
Abstract
Background:
There is no information about a possible association of red blood cell distribution width (RDW) with cryptogenic stroke (CS). We aimed to analyze the association of RDW with CS.
Patients and Methods:
One hundred and sixty-three patients with CS were included along with 186 healthy controls. Fibrinogen, leukocytes, hemoglobin, and erythrocyte indices were evaluated.
Results:
Patients showed higher RDW, leukocyte count, and body mass index (BMI) than controls (P < .05). No differences were observed in the erythrocyte indices or in glucose, cholesterol, and triglycerides levels (P > .05). When patients with anemia were excluded from the study (6 controls and 5 cases), the differences between cases and controls persisted (P = .005). Multivariate logistic regression revealed that, after adjusting for potential confounders (anemia, age > 40 years, gender, and fibrinogen >382 mg/dL, total cholesterol >240 mg/dL, and BMI > 28.7 kg/m2), RDW >14% was the only parameter that independently increased the risk of CS.
Conclusion:
The RDW >14% increased the risk of CS by 2.5-fold, irrespectively of anemia, inflammation, and lipidic profile.
Keywords
Introduction
Ischemic strokes may be due to large artery atherosclerosis, small vessel occlusion, cardioembolism, and other less common mechanisms such as hypercoagulability and vasospasm. Strokes with no identifiable cause despite a complete work-up are described as cryptogenic, 1 which is therefore a diagnosis of exclusion. Red blood cell distribution width (RDW), a parameter of routine blood cell counts that reflects size variations in erythrocytes and indicates the degree of anisocytosis of red blood cells, has been shown to be a marker of cardiovascular events that are both atherotrombotic 2 –7 and thromboembolic. 7 –11 In patients with ischemic stroke, the association with RDW has been evaluated in 4 studies 12 –15 with conflicting results; Ani and Ovbiagele 12 found that elevated RDW predicts both cardiovascular and all-cause death in patients with stroke, and Kim et al 13 observed RDW to be independently associated with poor functional outcome and all-cause death in patients with stroke after 1 year from onset. However, Ntaios et al 14 reported that RDW does not predict severity or functional outcome in patients with ischemic stroke. In the above-mentioned studies, neither the mechanism of increased RDW in these patients nor its possible role as a marker of adverse outcomes was established. It is important to take into account that in most of the above-mentioned studies, 12,13 RDW was determined in the acute reactant phase. This fact may influence RDW values via inflammation.
It has been suggested that RDW may be associated with lipidic alterations, 13 inflammatory markers, 16 and anemia. 17 However, it is necessary to highlight that the erythrocyte indices, that is, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC), have been reported in none of these studies. These indices are of paramount importance and are, therefore, a limitation of some studies. 14 Cryptogenic stroke (CS) accounts for almost a quarter of ischemic strokes, 18 –20 despite modern diagnostic evaluations, and it usually affects younger people 21 in whom the prevalence of conventional cardiovascular risk factors is low. Therefore, in this type of stroke, neither age nor cardiovascular risk factors should have an influence on RDW values. To date, there are no studies available on RDW in patients with CS. The aim of the present study was to analyze the association of RDW with CS and the hematological, biochemical, and inflammatory parameters related to RDW.
Materials and Methods
Patients and Controls
We conducted a case–control study of CS among consecutive patients from the Neurology Service at the La Fe University Hospital, Valencia (Spain) who were sent to our unit for a thrombophilia work-up from 2004 to 2011. One hundred and sixty-three patients (81 males and 82 females), with a first-ever ischemic stroke of undetermined etiology due to a negative work-up, were considered to be CS according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria 22 and entered the study. In short, the CS criterion is met when no cause for the stroke is found despite an extensive evaluation, including neuroimaging of the brain (computed tomography scan and/or magnetic resonance [MR] imaging), vascular imaging (angiography, colour duplex sonography, or MR angiography), electrocardiogram, and transesophageal echocardiography. The time elapsed between CS and sampling was 233 ± 178 days (range: 67-535). Exclusion criteria were malignancy, hepatic, renal, infectious, or autoimmune disease, as well as having received a blood transfusion in the previous 3 months. The control group consisted of 186 healthy participants (90 males and 96 females) belonging to the staff of our hospital who underwent a routine blood analysis.
