
Abstract
Aims:
We aimed to investigate the determinants of angiographic thrombus burden in patients with ST-segment elevation myocardial infarction (STEMI) who underwent primary percutaneous coronary intervention (pPCI).
Methods:
The study population consisted of 662 patients with nonanemic STEMI who underwent pPCI. Clinical, laboratory, and demographic properties of the patients were recorded. Baseline hematologic indices were measured at the time of admission. Angiographic coronary thrombus burden was scored based on thrombolysis in myocardial infarction (TIMI) thrombus grades. After wiring and/or small balloon dilation, patients with thrombus burden grades 4 and 5 were defined as high thrombus burden, and patients with thrombus burden <grade 4 was defined as low thrombus burden.
Result:
Patients with high thrombus burden had more family history of coronary artery disease, longer pain to balloon time, higher Killip class (≥II), higher neutrophil to lymphocyte ratio, red cell distribution width (RDW), baseline creatine kinase-MB fraction (CK-MB) and baseline troponin, higher peak CK-MB, and peak troponinbut lower triglycerides. Angiographically, patients with high thrombus burden had longer lesion in the infarct-related artery, less frequent direct stenting, lower epicardial and myocardial perfusion, more frequent distal embolization, and more frequent electrocardiographic and angiographic no reflow. In multivariate logistic regression analysis, only RDW (odds ratio: 1.29, 95% confidence interval 1.19-1.39, P < .001) was determined as independent predictor. The area under the receiver–operating characteristic curve of the RDW was 0.733 (0.690-0.776, P < .001) to predict high TIMI thrombus burden.
Conclusion:
Present study results demonstrated that high thrombus burden in patients with STEMI was associated with impaired postprocedural epicardial and myocardial perfusion and higher no reflow and distal embolization; and increased RDW values were independent predictors of coronary thrombus burden.
Introduction
Intracoronary thrombus management is still challenging, despite recent major pharmacological and invasive improvements, such as glycoprotein IIb/IIIa antagonists or thrombectomy, respectively, in percutaneous coronary intervention (PCI). 1 –3 Intracoronary thrombus burden is still a risk factor for long-term adverse cardiovascular events, stent thrombosis, no reflow, and distal embolization. 4 –7 Establishing the predictors of intracoronary thrombus and associated clinical and angiographic conditions, therefore, may provide improvements in its management. To address this issue, we aimed to investigate the determinants of angiographic thrombus burden in patients with ST-segment elevation myocardial infarction (STEMI) who underwent pPCI.
Methods
Study Population
We retrospectively reviewed 778 consecutive patients who presented with STEMI and who underwent primary PCI (pPCI) at the Ataturk University School of Medicine between January 2010 and September 2012. The inclusion criteria were (1) presentation within the first 12 hours after the onset of pain (18 hours for cardiogenic shock) and (2) presence of an ST-segment elevation at least 1 mm (2 mm for V1-V3) in 2 or more contiguous leads in electrocardiogram (ECG) or new onset of left bundle-branch block. The patients with baseline anemia (<13 g/dL for males, 12 g/dL for females; n = 109) and history of blood transfusion in the last 3 months (n = 7) were excluded. Finally, the study population consisted of 662 patients. Informed consent was obtained from all patients during hospitalization, and the study protocol was approved by the local ethics committee.
Age, sex, history of hypertension, diabetes, hyperlipidemia, smoking status, previous PCI or coronary artery bypass graft (CABG), family history, anthropometric characteristics such as height and weight, and clinical risk factors were recorded for all patients included. Additionally, blood pressure, heart rate, Killip class, presence of cardiogenic shock, previous medications, presence of preinfarction angina, pain to balloon time and door to balloon time, serum creatinine, lipid panel, and hematological indices were measured for all patients during hospital admission. Hemoglobin, white blood cell, neutrophil–lymphocyte (NLR) ratio, red cell distribution width (RDW), mean platelet volume, and platelet counts were measured as part of the automated complete blood count (CBC) using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland).
Clinical and demographic properties of the patients were recorded. Baseline lipid panels, creatine kinase, creatine kinase-MB isoform (CK-MB), and troponin levels were obtained on admission. An estimated glomerular filtration rate (GFR) calculated from serum creatinine using the Cockgroft-Gault equation ([140 − age] × [weight in kg] × [0.85 if female]/[72 × creatinine]). The use of glycoprotein IIb/IIIa receptor blockers (tirofiban) with 10 μg/kg bolus and 0.15 μg/kg/min intravenous infusion was left to the primary operator’s discretion.
