
Abstract
Patients with intermittent claudication have significantly higher levels of inflammatory biomarkers, particularly interleukins, which is also a consequence of exercise limitation. Physical activity, which is one of the preventive measures against atherosclerosis, is associated with a decrease in inflammatory biomarkers. Therefore, in our study, we investigated the effects of revascularization of peripheral arteries in patients with intermittent claudication on functional capacity and levels of inflammatory markers. The study included 26 patients with intermittent claudication who underwent percutaneous transluminal angioplasty (PTA). Before the procedure and 2–4 months after successful revascularization, the ankle-brachial index (ABI), functional capacity using the treadmill test, and the walking impairment questionnaire (WIQ) were determined. Inflammatory biomarkers were also measured before and after procedures. Successful revascularization was associated with an increase in intermittent claudication: 120 (20–315) versus 300 (100–1000 m), P < 0.001. Treadmill testing showed a significant increase in initial and maximal walking distance. After revascularization, ABI increased significantly (0.55 vs 0.82, P < 0.003). Improvement in functional performance was also demonstrated by WIQ. Two to three months after revascularization, some inflammatory biomarkers decreased significantly: fibrinogen, interleukin-6 (IL-6), and interleukin-8 (IL-8). The high-sensitivity C-reactive protein (hsCRP) and tumor necrosis factor-alpha (TNFα) also did not decrease significantly. The levels of some inflammatory markers: IL-6, TNFα, and fibrinogen were significantly related to the improvement in patients’ functional capacity. The results of our study show that successful revascularization of the lower limb arteries not only improves the functional capacity of patients with intermittent claudication, but also reduces the systemic inflammatory response and may have a preventive effect on local and concomitant other atherosclerotic diseases.
Keywords
Introduction
Peripheral arterial disease (PAD) is a manifestation of atherosclerotic vascular disease, which is considered a low-grade chronic inflammatory process. Inflammation plays a role in all phases of the disease, from its onset to the thrombotic complications of atherosclerosis. Therefore, inflammatory biomarkers are a target in the quest to improve the diagnosis and prognosis of various atherosclerotic diseases, including PAD. Inflammatory or tissue cells activated during inflammation have been shown to be associated with poor prognosis in PAD. 1 Recently, new inflammatory biomarkers have been found that are useful for identifying individuals with atherosclerotic disease. In patients with PAD, elevated YKL-40 levels have been shown to be independently associated with poor long-term survival and YKL-40 levels have been shown to correlate with patients’ ankle-brachial index (ABI). 2 In patients with intermittent claudication, some inflammatory biomarkers increase with acute exercise. However, long-term exercise and rehabilitation of patients with PAD reduces endothelial cell apoptosis, improves endogenous antioxidant markers, and reduces endothelial cell-derived inflammation. 3 Treatment of the advanced form of PAD, including intermittent claudication and critical leg ischemia (CLI), is based on revascularization procedures of the lower limb arteries. Percutaneous transluminal angioplasty (PTA) is a relatively safe and effective procedure for reopening peripheral arteries. Successful revascularization improves the functional capacity of these patients.3,4
Patients are therefore expected to improve their physical activity and quality of life after successful reopening of the peripheral arteries. As it has been shown that higher levels of physical activity were associated with lower levels of inflammatory markers in PAD patients, in our study we investigated the effects of percutaneous revascularization of the lower limb arteries on the levels of inflammatory biomarkers and whether the levels of the biomarkers were related to the changes in functional capacity of PAD patients after successful revascularization.
Patients and Methods
The study was conducted in an outpatient clinic of the Department of Vascular Diseases at the University Medical Centre Ljubljana between June 2019 and January 2020. Patients referred for vascular examination were screened for eligibility for the study. The inclusion criterion for the study was an objectively confirmed diagnosis of PAD (ABI ≤ 0.90) with a stable claudication distance (50–350 m). Patients with femoral, femoropopliteal, and iliofemoral arterial occlusions were included. Patients were excluded if they had undergone previous revascularization, had ischemic ulcers or rest pain, were limited in their ability to walk due to other health conditions, had advanced heart failure, chronic obstructive pulmonary disease, advanced renal failure, neuromuscular disorders, arthritis, or refused consent to participate in the study. A total of 113 patients with PAD were screened and 26 eligible patients were enrolled in the study (Table 1). They were predominantly male (21/26) and a median age of 68 years.
