
Abstract
Objectives:
We evaluated the relationship between neutrophil to lymphocyte ratio (NLR) and slow coronary flow (SCF).
Methods:
A total of 180 participants were recruited to the present study. Of all the participants, 82 patients were with SCF and 98 participants were with normal coronary arteries. Basal characteristics were recorded. Coronary flow was quantified by thrombolysis in myocardial infarction frame count.
Results:
Basal characteristics were similar between the 2 groups. The NLR was significantly higher in the SCF group when compared to the control group (2.3 ± 0.8 and 1.5 ± 0.4 respectively, P < .001). In multiple logistic regression analysis, NLR remained as the independent predictor of SCF (P < 0.001).
Conclusions:
Our findings showed that NLR was significantly higher in the SCF group when compared to the control group with normal coronary arteries. We also showed that NLR was related to the presence of SCF rather than the extent of SCF. Besides these findings, we also showed the NLR as an independent predictor of SCF.
Introduction
Slow coronary flow (SCF) is characterized by delayed opacification of coronary arteries in the absence of obstructive coronary artery disease (CAD) in coronary angiography. This phenomenon was first described by Tambe and collegues in 1972. 1 The incidence of SCF reported in a study was 1% in patients who underwent coronary angiography for suspicion of CAD. 2
Coronary atherosclerosis, disturbed microvascularization functions, and endothelial dysfunction were reported to be closely related to SCF. 3,4,5 It was shown that there is significant relationship between inflammatory markers and coronary flow rate. 6,7 In recent studies, it was shown that neutrophil to lymphocyte ratio (NLR) is a sensitive marker of various inflammatory diseases, and it was proposed as a predictor of worse cardiovascular outcomes in different clinical settings. 8,9
To our knowledge, there is no published data on the relationship between NLR and SCF. We hypothesized that NLR may be associated with SCF, because an increased NLR was shown to be closely associated with inflammation and atherosclerosis. Therefore, in this study we aimed to evaluate the relationship between coronary blood flow rate and NLR.
Methods
Patients
In this study, a total of 8250 patients who underwent coronary angiography between January 2008 and January 2012 were retrospectively evaluated. Totally, 180 individuals were recruited to the present study. The study group included patients with SCF (n = 82). The control group consisted of age- and gender-matched participants who were selected in a consecutive manner from the catheterized patients during the same study period and who have been proved to have normal coronary arteries (n = 98).
Exclusion criteria were the presence of at least one of the followings: acute coronary syndrome, significant valvular heart disease, decompensated heart failure, malignancy, renal or hepatic failure, acute or chronic infectious disease, autoimmune disease, anemia (hemoglobin level of <12 g/dL in women or <13 g/dL in men according to World Health Organization criteria), hematologic disease, and acute or chronic pulmonary disease.
Angiographic Analysis
The indication for coronary angiography was either the presence of typical chest pain or positive or equivocal results of noninvasive screening tests for myocardial ischemia. Coronary angiographies were performed by femoral approach using Judkins’ technique.
During the coronary angiography, iopromide (Ultravist 370, Schering AG, Berlin, Germany) was used as the contrast agent in all patients and control participants.
Two observers who were blinded to the clinical details of individual participants independently quantified the coronary flow using the thrombolysis in myocardial infarction frame count (TFC) as previously described. 10 Shortly, in this method, the number of cine frames that was recorded at 30 frames/s required for the contrast to first reach standard distal coronary landmark in left anterior descending (LAD) artery, left circumflex (LCX) artery, and right coronary artery (RCA) were measured. Predefined distal landmarks were as follows: the distal bifurcation for LAD, distal bifurcation of the segment with longest total distance that includes the culprit lesion for the LCX, and the first branch of posterolateral artery for the RCA.
Because the LAD coronary artery is usually longer than the LCX and the RCA coronary arteries, the TFC for LAD coronary artery is often higher compared to others. Therefore, the TFC for LAD was divided by 1.7 to obtain the corrected TFC.
Study participants with a TFC greater than 2 standard deviations from the normal published range for any 1 of the 3 coronary arteries (>40.6 frames for LAD, >29.8 frames for LCX, and >27.3 frames for RCA) were accepted as an indicator of SCF.
Laboratory Analysis
Basal clinical characteristics were reviewed. Laboratory parameters (including complete blood count (CBC), biochemistry panel, and cholesterol panel that were taken before the index coronary angiography) of all the participitants were recorded. In our instutition, the blood samples are routinely collected after 12-hour fasting in the morning hours of 8.00
Statistical Analysis
Statistical analysis were performed by using SPSS 16.0 Statistical Package Program for Windows (SPSS Inc, Chicago, Illinois ). Continuous variables were given as the median ± standard deviation, and categorical variables were defined as percentages. Student t test or Mann-Whitney U test was used to compare continuous variables. Categorical variables were compared with Chi-square test. In order to define the relationship between SCF and possible confounding factors, logistic regression analysis was used. A P value of <.05 was accepted for statistical significance.