All pPCI procedures were performed by experienced interventional cardiologists through a femoral approach. Postprocedural final thrombolysis in myocardial infarction (TIMI) flow grade and TIMI myocardial perfusion grade (TMPG) were assessed. Postprocedural TIMI flow, corrected TIMI frame count (cTFC), and TMPG were noted.
Clinical Definitions
Anemia on admission was defined as a baseline hemoglobin concentration of less than 13 mg/dL in men and less than 12 mg/dL in women, in accordance with the World Health Organization criteria. 8 Hypertension (HTN) was defined as systolic pressure >140 mm Hg and/or a diastolic pressure >90 mm Hg at least 2 times, or if the individual was taking antihypertensive medications. The diagnosis of diabetes mellitus (DM) was based on previous history of DM treated with or without drug therapies. Hypercholesterolemia was defined as total cholesterol ≥200 mg/dL or previous history of statin use. Current smokers were defined as those who had smoked for some period during the past year. Positive family history of coronary artery disease was defined as documented evidence of premature coronary artery disease in a close relative (men <55 and women <65 years of age). Cardiogenic shock was defined as the presence of peripheral hypoperfusion signs (cold shivering, paleness, oliguria, loss of consciousness, etc) accompanied by low-systemic blood pressure (<90 mm Hg) that were resistant to fluid administration and required inotropic therapy and/or intra-aortic balloon pump.
Angiographic Definitions
Angiographic coronary thrombus burden was scored based on 5 grades, as previously described. 5 The classification of thrombus burden is demonstrated in Table 1 in detail. We primarily calculated TIMI thrombus grade based on the initial diagnostic angiogram, then, after restoring antegrade flow through guidewire or small balloon dilatation in patients with TIMI thrombus grade 5; coronary angiogram enabled restratification of the underlying residual thrombus (final TIMI thrombus grade). 5,9,10 We then stratified the final TIMI thrombus grades as low thrombus burden or high thrombus burden, based on scores 1 to 3 or 4 to 5, respectively.
The TIMI Thrombus Burden Classification.a
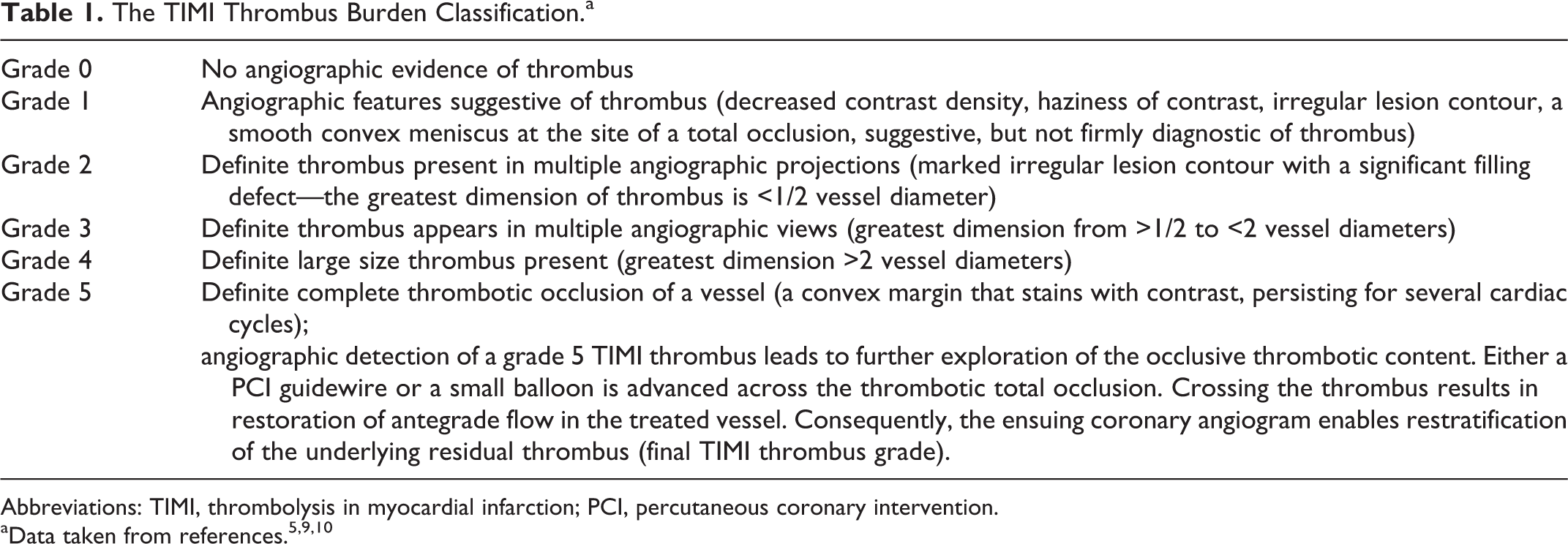
Abbreviations: TIMI, thrombolysis in myocardial infarction; PCI, percutaneous coronary intervention.