Demographic and Clinical Characteristics of PAD Patients with Intermittent Claudication Included in the Study.

The values are reported as median (interquartile range) of number and percentage.
Abbreviation: PAD, peripheral arterial disease.
Blood pressure > 140/90 mm Hg or treated hypertension.
LDL cholesterol ≥ 2.5 mmol/L with or without treatment.
A complete history was taken and a detailed clinical examination was performed in all patients before inclusion in the study and 2–4 months after successful revascularization. Ankle-brachial pressure and ABI were determined according to a previously described protocol.5,6
Walking Impairment Questionnaire (WIQ): The modified WIQ, developed by researchers at the University of Colorado Health Science Centre and modified by Coyne and associates, was used. 7 Each symptom was scored from 1 to 5, with 1 point indicating that the patient had no difficulty walking and 5 points categorizing patients who could not perform any type of exercise. If the patient collected a total of 16 points in all 16 categories, it meant that they had no difficulty walking, and if someone had 80 points (16 × 5), it meant that they were unable to perform any type of walking.
Before enrollment in the study, all participants were informed about the study methods and gave written informed consent. The study was approved by the National Medical Ethics Committee (number 67-2019-4) and the principles of the Declaration of Helsinki were followed.
Laboratory Investigation
Blood samples were taken from all patients one week before the procedure (PTA) and 2 to 4 months after PTA. Basic laboratory tests (glucose and cholesterol) were performed with standard colorimetric tests using a Vitros Fusion 5.1 analyser (Ortho Clinical Diagnostics, USA). Plasma levels of C-reactive protein (CRP), interleukins (IL-6, IL-8, IL-10), and tumor necrosis factor-alpha (TNFα) were measured using an ELISA method (R&D Laboratories, Minneapolis, MN, USA).
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD). Mann–Whitney U test was used to compare continuous variables and Fisher's exact chi-square test was used to compare categorical data.
Statistical analyses were conducted using IBM SPSS Statistics for Windows, version 23.0. Armonk, NY: IBM Corp., USA.
Results
The demographic data of 26 patients with intermittent claudication included in this study are shown in Table 1. Most patients had one or more risk factors for atherosclerosis. Most of them were smokers or former smokers and half of them had arterial hypertension. All patients had claudication in one leg. In five patients, PAD was associated with coronary artery disease and six patients had asymptomatic atherosclerosis of the carotid artery. Most patients had occlusions of the iliac artery and the superficial femoral artery.
The patients’ functional performance improved significantly after revascularization (Table 2). The patients’ medical history showed a prolongation of the claudication distance by up to threefold. The treadmill test also confirmed a significant improvement in initial as well as maximum claudication distance and the WIQ showed an improvement in overall functional capacity after successful revascularization. The ABI increased by more than 50%. Table 3 shows the values of inflammatory biomarkers before and 2–4 months after successful revascularization of the lower limb arteries. It showed that IL-6, IL-8, and fibrinogen decreased significantly after successful procedure. There was also a trend toward lowering TNFα and hsCRP.
Tests of Functional Capacity, Walk Tests, a Walking Impairment Questionnaire, and ABI Before and After Intervention (PTA or PTA with Stent Implantation) Performed in Patients with PAD.

The values are reported as median (interquartile range) of number and percentage.
Abbreviations: ABI, ankle-brachial index; WIQ, walking impairment questionnaire; PAD, peripheral arterial disease; PTA, percutaneous transluminal angioplasty.
Inflammatory Biomarkers in Patients with PAD Before and After Revascularization Procedures.
