
Abstract
Patients with atrial fibrillation (AF) have an increased risk of stroke and systemic thromboembolism. Diagnosis of AF is commonly encountered in the emergency department (ED). The purpose of this study was to assess the number of patients with new-onset AF appropriately initiated on oral anticoagulation (AC) during their ED encounter. This retrospective analysis included patients discharged from the ED from July 2016 to July 2021 with a new diagnosis of AF. Patients were excluded if they were on AC before admission. The major endpoint was to identify the percentage of patients discharged from the ED without initiating AC. Minor endpoints included the average CHA2DS2-VASc scores and the reason for not initiating AC. A total of 380 patients were included in the final analysis. Of the 245 patients found to be indicated for AC, only 131 patients (53.5%) were initiated on AC and 114 patients (46.5%) were discharged without initiating AC. Almost half of the patients who presented to the ED with a new diagnosis of AF and indicated for AC were discharged without AC.
Introduction
Atrial fibrillation (AF) is the most common cardiac rhythm disorder and increases in prevalence with age. 1 In the United States (US), the percentage of Medicare beneficiaries with AF in 2010 was as high as 10% for those ≥65 years of age and 2% for those <65 years of age. 2 More than 450 000 patients are hospitalized annually with AF as the primary diagnosis. 2 Furthermore, the annual ED visit for AF has increased by more than 30% from 2007 to 2014. 3 In addition, the prevalence of AF is expected to increase by more than double by 2030.4,5 Stroke prevention is a priority for patients with AF, as the incidence of stroke is estimated to be as high as 20% in patients with AF. 4 Individuals with AF are nearly 5 times more likely to have a stroke compared to individuals without AF. 4 Furthermore, AF-related stroke is associated with increased severity and mortality compared to non-AF-related stroke. 1 Additionally, AF is an expensive disease to treat as it's estimated that treating patients with AF adds US$26 million to the US healthcare cost annually. 6
In patients with AF, there is robust data demonstrating that oral anticoagulation (AC) can effectively prevent systemic embolism, and stroke and reduce mortality. 7 The use of oral AC (OAC) with either warfarin or a direct-acting OAC (DOAC) is recommended by the American Heart Association, American College of Cardiology, Heart Rhythm Society, and the American College of Chest Physicians for patients with a CHA₂DS₂-VASc score of ≥ 2 if female or ≥ 1 in male.8,9 For patients with a new AF finding, delays in OAC initiation expose patients to an elevated risk of stroke and systemic thromboembolism. 9 Moreover, as the population ages, the number of patients presenting to the emergency department (ED) with AF as the primary or secondary diagnosis has markedly increased. 3 Regardless of the high prevalence of AF in the ED, there is a lack of evidence evaluating adherence to the guidelines for initiating AC for patients discharged from the ED with a new diagnosis of AF, and some evidence suggests that despite consensus guidelines, up to 50% of patients with an indication for AC do not receive it. 10
Evaluating adherence to the guidelines recommendations in initiating AC is critical to reducing the risk of stroke in patients with a new AF diagnosis. The purpose of this study was to assess the number of patients who presented to the ED with new-onset AF and then were appropriately initiated on AC during their ED encounter before discharge.
Materials and Methods
This was a single-center, retrospective cohort study at Brigham and Women's Hospital ED, a tertiary care academic teaching hospital. Patients’ medical records were obtained from July 2016 to July 2021 using system-generated reports from the electronic health record. Approval from the Mass General Brigham Institutional Review Board was obtained before the start of this study. Patients were included for screening if they were 18 years of age or older and discharged from the ED with a new diagnosis of AF, so no patients were admitted to the hospital in this study. Then, patients who were already on AC before admission were excluded. Patients with a CHA2DS2-VASc score of ≥2 in females or >1 in males were identified as indicated for AC. The CHA2DS2-VASc and HAS-BLED scores were calculated from the patient's electronic health records.
The major endpoint was to identify the percentage of patients indicated for AC without being initiated on AC during their ED encounter. Minor endpoints included the average CHA2DS2-VASc and HAS-BLED scores, the provider's documentation of why AC was not initiated if patients were indicated for AC, choice of AC if initiated, other concomitant home medications, and whether the Anticoagulation Management Service (AMS) was consulted for follow-up.
Baseline characteristics were collected alongside CHA2DS2-VASc and HAS-BLED scores, discharge date, and whether the patient went for cardioversion in the ED. Chi-square or Fisher's exact tests were used to analyze nominal data. Two-sided Mann-Whitney U-test, Student's t-test, or Wilcoxon signed-rank tests were used for continuous data, as appropriate, with an α level of 0.05.
Results
Of the 547 patients evaluated for inclusion, 167 patients were excluded and 380 patients were included in the final analysis. Of the patients included, 245 patients (64.5%) were identified as indicated for AC based on their CHA2DS2-VASc score, and 135 patients (35.5%) were deemed not indicated for AC (Figure 1). The baseline demographics for the included patients were notable for a mean age of 65 years, 52% females, and a mean body mass index (BMI) of 28 kg/m2 (Table 1).