Results
The patients’ basal characteristics for the SCF and control groups were summarized in Table 1. The characteristics of the 2 groups were similar. Laboratory parameters of the groups are given in Table 2. White blood cell count was higher in the SCF group (7.7 ± 1.6, 8.2 ± 1.9, P = 0.044). Neutrophil number was higher in the SCF group, and lymphocyte count was higher in the control group. Although the level of high-density lipoprotein (HDL) was lower in the SCF group, it did not reach statistical significance. The calculated NLR was significantly higher in the SCF group when compared to the control group (2.3 ± 0.8, 1.5 ± 0.4 respectively, P < 0.001; Figure 1). When we compared the groups, it was seen that NLR was related to the presence of SCF rather than the extent of SCF (Figure 2).
Basal Characteristics of Groups (SCF and TFC).
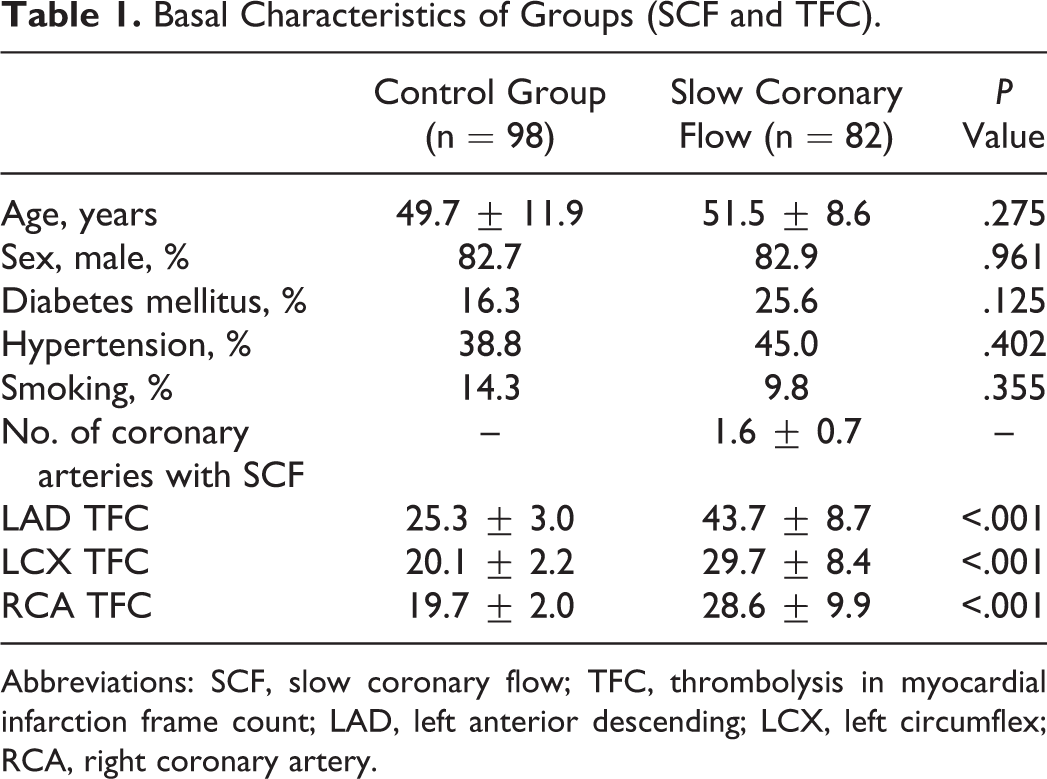
Abbreviations: SCF, slow coronary flow; TFC, thrombolysis in myocardial infarction frame count; LAD, left anterior descending; LCX, left circumflex; RCA, right coronary artery.
Laboratory Parameters of the 2 Groups (HDL and LDL).