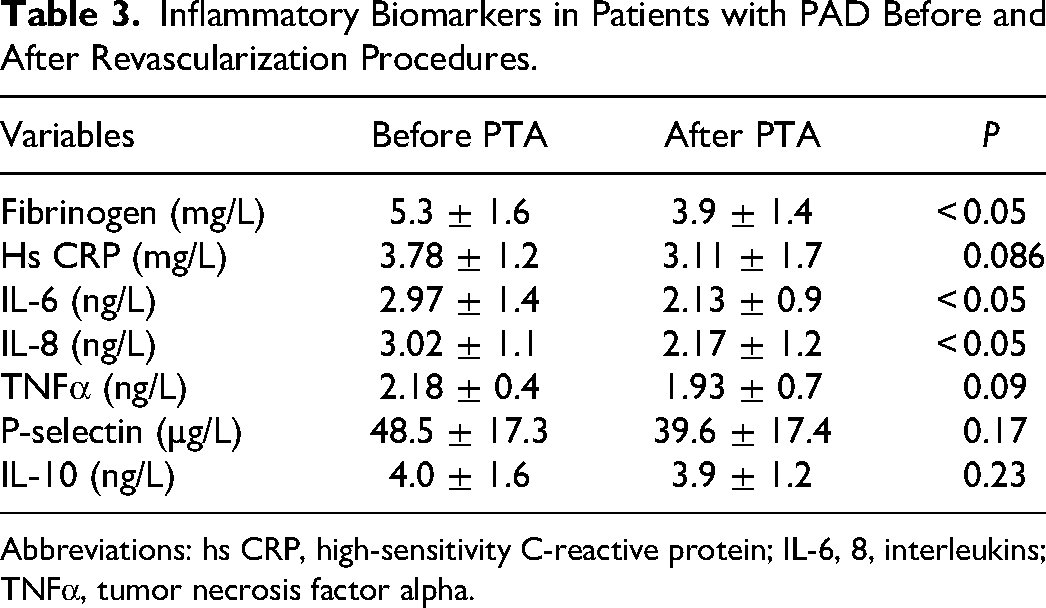
Abbreviations: hs CRP, high-sensitivity C-reactive protein; IL-6, 8, interleukins; TNFα, tumor necrosis factor alpha.
One of the most interesting findings was the correlation between the changes in the levels of some inflammatory markers and the improvement in functional capacity after successful revascularization (Table 4). After revascularization of the peripheral arteries, the increase in ABI was significantly related to the decrease in fibrinogen and IL-6 levels. The improved functional capacity shown by the treadmill test was significantly related to the decrease in IL-6 and TNFα. In addition, WIQ, which indicated improvement in walking ability, was significantly related to fibrinogen and IL-6 levels. A borderline relationship was also found between WIQ and hsCRP. The increase in ABI as a standard measure of revascularization success was related to fibrinogen and IL-6 levels, and a relationship was also found between ABI and IL-8 and hsCRP.
Relationships Between Differences of Functional Capability and Changes in Levels of Inflammatory Markers Before and After Successful Revascularization of Arteries of Lower Limbs.

Abbreviations: IL-6, 8, interleukins; TNFα, tumor necrosis factor alpha; hs CRP, high-sensitivity C-reactive protein; WIQ, walking impairment questionnaire; ABI, ankle brachial index; IC, intermittent claudication.