Patient enrollment.
Baseline Characteristics.

Abbreviations: CHF, congestive heart failure; CVA, cerebrovascular accident; TIA, transient ischemic attack; DAPT, dual antiplatelet therapy, 3 patients on ticagrelor/aspirin, the rest are on clopidogrel/aspirin; NSAIDSs, nonsteroidal anti-inflammatory drugs.
Data expressed as mean ± standard deviation.
Data expressed as n (%).
Calculated creatinine clearance using the Cockcroft-Gault equation.
Data expressed as median (interquartile range).
Of the 245 patients indicated for AC, 131 patients were initiated on AC compared to 114 patients who were not initiated on AC (53% and 47%, respectively, Figure 2). When comparing patients initiated on AC to those that were not, there were more patients diagnosed with hypertension and stage 3 chronic kidney disease in the initiated on AC group (Table 2). The average CHA2DS2-VASc score for the group of patients initiated on AC was higher than the group of patients who were discharged without initiating AC (3.3 ± 1.3 vs 2.8 ± 1.4, P = .02). Nevertheless, 85% of patients from the group of patients discharged from the ED without initiating AC had a CHA2DS2-VASc score of ≥2. All other minor endpoints are outlined in Table 2.

Major endpoint.
Minor Endpoints.

Abbreviations: CHF, congestive heart failure; CVA, cerebrovascular accident; TIA, transient ischemic attack; DAPT, dual antiplatelet therapy; NSAIDSs, nonsteroidal anti-inflammatory drugs.
Data expressed as mean ± standard deviation.
Data expressed as n (%).
Calculated creatinine clearance using the Cockcroft-Gault equation.
Data expressed as median (interquartile range).
For those patients initiated on AC, 96.9% were started on a DOAC and 3.1% were started on warfarin. Apixaban was the most commonly used DOAC (66.1%), followed by rivaroxaban (30.7%) then dabigatran (3.2%). For those that were not initiated on AC during their ED encounter, the most common reason was “defer to primary care provider (PCP).” Figure 3 outlines other reasons providers noted in the chart as to why AC was not initiated. Lastly, 7% of the patients that were indicated for AC were referred to our AMS for further management.
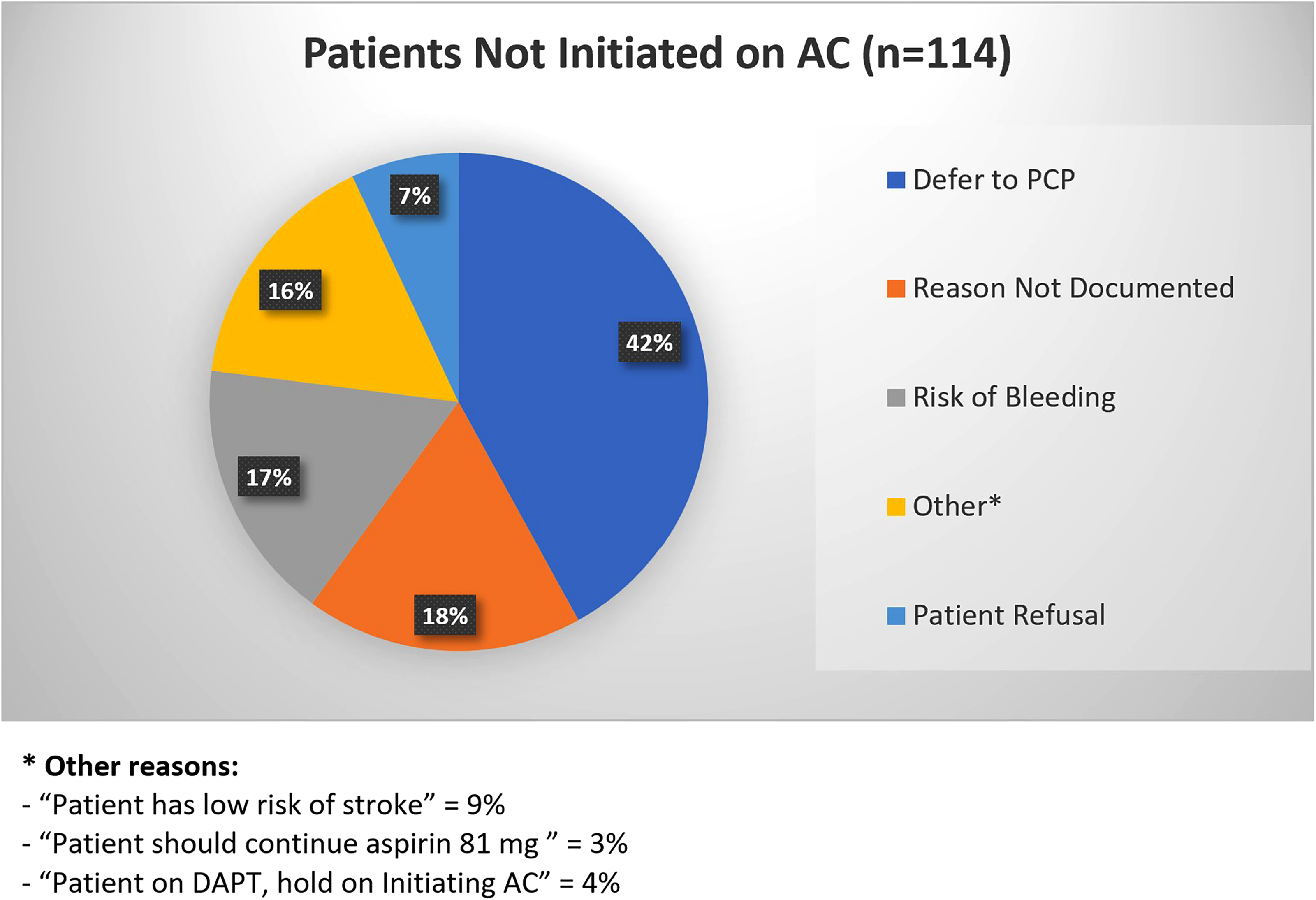
Provider reasons anticoagulation (AC) was not initiated when ACs were indicated.