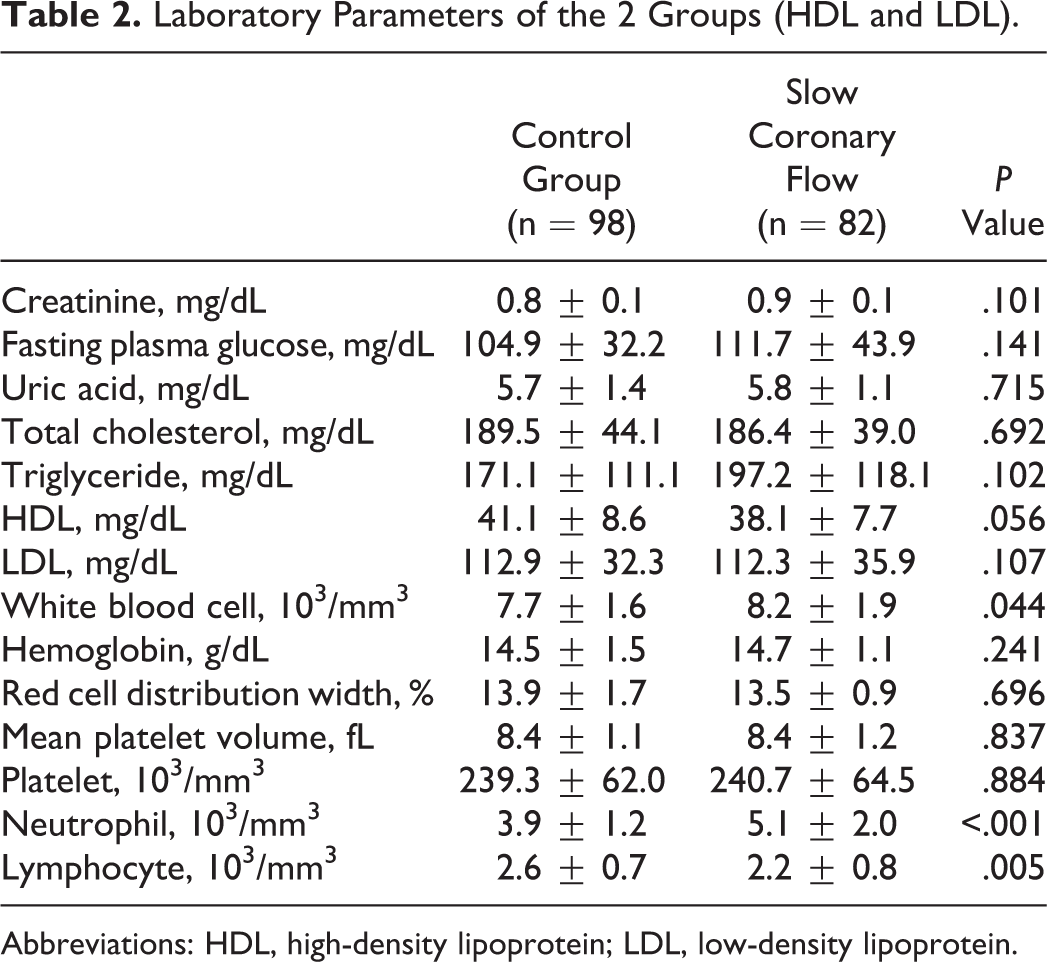
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
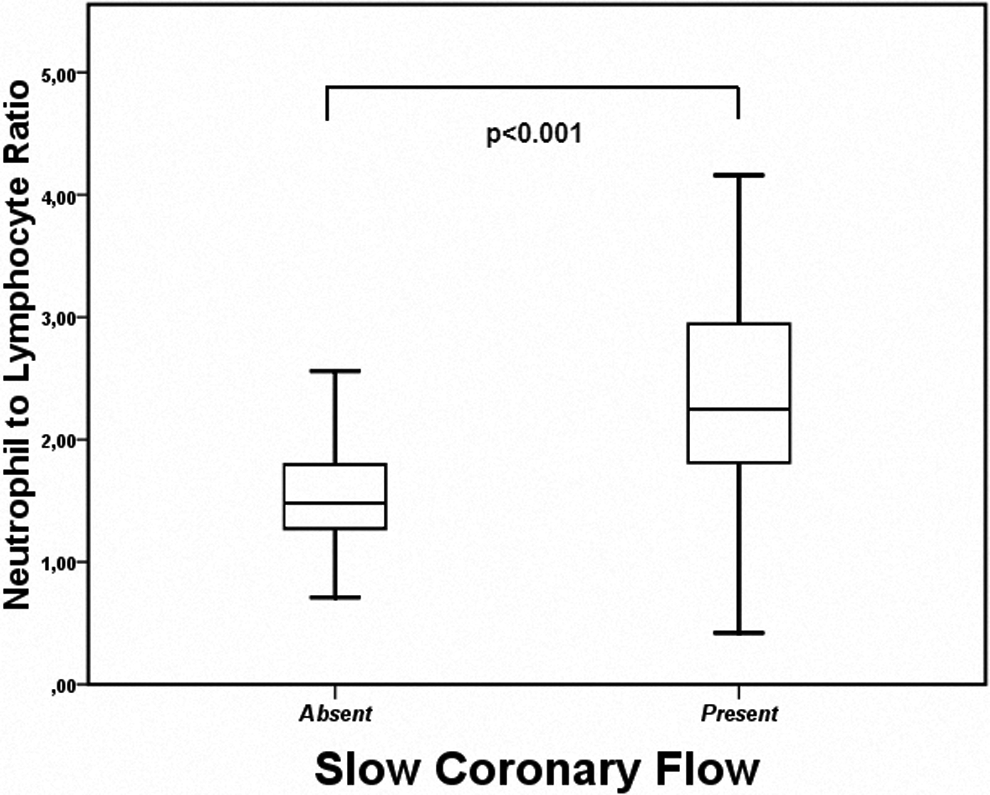
Neutrophil to lymphocyte ratio according to the presence or absence of slow coronary flow phenomenon.