Discussion
In our study, patients with PAD had elevated levels of inflammatory markers, including IL-6, fibrinogen, and TNFα, before the procedure, compared with subjects without PAD.8,9 After successful revascularization of the lower limb arteries, confirmed by angiography and elevated ABI immediately after the procedure, our patients’ functional capacity improved significantly. Claudication disappeared in most patients (17 out of 26), while it was significantly prolonged in others. The WIQ test also showed improvement in daily functioning. An increased inflammatory response as a result of risk factors of atherosclerosis leads to an invasion of inflammatory and immune cells into the injured arterial wall. Activation of these cells triggers inflammatory markers, particularly cytokines. 10 Fibrinogen, CRP, and cytokines, particularly IL-6, TNFα, and IL-10, are the most commonly described inflammatory markers in atherosclerosis, including PAD.11,12 Recent evidence, therefore, supports the view that inflammation plays a key role in the initiation and progression of vascular damage. 13 Studies have shown that inflammation plays an active role in the pathogenesis of PAD and that the relative risk of developing PAD increases with each quartile of CRP level. 14 Among inflammatory biomarkers, the pro-inflammatory cytokine IL-6 was found to be the strongest predictor of PAD and was independently associated with disease progression. 15
Lifestyle modification, particularly physical activity, reduces inflammatory markers by decreasing adipocytokine production and cytokine release from skeletal muscle and endothelial cells and improving oxidative status.16,17 In patients with intermittent claudication, exercise and physical performance are impaired and may be a reason for the elevated levels of inflammatory markers that promote the progression of local disease and atherosclerosis in other vascular beds. Therefore, we expected that successful revascularization of lower limb arteries, eliminating claudication, would improve functional capacity and exercise ability in these patients, which could reduce proinflammatory circulating biomarkers.
Improvement in functional capacity is one of the most important indicators of the success of peripheral artery revascularization.4,18 It improves patient mobility and functional capacity, which was also shown in our study. 19 Physical activity is one of the basic preventive measures for atherosclerotic disease. However, physical activity may have opposite effects on inflammatory biomarkers. Acute exercise ischemia increases the production of inflammatory cytokines,20,21 especially in obese individuals. 21 One of our studies showed that acute exercise-induced intermittent ischemia induces endothelial dysfunction associated with a systemic inflammatory response in patients with PAD. 22 Acute exercise may also influence the release of circulating angiogenic cells and microparticle populations that play a role in vascular health. 23 Therefore, acute exercise, which produces elevated levels of biomarkers, particularly inflammatory markers, may be responsible for advanced atherosclerosis in various areas of the arterial system in PAD patients.
However, regular physical activity has an anti-inflammatory effect. Regular physical activity leads to an increase in systemic levels of cytokines and chemokines with anti-inflammatory properties. 16 This suggests that regular physical activity exerts an anti-inflammatory effect, with the interaction between contracting muscles and circulating cells providing the anti-inflammatory effect. 16 Studies have also shown that exercise reduces inflammatory markers by decreasing the production of adipocytokines and their release from skeletal muscle, endothelial cells, and the immune system. 17
In our patients, functional performance tests (treadmill, WIQ) showed that functional performance improved and that this was associated with a decrease in some inflammatory markers, particularly interleukins. Interleukins were found to be the most specific inflammatory markers of vessel wall inflammation. The inflammatory response of vessels to the deleterious effects of risk factors involves a complex interaction between inflammatory cells, endothelial cells, and vascular smooth muscle cells. It is associated with the expression of cytokines that interact with mitochondria and increase the production of reactive oxygen species. Elevated levels of inflammatory markers are associated with vascular dysfunction and morphological deterioration of the vessel wall, including atherosclerosis. Following successful revascularization of occluded peripheral arteries, a decrease in inflammatory markers, particularly interleukins and fibrinogen, was expected as this improved functional capacity in these patients. In our study, the improvement in walking ability after successful revascularization and the associated decrease in systemic levels of some inflammatory markers were shown in a relatively short time. Against this background, successful revascularization that removes obstacles to ambulation could be considered a useful weapon against local vascular and systemic inflammation causing atherosclerosis and could have a preventive effect on local and systemic diseases.
Conclusions
Atherosclerosis, including PAD, is a low-grade chronic inflammatory process. Successful revascularization of peripheral arteries improves functional capacity in these patients and lowers levels of some inflammatory markers, particularly interleukins, fibrinogen, and TNFα. Therefore, the removal of obstacles to movement, such as the removal of occlusions of peripheral arteries, could be considered a useful tool against local vascular and systemic inflammation in atherosclerosis and prevent local and systemic disease progression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.