
Abstract
In a cohort of patients with juvenile myocardial infarction, we considered the red cell distribution width (RDW), hematocrit, hemoglobin, and elongation index values at the initial phase and at 3 and 12 months from the acute event. In the initial phase, only the elongation index values turn out reduced if compared with those of the control group, and that only turn out to discriminate the infarcted ST-segment elevation myocardial infarction (STEMI) from non-STEMI. Dividing the patients according to the traditional risk factors and the extent of coronary heart disease, there are no significant variations in the analyzed parameters. No major changes are observed after 12 months from the acute event. Both to 3 and to 12 months from the infarct episode, the negative statistical correlation between RDW and the value of elongation index remains. These data make us reflect on the role of the degree of anisocytosis of red blood cell expressed by the RDW on the determinism of erythrocyte deformability, which plays its role in the microcirculation district and that is essential in the transfer of tissue oxygen.
Keywords
Introduction
As part of the “Sicilian study on juvenile myocardial infarction,” we have reported in recent years about the aspects regarding the hemorheological profile, 1 the metabolic and functional activity of polymorphonuclear leukocytes2,3 and platelets,4,5 the role of genetic polymorphisms, 6 oxidative stress, 7 protein oxidation, 8 the neutrophil/lymphocyte ratio, 9 and plasma viscosity 10 at the initial phase and in the months following the infarct event. However, we have not disregarded neither the behavior of erythrocyte deformability nor the red cell distribution width (RDW), although in part of the entire cohort of these patients, we have previously observed a reduction in erythrocyte deformability, explored with whole blood filtration and diffractometric technique, with respect to the group of healthy volunteers. 11
The erythrocyte deformability is dependent on the surface/volume ratio of the erythrocyte, on internal viscosity related mainly to the concentration of cytosolic calcium, on erythrocyte organic phosphates (ATP and 2.3 DPG), and changes in hemoglobin, and it is also dependent on the dynamic membrane properties, related to the protein and lipid composition. In addition to allowing the erythrocyte to easily cross microvascular districts of a few microns, so much lower than the geometric characteristics of the red blood cell (RBC), the deformability plays a specific role in the supply to oxygen to tissues. 12
So far, in patients with acute myocardial infarction (AMI) not divided for age, many are the reports related to the evaluation of this parameter, whose behavior has been described from time to time but almost never full analyzed.13–18
Similarly, there are many reports regarding the RDW in both coronary heart disease and AMI. As is well known, RDW is a measure of the range of variation of the volume of erythrocytes, in terms of percent coefficient of variation. Two factors influencing the change in erythrocyte volume in physiological terms should be considered when assessing this parameter. The first is the variability of bone marrow production that eliminates cells that are not suitable to be circulated through the reticuloendothelial system (ineffective erythropoiesis). The second is related to the progressive aging of circulating erythrocyte population, which is accompanied by a reduction in cell volume due the dehydration; in short, the causes of the increase in RDW lie in 1 of these 4 possibilities: decreased mean volume, increased reticulocyte volume variance, increased heterogeneity in the rate of RBC volume occurring in the peripheral circulation, and delayed RBC clearance. 19 Interest in RDW has winded over the past 2 decades after various and in-depth research have highlighted the close relationship between the increase in RDW and certain cardiovascular diseases, so as to make it consider a predictive marker of a very wide range of cardiovascular disorders. There are many papers about the behavior of RDW in patients with coronary heart disease20–31 and in AMI patients.32–37
We must consider that in AMI especially at the initial stage, there are all the doctrinal assumptions that both the erythrocyte deformability and the RDW are involved in the opposite way. In fact, in the initial or acute phase of the AMI, the erythrocyte deformability is adversely affected by increased lipid peroxidation than from that of protein oxidation that some of us have observed and described in this cohort of patients with juvenile myocardial infarction,7,8 and the trend of RDW could be associated with the cytokine network that seems to accompany the infarct myocardial event.38–42 The RDW reflects the increase in cytokines such as IL-6 and TNF-alpha. These cytokines together with other inflammatory markers alter erythropoiesis and cause a significant variation in erythrocyte maturation.