In the final diagnostic angiogram, TIMI flow grades, cTFC, and TMPG measurements were assessed as previously described. 11 –13 The TMPG was analyzed by categorizing into 2 groups (TMPG 0, 1 vs TMPG 2, 3). TIMI 0, I, and II were described as angiographic no reflow. The ST resolution (STR) in ECG was assessed based on ST-segment regression percentage on 90th minute ECG. Although 70% and above ST resolution was concluded as successful reperfusion, less than 70% ST resolution on ECG was defined as electrocardiographic no reflow. Distal embolization was defined as a new filling defect with an abrupt cutoff in one or more peripheral coronary branches of the infarct-related artery (IRA) distal to the angioplasty site.
Statistics
Continuous variables are expressed as mean ± standard deviation, whereas categorical variables are expressed as percentage. Comparison between groups was made using the Mann-Whitney U test or chi-square tests, as appropriate. Multiple logistic regression analysis was performed to identify the independent predictors of high thrombus burden using variables showing marginal association with it on univariate testing (P < .10). Receiver–operating characteristic (ROC) curves were plotted to determine the optimal cutoff values for individual parameters in order to predict high TIMI thrombus grade and to establish the optimal cutoff points for use in clinical decision making. Two-tailed P values <.05 were considered to indicate statistical significance. Statistical analysis were performed using SPSS, version 17.0 for Windows
Results
Study population consisted of 662 patients with STEMI (mean age 54.5 ± 11.9 and 87.3% male). The TIMI thrombus grade was calculated from both initial angiogram and finally postwiring or post-small balloon dilatation (Table 2). Eventually, final TIMI thrombus grades of the study population were low thrombus burden in 213 (32%) patients and high-thrombus burden in 449 (68%) patients.
Initial TIMI Thrombus Burden Classification and Final TIMI Thrombus Burden Reclassification.
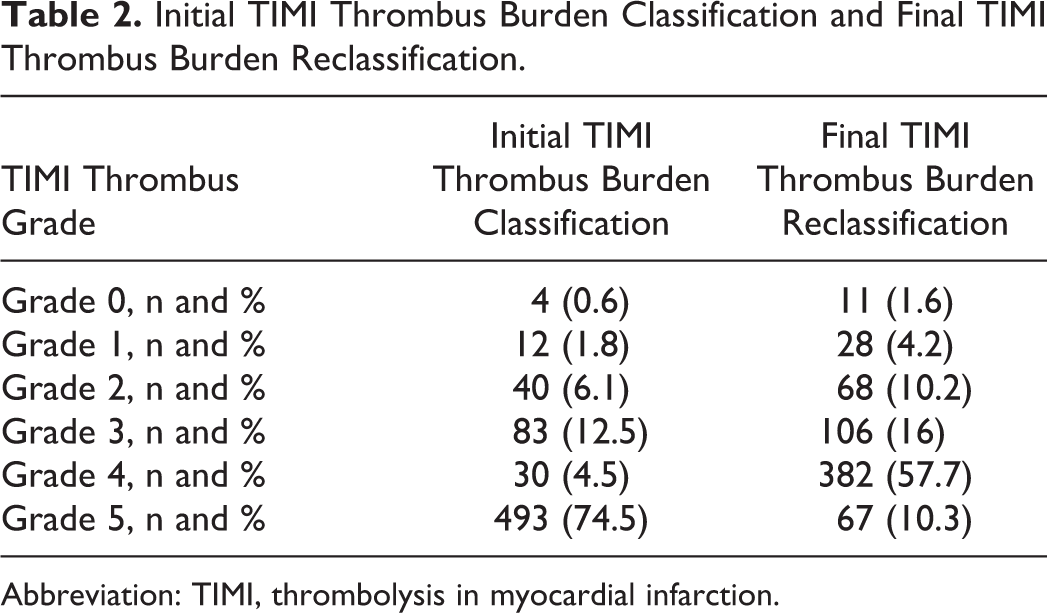
Abbreviation: TIMI, thrombolysis in myocardial infarction.
