk of minor bleeding. 5 –7 The Randomized Efficacy Study of Tirofiban for Outcomes and REstenosis (RESTORE) trial compared tirofiban + heparin combination with heparin and revealed no significant difference between the 2 groups with respect to major bleeding. 24 Similarly, in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) and PRISM in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) trials, no difference was found between tirofiban and heparin with respect to major bleeding. However, in all these trials, tirofiban was generally administered for a period longer than 18 hours. 25,26 In the present study, we did not found any difference between the tirofiban with a standard duration (24 hours) and the tirofiban infusion with a shorter duration with respect to major or minor bleeding.
Limitations
The most important limitation of the present study is its retrospective design. Retrospective studies involve a higher systematic bias relative to the randomized controlled studies. In order to prevent bias, the in-hospital and 6-month data were collected by different investigators. This limits the generalization of the results. In addition, the number of patients is relatively small. Particularly, the low incidence of the end points reached during the in-hospital and 6-month follow-up reduces the power of the statistical analysis.
Conclusion
A 12-hour tirofiban administration has an equivalent in-hospital clinical efficacy and safety relative to 24-hour tirofiban administration. Similarly, the midterm clinical efficacy was also comparable. As a result, we conclude that 12-hour tirofiban administration is as effective and safe as the 24-hour tirofiban administration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.