In this retrospective study on our cohort of patients with juvenile myocardial infarction, we examined the behavior of the 2 parameters at an early stage, 3 and 12 months after the acute event in relation to the main traditional risk factors (smoking habit, family history of coronary artery disease, hypercholesterolemia, arterial hypertension, and diabetes mellitus) and the extent of coronary heart damage, especially evaluating their possible correlation.
Materials and Methods
Population
In this study, we examined 119 young subjects (aged <46) with recent AMI, from 2001 to 2007. The time interval between the AMI onset and the investigation was 13 ± 7 days. The diagnosis of AMI was carried out on the basis of clinical picture, electrocardiography, blood parameters (creatine kinase, troponin, and myoglobin), and echocardiography, according to ESC/ACC/AHA/WHF gudelines. 43 Subjects were admitted either from the A&E department of our university hospital or were transferred from other hospitals in western Sicily. In each subject, we examined the presence of the main cardiovascular risk factors, including smoking habits, family history of CAD, hypercholesterolemia, arterial hypertension, and diabetes mellitus. Family history consisted of any first-grade relative with clinical manifestation of coronary artery disease at age <55 years. Hypercholesterolemia was defined as a total cholesterol level >220 mg/dL and/or use of lipid-lowering drugs. Diabetes mellitus was defined as a fasting blood glucose level >126 mg/dL and/or the use of hypoglycemic drugs. Arterial hypertension was defined as a systolic blood pressure >140 mm Hg and/or a diastolic blood pressure >90 mmHg and/or the use of antihypertensive drugs. According to the number of cardiovascular risk factors, the young AMI subjects were subdivided into 3 subgroups: 38 of them had 0 to 1 risk factor, 41 had 2 risk factors, and 40 had 3 to 5 risk factors. Coronary angiography was performed only in 101 subjects. In the other cases, the subjects declined their consent or the angiographic evaluation was not carried out because of the long distance between the hospital in which the AMI was diagnosed and the angiographic unit of the university center. The 101 subjects in which coronary angiography was performed were subdivided into 3 groups on the basis of the extent of coronary lesions: 21 subjects did not have any significant coronary lesions, 47 had a single-vessel disease (defined as a stenosis >70% in 1 coronary artery), and 33 had a multivessel disease, which is a stenosis >70% in at least 2 coronary vessels. A revascularization procedure was performed with PCI in 57 patients and with CABG in 8.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Hospital of Palermo. Informed consent was obtained from all subjects involved in the study.
Methods
In this retrospective study, we evaluated the following parameters: RDW expressed as a percentage and evaluated with the automated blood count; hematocrit (Ht) obtained using an automated hematology analyzer; hemoglobin, expressed in grams per liter and evaluated with the automated blood count; and erythrocyte deformability: to evaluate this hemorheological parameter, a 30 µL of anticoagulated blood with 2 mL of dextran solution at a viscosity of 24 mPa was mixed. The measurement was obtained by using the diffractometer Rheodyn SSD of Myrenne, which measures the diffraction pattern of a laser beam passing through erythrocytes suspended in a viscous medium and deformed by a force with defined shear stress. The shear stress employed was 30 and 60 Pa. The erythrocyte deformation was expressed as elongation index (EI) = (l − w/l + w) × 100, where l = length and w = width of the erythrocytes.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism version 9.5. The data were expressed as means and standard deviation. The comparison between the means was effected using the Student t test for unpaired data. The comparison between the different subgroups of juvenile AMI according to the traditional cardiovascular risk factors and to the extent of the coronary damage was made employing the 1-way analysis of variance (ANOVA) integrated by the Tukey’s test. The comparison between each parameter between initial stage (T1), 3 months (T2), and 12 months (T3) was made using the ANOVA for repeated measures. For the analysis of the different correlations, the Pearson’s test was employed. The null hypothesis was evaluated for values of P ≤ .05.