The comparison of basic clinical and laboratory findings between thrombus burden groups is shown in Table 3. Patients with high-thrombus burden had more family history of coronary artery disease (CAD; 28.1% vs 17.4%, P = .003), longer pain to balloon time (150 [80-237] vs 120 [60-210] vs, P = .002), higher Killip class (≥II; 18.9% vs 11.3%, P = .013), higher NLR (5.6 [3.6-9.1] vs 4.2 [2.8-6.2], P = .001), RDW (17.3 [15.3-19.3] vs 14.5 [12.8-16.5], P < .001; Figure 1), baseline CK-MB (35 [25-48] vs 32 [23-39], P < .001) and baseline troponin (2.34 [0.90-5.43] vs 1.34 [0.60-3.45], P < .001); higher peak CK-MB (188 [116-332] vs 127 [71-216], P < .001), and peak troponin (91 [45-187] vs 47.9 [15.4-120], P < .001); however, lower triglycerides (TGs; 110 [78-155] vs 124 [86-187], P = .014).
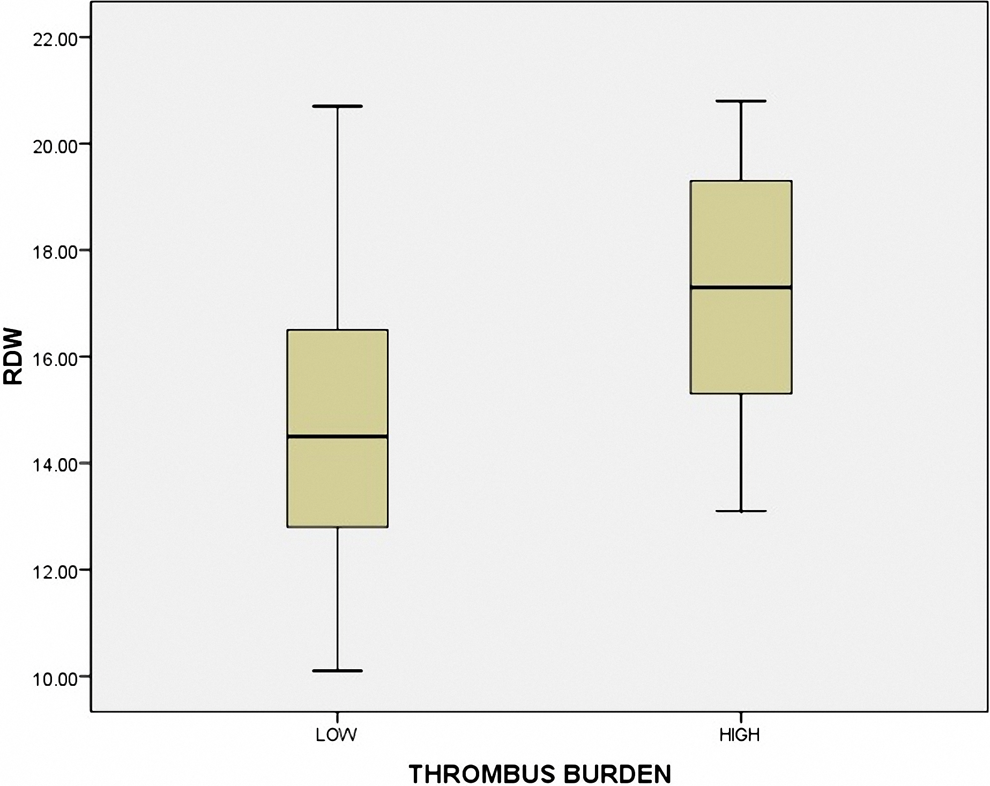
Red blood cell distribution width (RDW) values according to thrombolysis in myocardial infarction (TIMI) thrombus burden.
Baseline Clinical and Laboratory Characteristics According to Thrombus Burden.