Controls and patients were from the same geographical area (eastern Spain) and were all caucasians, and sampling and analytical tests were performed at the same time. Informed consent was obtained from all the participants, and the ethic committee of our hospital approved the study.
Given the influence of anemia on RDW, the hemoglobin levels lower than 13 g/dL for males and 12 g/dL for women were considered to determine the anemic status of all the patients in accordance with the World Health Organization. 17 Patients were considered to have a cardiovascular risk factor if they were obese (body mass index [BMI] ≥30 kg/m2), smokers (≥1 cigarette/d), or if they had hypertension (systolic blood pressure ≥ 130 mm Hg and diastolic blood pressure ≥ 85 mm Hg), hyperlipidemia (total cholesterol ≥ 220 mg/dL or triglycerides ≥175 mg/dL), fasting glucose concentration ≥126 mg/dL, or receiving pharmacological treatment for hypertension, hyperlipidemia, or diabetes.
Laboratory Methods
Venous blood samples were obtained by sterile antecubital venipuncture after overnight fasting for 12 hours, between 8
Leukocyte count, red blood cell count, hemoglobin concentration, hematocrit, and erythrocyte indices, that is, MCV, MCH, MCHC, and RDW, were determined in a Sysmex XE-2100 (Roche Diagnostics S.L., Barcelona, Spain). Fibrinogen was evaluated in an ACL-TOP autoanalyzer (Instrumentation Laboratory, Milan, Italy). Total cholesterol, triglycerides, and glucose were determined by enzymatic techniques, and creatinine and iron by a colorimetric technique in an Olympus AU 5430 autoanalyzer (Beck Coulter España S.A., Madrid, Spain).
Statistical Analysis
All the continuous variables were checked for normal distribution with the Kolmogorov-Smirnov test. Glucose and triglycerides were log-transformed to improve normality for statistical testing. The chi-square test was used to compare differences in percentages in the dichotomic variables.
A Student t test was employed to compare differences in the continuous variables between the 2 groups. Pearson correlation coefficients were calculated to describe the crude association between variables. Finally, a logistic regression analysis was applied to estimate the unadjusted and multivariate adjusted odds ratios and the 95% confidence intervals for RDW >14%, leukocytes >8 × 103/µL, neutrophils >4.8 × 103/µL, fibrinogen >382 mg/dL, and anemia. These cutoff points were calculated from the normal values of the control group, plus 1 standard deviation (SD). Data are expressed as means ± SD. For statistical inference, a bilateral P value of <.05 was considered statistically significant. All the analyses were calculated using the SPSS (SPSS, version 11) for Windows.
Results
Table 1 shows the mean value and SD of biochemical, hematological, and inflammatory parameters in patients with CS and controls. Patients showed statistically higher BMI, RDW, leukocytes and neutrophils counts, and lower total cholesterol than the controls (P < .05). No differences in other parameters analyzed were observed. Seventeen controls (9.1%) and 36 cases (22.1%) showed RDW >14%, P = .001. When patients with anemia (6 controls and 5 cases) were excluded from the study, results did not change (data not shown). When patients and controls were considered separately, women showed statistically higher RDW than men for both cases (13.81 ± 1.4 vs 13.41 ± 0.99, P = 0.044) and controls (13.43 ± 0.70 vs 13.07 ± 0.56, P < .001).
Biochemical, Hematological, and Inflammatory Parameters in Cryptogenic Stroke and Controls.