Results
Preliminary, at the initial phase of this cohort of patients with juvenile AMI, we evaluated means, standard deviation, and range of all parameters considered (Table 1). Immediately afterwards, we compared the behavior of the same parameters in the subgroup of ST-segment elevation myocardial infarction (STEMI) infarcts with that of NSTEMI infarcts. From this comparison, it turns out that in the STEMI subgroup, a reduction in the erythrocyte deformability is evident as EI at 30 and 60 Pa (data not shown).
Means ± SD and Ranges of the Erythrocyte Parameters in AMI Patients at T1.

Abbreviations: SD, standard deviation; AMI, acute myocardial infarction; T1, see text; RDW, red blood cell distribution width; Ht, hematocrit; Hb, hemoglobin; EI 30, elongation index at the shear stress of 30 Pa; EI 60, elongation index at the shear stress of 60 Pa.
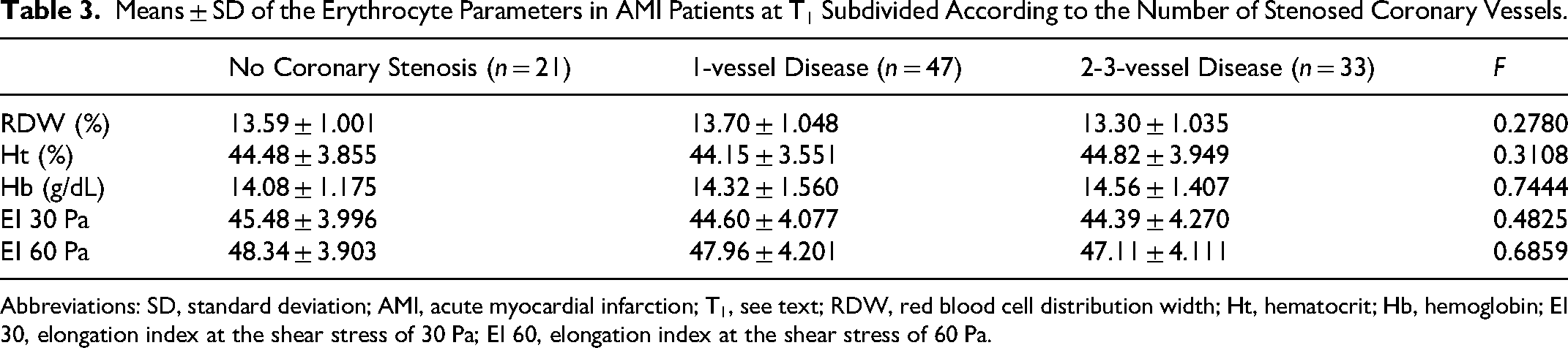
We then divided, always in the initial phase (T1), the entire cohort into 3 subgroups according to the number of traditional cardiovascular risk factors, observing with the use of the ANOVA, that neither the RDW erythrocyte index nor the erythrocyte deformability, nor the remaining parameters were affected by risk factors (Table 2). The result was similar when, still at an early stage, the entire cohort was divided into 3 subgroups according to the extent of coronary heart damage. Even with this further subdivision, none of the parameter considered seems to have a discriminating role (Table 3). At the initial phase, however, of particular interest is the negative correlation between the RDW erythrocyte index and the EI, both at shear stress of 30 and 60 Pa (Table 4). We then examined the trend of each parameter at 3 and 12 months after the event. The study, this time, concerned only 52 patients who had adhered to the indications formulated at the time of hospital discharge. This evaluation, carried out with the ANOVA for repeated measurements, has shown that among the parameters under examination, only the Ht tends to increase from the initial phase up to 12 months after the infarct event (Table 5). Once again, data relating to the study of correlations between RDW and the remaining parameters are of particular interest both at 3 months (T2) and at 12 months (T3) from the acute event. In fact, both in T2 and T3, there is a negative correlation between RDW and the values of the EI (data not shown).
Means ± SD of the Erythrocyte Parameters in AMI Patients at T1 Subdivided According to the Number of RFs.