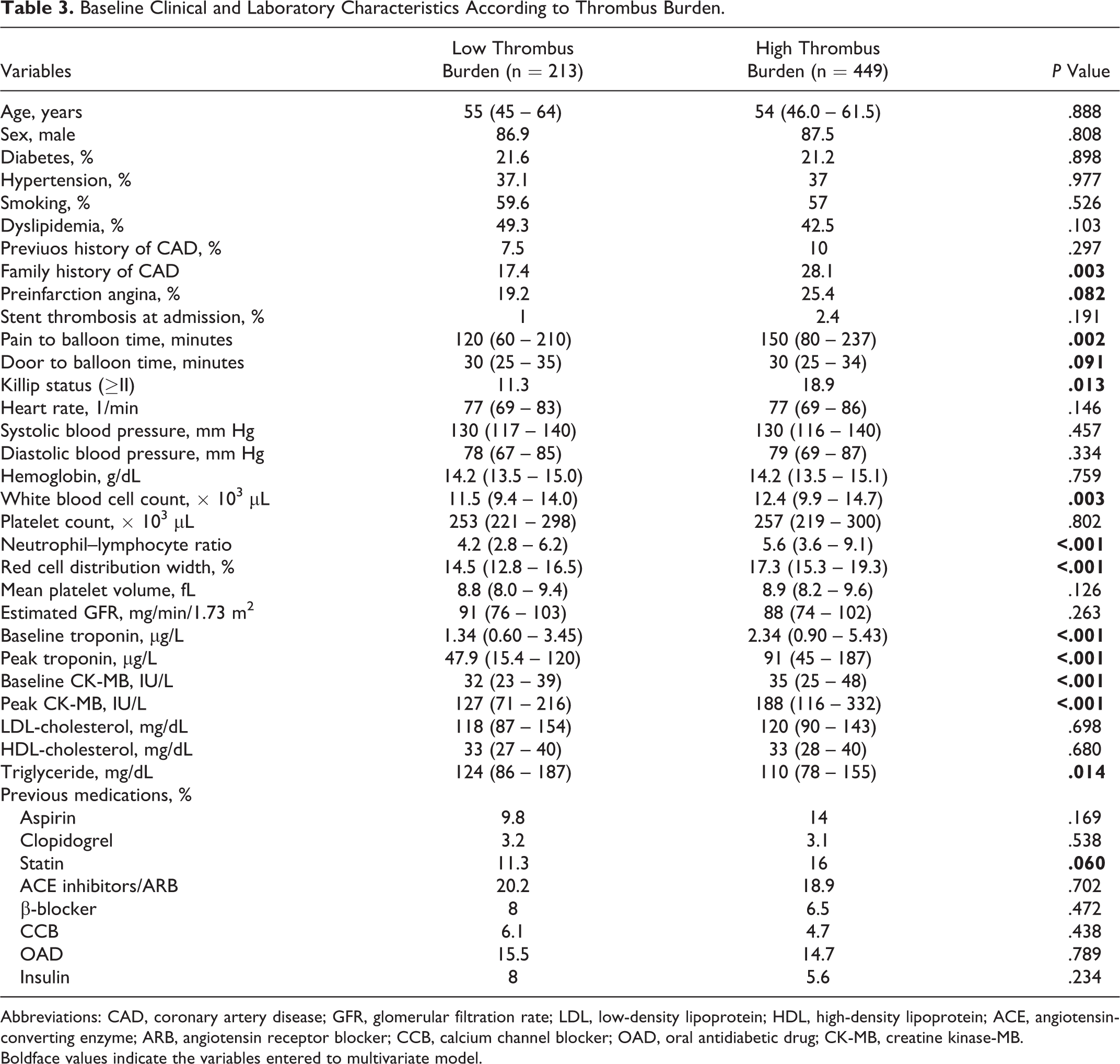
Abbreviations: CAD, coronary artery disease; GFR, glomerular filtration rate; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; OAD, oral antidiabetic drug; CK-MB, creatine kinase-MB.
Boldface values indicate the variables entered to multivariate model.
Comparison of the baseline angiographic characteristics and postprocedural findings of the groups based on thrombus burden is shown in Table 4. Longer lesion in the IRA (14 [12.0-16.6] vs 12.6 [10.1-15.0], P < .001), less frequent direct stenting, lower epicardial (87.5% vs 95.3% for TIMI-flow III, P = .002 and 22 [17-28] vs 20 [15-24] for cTFC, P < .001) and myocardial perfusion (44.1% vs 61.2%, P = .001), more frequent distal embolization (7.3% vs 2.8%, P = .021), more frequent electrocardiographic (41.7% vs 19.4%, P < .001), and angiographic no reflow (12.5% vs 4.7%, P < .001) were observed in patients with high thrombus burden. There were weak inverse correlation between RDW value and cTFC (r = .089, P = .022) and percentage of ST segment resolution (r = −.113, P = .004). As expected, operators have given more tirofiban to the high thrombus burden group (82.2% vs 75%, P = .034).
Baseline Angiographic and Postprocedural Characteristics According to Thrombus Burden.