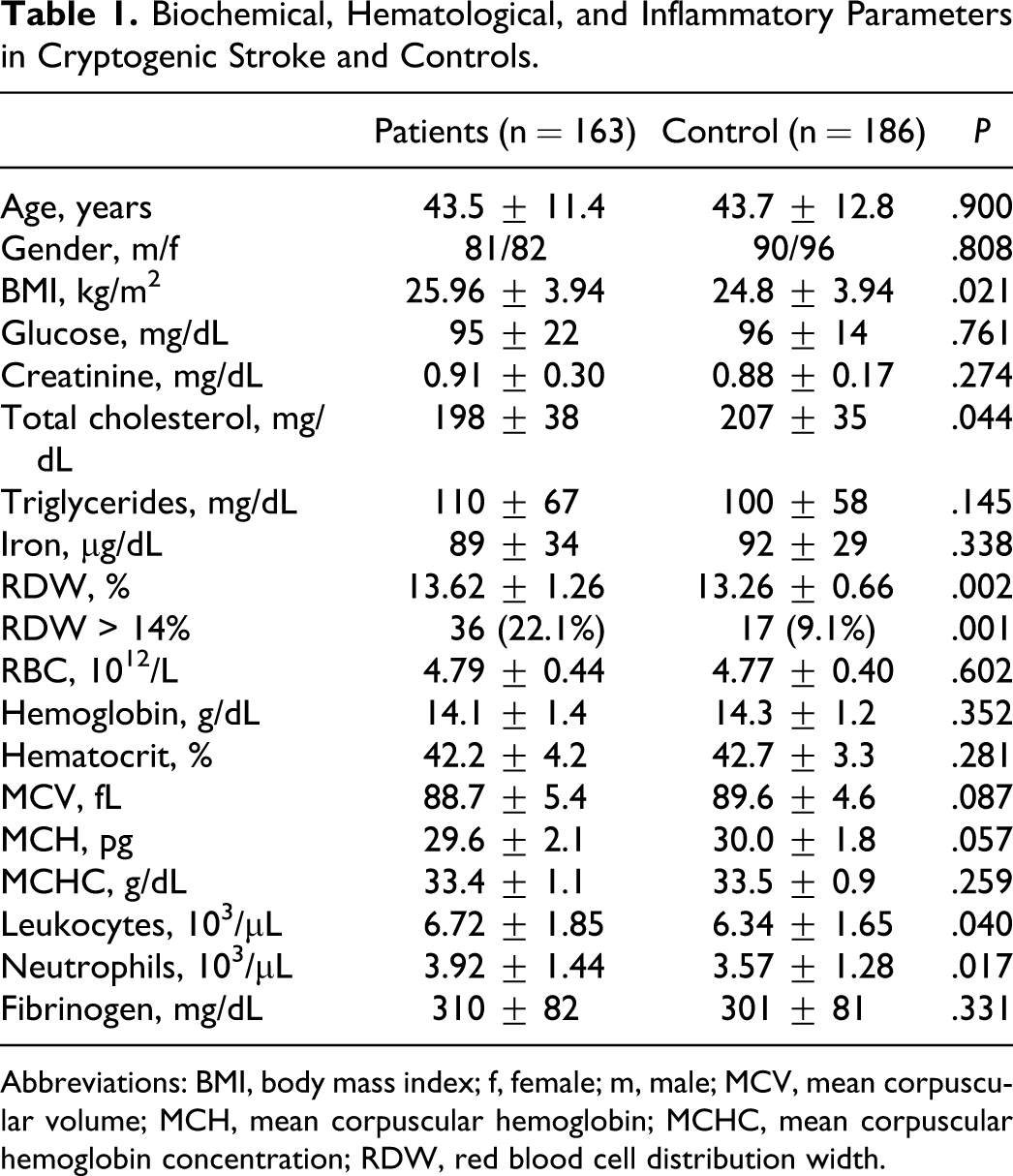
Abbreviations: BMI, body mass index; f, female; m, male; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; RDW, red blood cell distribution width.
Obesity was more prevalent in cases (16%) than in controls (8%), P = .044. No differences in the prevalence of the other cardiovascular risk factors were observed: smokers (cases 36% vs controls 30%; P = .246), hypertension (19% vs 14%; P = .236), hyperlipidemia (22.6% vs 17%; P = .227), and diabetes (6% vs 4%; P = .578).
When only cases were considered, the Pearson bivariate correlation showed that RDW correlated inversely with hemoglobin (r = −.299), Fe (r = −.302), MCV (r = −.424), MCH (r = −.550), and MCHC (r = −.474); P < .01 in all cases. No other statistical correlations were found significant.