Abbreviations: SD, standard deviation; AMI, acute myocardial infarction; T1, see text; RFs, risk factors; RDW, red blood cell distribution width; Ht, hematocrit; Hb, hemoglobin; EI 30, elongation index at the shear stress of 30 Pa; EI 60, elongation index at the shear stress of 60 Pa.
Means ± SD of the Erythrocyte Parameters in AMI Patients at T1 Subdivided According to the Number of Stenosed Coronary Vessels.
Abbreviations: SD, standard deviation; AMI, acute myocardial infarction; T1, see text; RDW, red blood cell distribution width; Ht, hematocrit; Hb, hemoglobin; EI 30, elongation index at the shear stress of 30 Pa; EI 60, elongation index at the shear stress of 60 Pa.
Correlations Between RDW and the Other Erythrocyte Parameters in AMI Patients at T1.

Abbreviations: AMI, acute myocardial infarction; T1, see text; RDW, red blood cell distribution width; Ht, hematocrit; Hb, hemoglobin; EI 30, elongation index at the shear stress of 30 Pa; EI 60, elongation index at the shear stress of 60 Pa.
Means ± SD of the Erythrocyte Parameters in AMI Patients Who Completed the Follow-Up (n = 52).

Abbreviations: SD, standard deviation; AMI, acute myocardial infarction; T1, T2, T3, see text; RDW, red blood cell distribution width; Ht, hematocrit; Hb, hemoglobin; EI 30, elongation index at the shear stress of 30 Pa; EI 60, elongation index at the shear stress of 60 Pa.
*P < .05 versus T1 (Tukey's test)
**P < .05 (repeated measurements ANOVA)
Discussion
The simultaneous evaluation of RDW and erythrocyte deformability, the latter examined with diffractometric technique, in the cohort of patients with juvenile AMI adds some interesting data to what is already known in this clinical condition.
As is known, the juvenile AMI is between 2% and 10% of all cases of heart attack. Traditional, modifiable, and non-modifiable risk factors must be supplemented by nontraditional risk factors (polycystic ovary, hypoestrogenemia, autoimmune diseases, and inflammatory genetic substrates) and above all the genetic polymorphisms that seem to characterize the cohort of infarcts that are part of the “Sicilian study on juvenile myocardial infarction.” About two-thirds of young patients are non-STEMI, but the clinical presentation is not distinguishable from that of older patients. Patients with juvenile AMI have less frequent angina symptoms. 44 In the same patients, it should instead be evaluated the recent use of abuse substances (cocaine and methamphetamine) and, at the same time, always deepen the family history for arterial and venous thrombotic diseases. From 3% to 11% of such young patients may already present with ventricular arrhythmias or sudden cardiac death when the juvenile AMI is traceable to coronary dissection. 45 As for the clinical picture, however, young patients benefit from revascularization and treatment of complications. In the juvenile population, there is often no coronary artery disease or at most only 1 coronary vessel is affected by narrowing; the disease of the 3 vessels is very infrequent. As a result, reperfusion with PCI is more frequent than with CABG and this has a favorable influence on prognosis. In the patients, there is a lower incidence of early or late complications such as cardiac insufficiency, angina, reinfarct, and atrioventricular block. However, it should be stressed as on the prognosis, also in juvenile AMI, may burden a 23% change of developing new cardiovascular events in the 5-year follow-up" with "In relation to the prognosis, also in juvenile AMI, it could a 23% of possibility of developing new cardiovascular events in the 5-year follow-up. 46
The preliminary data that emerges from this retrospective study is that the EI, explored to shear stress of 30 and 60 Pa, at the initial phase is reduced in juvenile AMI when compared to the values of the control group (P < .05), whereas RDW does not discriminate the 2 groups against the cohort of AMIs subject to the control group. Of particular hemorheological interest is the fact that in the group of infarcted STEMI, EI values are reduced when compared with those found in the non-STEMI group; the RDW does not appear to be discriminating between the 2 subgroups. As previously observed for other parameters of the hemorheological profile, the EI values do not change as the number of cardiovascular factors changes. The same trend was observed for RDW, although there are many reports of its increase in smoking, 47 arterial hypertension,48–50 lipid profile, 51 metabolic syndrome,52,53 and diabetic disease.54,55 With regard to the latter, some authors believe that RDW is an indicator of complications associated with it56–59 and that it even manages