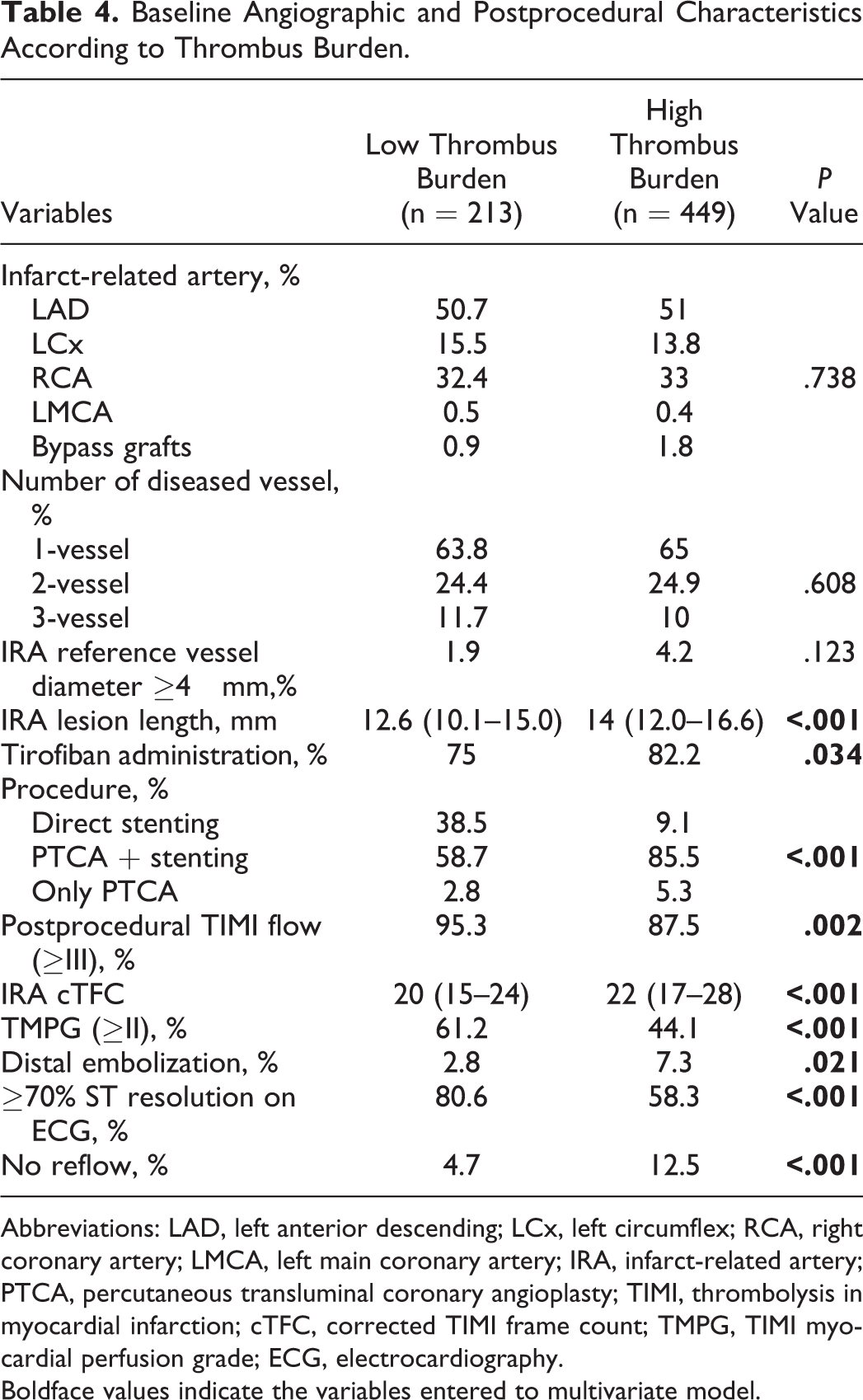
Abbreviations: LAD, left anterior descending; LCx, left circumflex; RCA, right coronary artery; LMCA, left main coronary artery; IRA, infarct-related artery; PTCA, percutaneous transluminal coronary angioplasty; TIMI, thrombolysis in myocardial infarction; cTFC, corrected TIMI frame count; TMPG, TIMI myocardial perfusion grade; ECG, electrocardiography.
Boldface values indicate the variables entered to multivariate model.
Multivariate logistic regression analysis was performed in order to determine independent predictors of high-thrombus burden (family history of CAD, preinfarction angina, previous history of statin use, Killip class, pain to balloon time, door to balloon time, NLR, RDW, TG, baseline CK-MB, and baseline troponin; Table 5). Only RDW (odds ratio = 1.29, 95% confidence interval = 1.19-1.39, P < .001) was determined as an independent predictor in the analysis. The area under the ROC curve of the RDW was 0.733 (0.690-0.776, P < .001) to predict high TIMI thrombus burden. The best cutoff values of the RDW to predict high TIMI thrombus burden was 15.2% (75% sensitivity and of 57% specificity; Figure 2).
Multivariate Logistic Regression Analysis to Detect the Independent Predictors of High TIMI Thrombus Burden.