In the unadjusted logistic regression (Table 2), both RDW >14% and leukocytes >8.0 × 103/µL increased the risk of CS. After adjusting for potential confounders, such as total cholesterol >240 mg/dL, BMI >28.7 kg/m2, age, gender, anemia, and fibrinogen >382 mg/dL, RDW >14% was the only parameter that independently increased the risk of CS 2.5 times.
Predictors for Cryptogenic Stroke.
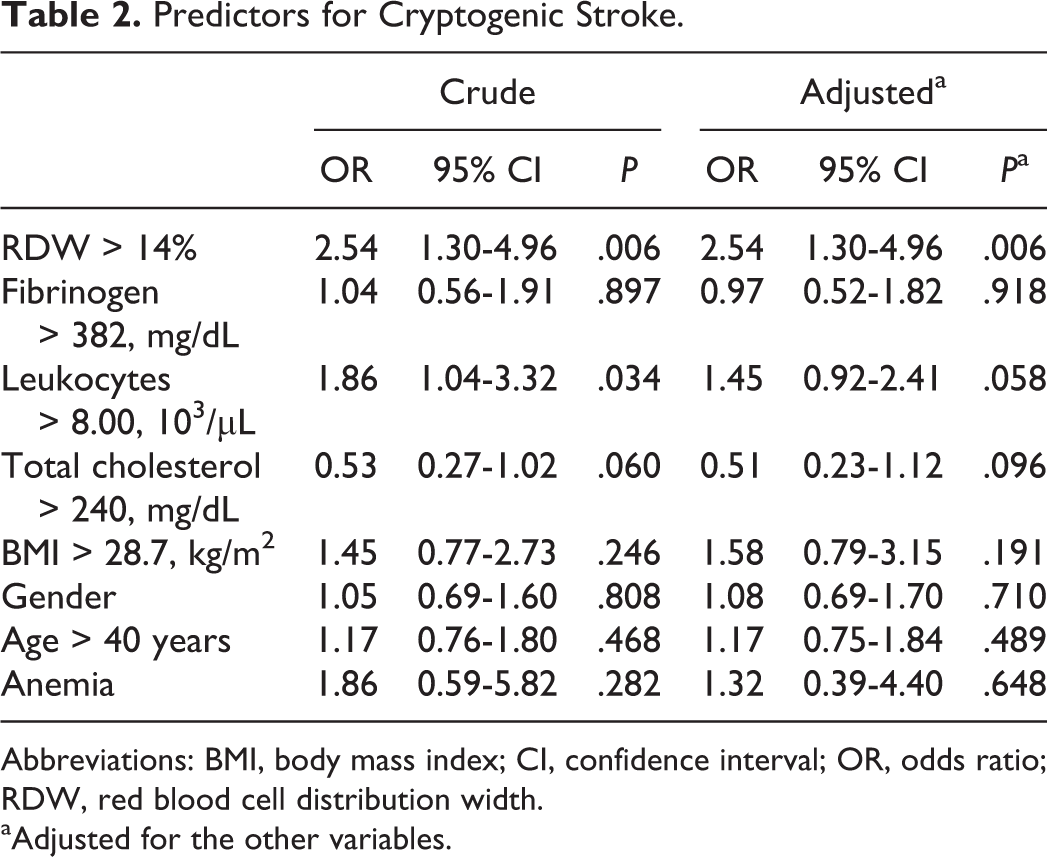
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; RDW, red blood cell distribution width.
aAdjusted for the other variables.