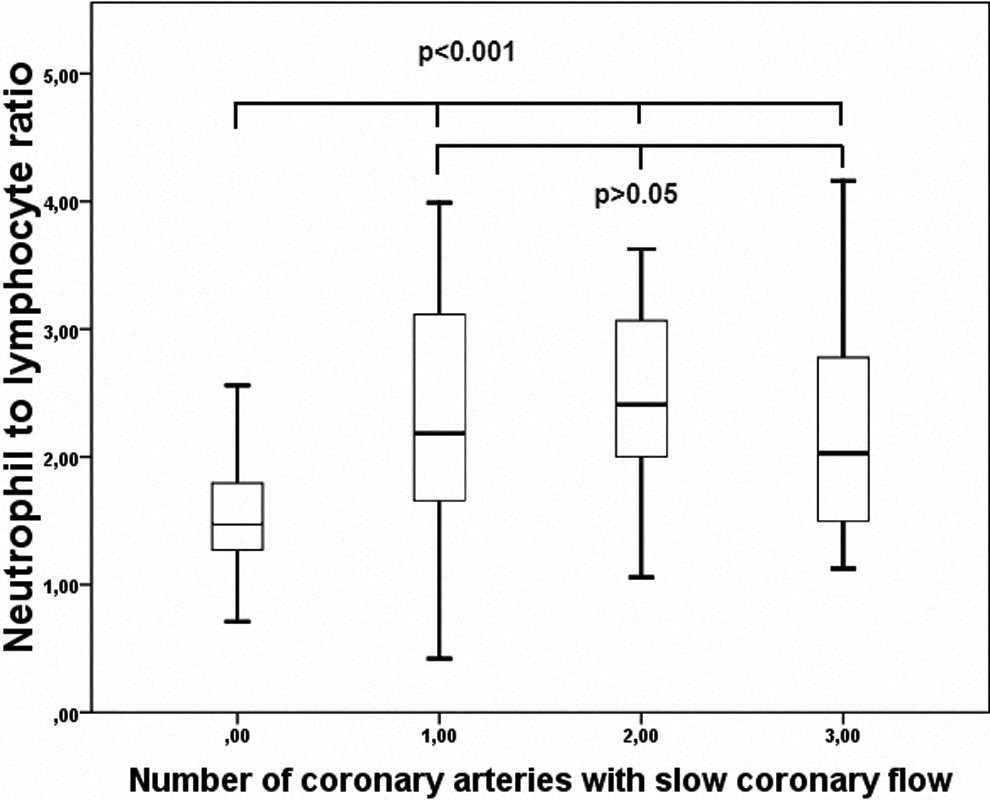
Relationship between neutrophil to lymphocyte ratio and extent of slow coronary flow.