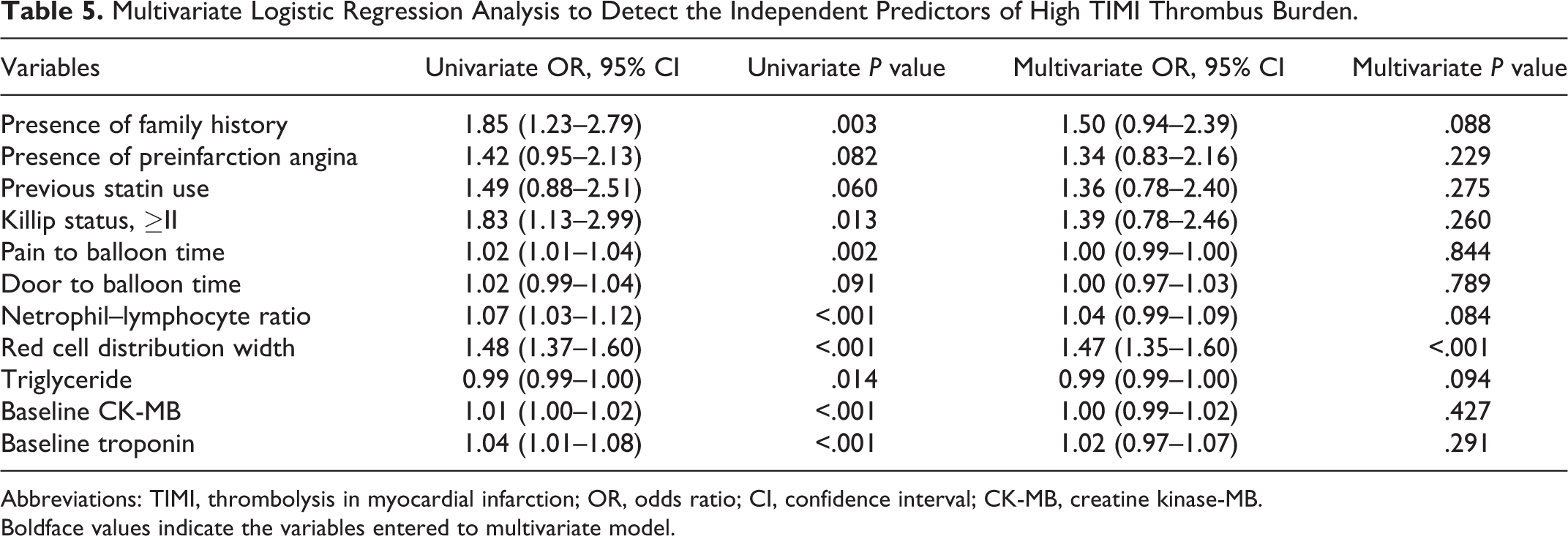
Abbreviations: TIMI, thrombolysis in myocardial infarction; OR, odds ratio; CI, confidence interval; CK-MB, creatine kinase-MB.
Boldface values indicate the variables entered to multivariate model.
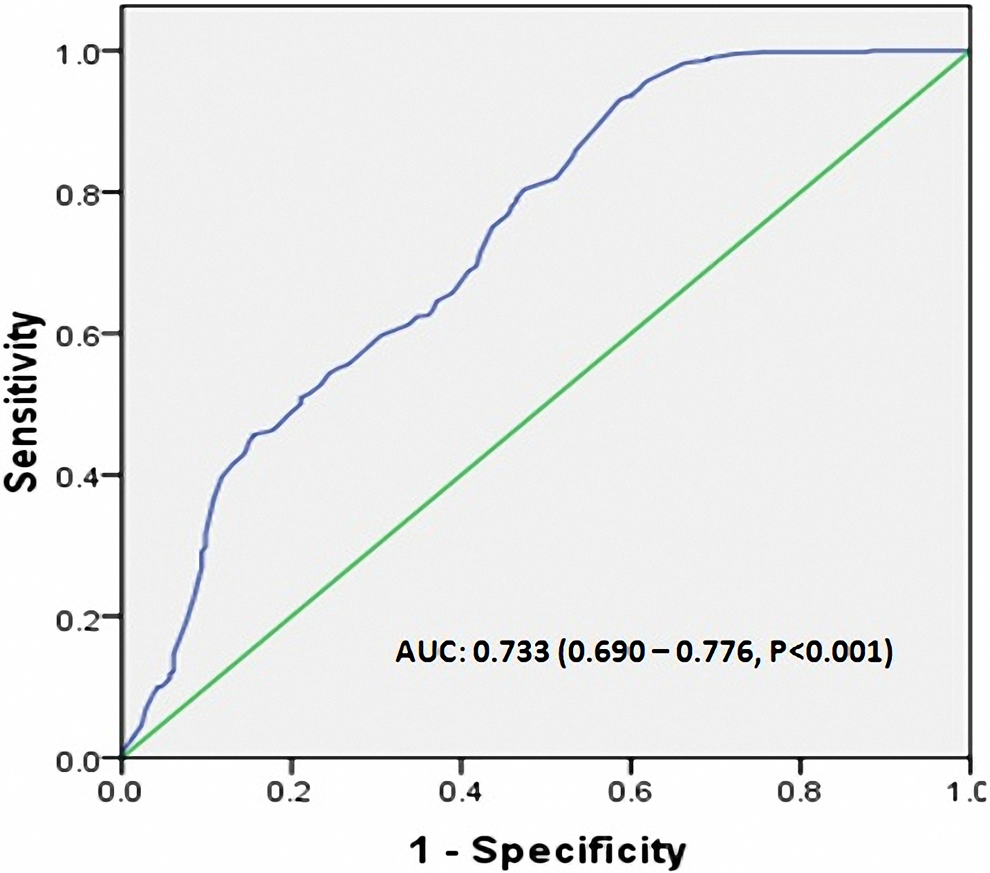
Receiver–operating characteristic curves for red blood cell distribution width (RDW) value for the prediction of high thrombolysis in myocardial infarction (TIMI) thrombus burden.