to predict 60 plasma glucose level at 2 h from the start of an oral glucose load curve. As the coronary artery damage strain observed in the course of the coronary artery investigation, as previously verified for other hemorheological determinants, there was no change in the EI values at either 30 or 60 shear stress. Similar is the behavior noted for the RDW that, in fact, does not appear to vary in the 3 considered subgroups. These last data however do not seem to align with what was described by other authors,61,62 which have shown an increase in RDW with varying severity and complexity of coronary heart disease and also the number of coronaries involved. By other authors, it is reiterated, through a follow-up carried out up to 3 years after the acute event, that in infarcted patients, not subdivided by age, the increase in RDW appears to be a marker of adverse clinical events and cardiovascular, both intra-hospital and long-term mortality.63,64
Data of particular doctrinal interest is what is recorded when the correlation between the RDW and EI values at 30 and 60 shear stress has been evaluated. In the entire cohort of patients with juvenile AMI, the negative correlation between these 2 parameters is evident. From the point of view of clinical hemorheology, it makes seriously reflect in how much it is not to exclude that in the determinism of the deformability of the RBCs must be taken in due consideration the degree of anisocytosis that of fact is that which is expressed by RDW. Until now, the data obtained in relation to the study of correlation between these 2 parameters have not converged in the literature. The first response concerned a cohort of 293 adults with an average age of 71.1 ± 13.3 participating in a longitudinal aging study in which a significant negative correlation was found between the RDW and the EI evaluated at shear stress of 3 Pa. 65 This correlation became significantly more marked when the entire cohort excluded the group of anemic subjects. Other authors instead both in hypertensive patients, 66 and in patients with AMI 67 both in subjects with metabolic diseases 68 showed a positive correlation between these 2 parameters. Similar to what Patel found, a negative correlation between RDW and EI occurred both in subjects with thalassemic trait and in patients with hematological neoplasms. 69
The behavior of the EI values, RDW, and the remaining parameters in the following months (T2 and T3) from the acute event does not seem to undergo significant changes. What happens to EI values does not surprise us since in all our previous reports 70 concerning the hemorheological profile related to the entire cohort of patients with juvenile AMI, the variations regarding blood viscosity, plasma, and serum viscosity and whole blood filtration were never detected not only at 3 months (T2) but also at 12 months (T3) from the acute event, and this is in agreement with what is now observed and seems to reiterate the peculiarity of the patients who are part of the Sicilian study on juvenile AMI that seem to be characterized by the high percentage of proinflammatory genetic polymorphisms.
The last consideration that concerns the data of this study is regarding what happens several months after the infarct event relative to the persistent negative correlation between RDW and EI values. So not only in the initial phase but also after 3 and 12 months, when you have certainly changed both the cytokine network that partly lipid peroxidation and protein oxidation, which confirms the interdependence related to these 2 parameters.
Conclusions
The data obtained in this report regarding the cohort of patients enrolled in this Sicilian study on juvenile AMI show that only the erythrocyte deformability expressed as EI to shear stress of 30 and 60 Pa is reduced at the initial phase, when compared to that of the control group, and that only this determinant is able to distinguish between STEMI and non-STEMI infarctions, with a negative correlation with the RDW. Erythrocyte deformability, as already established for other hemorheological determinants, does not seem to change with the passing of months and, even after 3 and 12 months from the acute event, correlates significantly with RDW.
As a limitation, this is a retrospective analysis, but this does not reduce the value of the obtained data.
Footnotes
Author Contributions
GC conceptualized the study, analyzed and interpreted the data, and wrote the original draft; MC performed writing—review and editing; RLP performed statistical analysis; MM performed laboratory testing; EC visualized the study. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.