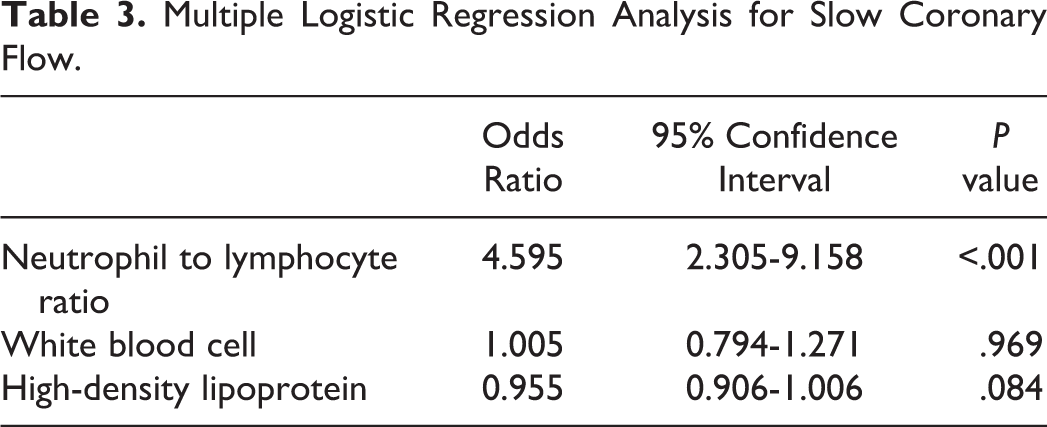
To determine the possible confounding factors for SCF, logistic regression analysis was used. In univariate analysis, NLR (P < .001), white blood cell count (P = .047), and HDL (P = .059) remained for multivariate analysis. In multiple logistic regression analysis, the NLR remained as the independent predictor of SCF (Table 3).
Multiple Logistic Regression Analysis for Slow Coronary Flow.
Discussion
In the present study, we demonstrated the independent association between NLR and SCF. We showed that patients with SCF had increased NLR when compared to the control group with normal coronary arteries. We also showed that the NLR was related to the presence of SCF rather than the extent of SCF. To the best of our knowledge, our study is the first report focusing on the relationship between the NLR and the SCF.
The underlying pathophysiological mechanisms of SCF are still remaining to be unclear. Different etiological insults have been proposed previously. Microvascular injury and microvascular disease, endothelial dysfunction, and atherosclerosis are the possible causes of SCF. 11,12 Gokce et al showed that platelet function disorder may be another responsible agent for pathogenesis of SCF. 13 Inflammation may be another possible insulting factor for the pathogenesis of SCF. Li et al showed that plasma C-reactive protein (CRP) and interleukin 6 levels were significantly elevated in patients with SCF. 14 In another study, it was demonstrated that the levels of soluble adhesion molecules in patients with SCF were increased, and the authors suggested that their findings could be interpreted as a sign of endothelial activation and inflammation in patients with SCF. 15 Similarly, Barutcu et al found increased high-sensitivity CRP (hsCRP) levels in patients with SCF when compared to the control group. 16
Inflammation has been shown to be an important pathogenic insulting factor for various cardiovascular diseases including coronary heart disease. In this regard, NLR has been shown to be closely related to numerous inflammatory diseases including some cardiovascular diseases. For example, Kaya and collegues showed that NLR was closely related to the severity of atherosclerosis. 17 Severe atherosclerosis was accompanying with higher levels of NLR. Turak et al proposed NLR in the prediction of bare metal stent restenosis. 18 In another study, it was shown that NLR ratios were increased in patients with coronary artery ectasia. 19
Similarly, it was shown that NLR is also related to morbidity and mortality in cardiovascular diseases. In the study of Duffy et al, it was demonstrated that NLR was useful in prediction of long-term survival after percutaneous coronary intervention. 20 In another study, Lee et al showed that increased postmyocardial infarction NLR levels were independent predictor of major adverse cardiovascular end points in patients with diabetes. 21 Shen and colleagues proposed NLR as an independent predictor of long-term mortality after ST-segment elevation myocardial infarction in whom early revascularization was performed. 22
Because there were important data suggesting a close relationship between SCF phenomenon and inflammation, we hypothesized that NLR (which has been shown to be a poor prognostic inflammatory marker) could be increased in patients with SCF. According to our findings, NLR was significantly higher in patients with SCF, and we also showed that NLR was independently associated with SCF phenomenon. According to our findings, it can be proposed that increased number of neutrophils can take a role in pathophysiology of SCF. Capacity of neutrophils in inflammatory processes, roles of cytokines released from neutrophils, and interaction of neutrophils and their cytokines with platelets might have a role in the mechanism of development of this poorly understood disease. In another words, increased NLR could be a sign of increased inflammatory status in patients with SCF. To clear these mechanisms, further studies are needed.
Study Limitations
There are some limitations of our present study. First of all, the study population was relatively small. Second, this was a retrospective study. Therefore, we could not sought some cytokine or adhesion molecule levels in this patient subset. We also did not perform intravascular ultrasound for patients with SCF, because this was not a routine protocol in this patient subset.
Conclusion
The NLR is increased in patients with SCF and it is significantly and independently associated with this phenomenon. It is an easily available, cheap, and easily calculated parameter of routine CBC. So NLR can be widely used in prediction of SCF. To clear the pathophysiologic role of NLR in SCF, further studies are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.