Discussion
In this retrospective cohort study, we aimed to evaluate the number of patients indicated for AC who were discharged from the ED without initiating AC. This study showed that 47% of the patients indicated for AC were discharged from the ED without initiating AC. The baseline demographics and comorbidities between the group of patients initiated on AC and the group of patients who were not initiated were similar. Even though the mean CHA2DS2-VASc score for patients initiated on AC was higher than those that were not initiated on AC (3.3 ± 1.3 vs 2.8 ± 1.4, P = .02), it's important to note that comparing patients who had a CHA2DS2-VASc score of ≥2 in both groups were similar (93.9% in the AC initiated group vs 85% in the non AC initiated group). This is a clear indication for AC and it implies that 85% of the patients who were not initiated on AC, had an annual risk of stroke from 2.2% to 9.8%, which aligns with the guidelines recommendation of initiating AC to reduce this risk of stroke.8,9 On the other hand, the results of this study are aligned with the guidelines recommendations regarding the choice of AC, where 97% of the patients initiated on AC were initiated on a DOAC. 8 In contrast, the main reason providers noted in the chart for not starting AC when indicated was “defer to PCP.” This delay of initiation of OAC in a newly diagnosed AF patient can expose patients to an elevated risk of stroke.8,9
Previous studies found that the ED is a frequent location for physicians to encounter AF and initiate AC for stroke prevention.11,13 However, multiple studies have shown that the rate of prescribing OAC in the ED is still very low.10,13,14 The findings of this study were similar to a recent review of health records of patients diagnosed with new-onset AF in 2 EDs in Canada where they found, only 17% of 272 patients indicated for AC left the ED with a prescription of OAC. 14 The barriers to initiating AC in the ED have been discussed in previous studies and have found similar results to this study. A recent study found that 52% of ED providers believed that a new AC prescription is the responsibility of the PCP. Then, 41% of the ED providers didn’t start AC due to concerns about bleeding and inadequate follow-up. 12 Other concerns are the lack of patient–provider relationships in the ED leading to incomplete medical history, incorrect risk estimation, and the brief time for proper discussion of the risks and benefits of AC in the ED setting.10,12 On the other hand, a recent study showed that starting AC in the ED rather than waiting for a longitudinal care provider was associated with significantly higher long-term use of OAC. 13 It was also noted that patients who start AC in the ED are more likely to fill their prescriptions as opposed to patients who discharge from the ED without starting AC.13,14
Targeted emergency physicians’ education with updated guidelines and proper utilization of accessible services like AMS for more intensive follow-up are important measures to support the initiation of OAC in the ED. Furthermore, an institutional pathway for patients with newly diagnosed AF in the ED is one way this problem could be targeted. These are critical measures to prevent exposing patients to an elevated risk of stroke through a lack of AC initiation for the prevention of thromboembolism.
There are several limitations to this study. It was single-center and retrospective in nature with a relatively small sample size. We couldn’t assess if AF was the primary or secondary diagnosis, and whether if this influenced AC initiation. Also, the reasoning for not starting AC was not consistently documented in all patients. Finally, future studies are needed to follow-up on patients discharged without initiating AC.
Conclusion
New onset AF in the ED is encountered frequently. In this study, almost half of the patients encountered in our ED were not initiated on AC. It is crucial to implement protocols and/or pathways to optimize the management of patients newly diagnosed with AF in the ED to ensure prompt initiation of AC, where appropriate, and to minimize exposure to an elevated risk of stroke. Future studies are needed to ensure the initiation of AC and identify any boundaries that patients may encounter when starting AC.
Footnotes
Acknowledgments
We acknowledge the countless direct and indirect contributions and efforts awarded to this research. Particularly, our pharmacy colleague, Katie Taylor, PharmD, BCPS who helped in providing ideas and connections with emergency care providers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
There is no funding associated with this study giving it was a retrospective study that was approved by the Institutional Review Board (IRB) at Mass General Brigham, protocol number 2021P002445.
Correction (May 2023):
The title of the article has been edited slightly since its original publication.