Discussion
The results of the present study indicate that RDW is higher in patients with CS than in the controls. Studies to analyze the association of RDW with ischemic stroke have been carried out only in patients with non-CS. 12 –15 In their study, Ani and Ovbiagele 12 included patients with both hemorrhagic and ischemic stroke and found that elevated RDW predicts both cardiovascular and all-cause death, which is in line with another study by Kim et al, 13 who observed RDW to be independently associated with poor functional outcome and all-cause death after 1 year from onset. Nevertheless, in a study conducted with a cohort of 1500 patients, Ntaios et al 14 found that RDW did not predict severity or functional outcome in patients with acute ischemic stroke, but that serum creatinine, hemoglobin, age, low ejection fraction, and antihypertensive treatment were the main determinants of RDW. It is important to highlight that in the 4 previously cited studies dealing with RDW and stroke, 12 –15 data are lacking on other possible determinants of RDW, like erythrocyte indices, that is, MCV, MCH, and MCHC, which are highly related to it. In fact, RDW is calculated by dividing the SD of the RBC volume by MCV. 23
In the present study, we aimed to evaluate in patients with CS who are not in the acute reactant phase, to avoid its influence on the RDW values, whether there are differences in RDW between patients and controls, what these differences, if any, can be attributed to, and whether RDW constitutes, or not, an independent risk factor for CS. In this sense, our results indicate that RDW is higher in cases than in controls. Given the influence of anemia on RDW, we removed patients with anemia from the study and the differences in RDW remained significant. In addition, we observed that RDW correlated inversely with erythrocyte indices (MCV, MCH, and MCHC) when only patients were considered, which indicates the influence of such indices on erythrocyte anisocytosis. We did not find a correlation between RDW and the several inflammatory parameters analyzed, such as fibrinogen, leukocyte, and neutrophil counts. Similarly, no differences were observed in their mean comparison, except for leukocytes. However, other authors have reported that RDW is associated with inflammatory parameters, such as C-reactive protein, in a large cohort of unselected outpatients, 16 although this has not been confirmed in other clinical settings. 24
Our study was carried out in patients with CS, and as expected, the mean age was around 40 years, which is lower than in the other aforementioned studies on non-CS stroke; that is, 72 ± 15 years 14 and 65 ± 12 years. 13 In line with this, our patients with CS did not show differences in the lipid profile when compared with controls, except for total cholesterol, which was even lower in patients with CS than in controls. In addition, no correlation existed between RDW and the lipidic parameters. Interestingly, the study by Kim et al, 13 conducted among patients with ischemic stroke and hypercholesterolemia, showed lower RDW than those without. However, as compared to our data, Ani and Ovbiagele 12 and Ntaios et al 14 did not observe any association between RDW and dyslipidemia. In a recent article on unselected outpatients from a general population, Lippi et al 25 observed that RDW was negatively associated with high-density lipoprotein cholesterol and positively associated with the atherogenic index of plasma. In this sense, Vayá et al 26 and Sánchez-Chaparro et al 27 found an association of RDW with metabolic syndrome and others with obesity, 24,28 hypertension, 29 and diabetes. 30 Given that CS affects a young population, and since we did not observe significant differences in the prevalence of cardiovascular risk factors (except higher obesity), the lack of correlation between RDW and plasmatic lipids is not surprising.
Our results indicate that, although leukocytes >8 × 103/µL increased the risk of CS in the univariate logistic regression analysis, after adjusting for confounders (fibrinogen >382 mg/dL, age >40 years, gender, and anemia) in the multivariate regression analysis, RDW >14% was the only parameter that independently increased the risk of CS 2.5 times. Increased RDW values have been recently reported in several cardiovascular disorders, such as ischemic heart disease, acute and chronic heart failure, peripheral occlusive disease, 7 deep vein thrombosis, 9 –11 and pulmonary embolism. 8 The RDW was also increased in inflammatory diseases, that is, systemic lupus erythematosus, 31,32 inflammatory bowel diseases, 33,34 and Behçet disease, 35,36 and has been shown to maintain its significance independently of anemia and inflammatory status. 9 –11,31 –38 After considering RDW in these various clinical settings, it seems that increased RDW is nonspecific and expresses a “pathological” state, irrespectively of the disease under study.
In the present study on patients with CS, we have determined erythrocytes indices as compared to other ischemic stroke studies, 12 –15 which has allowed us to confirm the correlation of RDW with the erythrocyte indices. This suggests that anisocytosis in patients with CS is related to altered erythropoietic mechanisms, and that it does not seem to be related to inflammation, anemia, or dyslipemia.
In conclusion, RDW >14% increases the risk of CS by 2.5-fold and constitutes a predictor of CS independently of anemia and inflammation. Further studies are needed to assess the possible mechanisms involved in the increased RDW that characterizes these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the PN de I+D+I 2008-2011 (ISCIII Red Investigación Cardiovascular RD12/0042/0029, Spain).