Two blinded interventional cardiologists (E.A., S.S.) assessed the data of 100 randomly selected patients for the interobserver and intraobserver agreements for final TIMI thrombus burden decision as low or high. The weighted κ value between the 2 observers is 0.66 (0.48-0.83). The data were again assessed by the same interventional cardiologist (S.S.) 2 weeks later and the weighted κ value is 0.83 (0.70-0.96).
Discussion
The present study results showed that RDW was independent predictors of high thrombus burden in patients with STEMI who underwent to pPCI. Furthermore, we found that high thrombus burden is associated with lower postprocedural TIMI flow, cTFC, and TMPG; higher peak CK-MB and troponin; and higher percentage of no reflow and distal embolization.
Intracoronary thrombosis developed after plaque rupture and causing partial or complete occlusion of coronary artery is the basic pathophysiologic event in patients with acute myocardial infarction and unstable angina. 14 Intracoronary thrombus and quantity of the thrombus burden are important determinants of prognosis in STEMI. 4,5,15 Intracoronary thrombus reduces epicardial blood flow depending on partial or complete occlusion. Besides, distal embolization coming from the thrombus mass (spontaneous or during PCI) impairs myocardial perfusion. Therefore, treatments such as glycoprotein IIb/IIIa inhibitors, or procedures such as thrombectomy, which are reducing thrombus burden, improve both epicardial and myocardial perfusion. 16 We aimed to determine predictors of intracoronary thrombus burden and to investigate the clinical and angiographic relations of the thrombus burden in our study. We found RDW as independent predictor of thrombus burden in our study. The RDW is a marker of variation in the size of circulating red cells (anisocytosis) and is routinely reported as a part of routine CBC analysis. The RDW is reported as high in patients with acute coronary syndrome and associated with adverse cardiovascular events in many studies. 17 –20 We determined that RDW is independently associated with intracoronary thrombus burden, for the first time. Association of high intracoronary thrombus burden with impaired postprocedural epicardial and myocardial perfusion was shown both in the present and in the previous studies. The RDW has a similar relation with postprocedural epicardial and myocardial perfusion. Isik et al demonstrated that baseline RDW value in patients who underwent pPCI was closely related to electrocardiographic no reflow. 21 In another study, Karabulut et al showed that increased RDW was associated with postprocedural impaired epicardial perfusion. 22 In conclusion, we believe that increased RDW impairs epicardial and myocardial perfusion by increasing coronary thrombus burden.
Our study has significant clinical implications. Prediction of thrombus burden and possible adverse events related to the thrombus burden in patients with STEMI undergoing pPCI before the intervention and detection of the high-risk patients may contribute to high thrombus burden management through enhancing utilization of pharmacological agents such as glycoprotein IIb/IIIa antagonists or interventional strategies such as mechanical thrombectomy.
Limitation
Since our study was designed retrospectively, it has common limitations of retrospective studies because of the bias depending on nonmeasurable factors. Similarly, since classification of thrombus burden was based on visual evaluation, an agreement analysis was performed, but agreement analyses also have some limitations. 23 Thrombectomy devices were not actively used in our country during the time of our study; therefore, we could not give information about the subject.
Conclusion
The present study results demonstrated that high thrombus burden in patients with STEMI was associated with impaired postprocedural epicardial and myocardial perfusion and higher no reflow and distal embolization; and increased RDW values were independent predictors of coronary thrombus burden.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.