
Abstract
Background:
The Asian population with atrial fibrillation (AF) have a higher risk of stroke than the caucasian population and a higher risk of intracranial bleeding when anticoagulated with warfarin. There are few real-world studies comparing the efficacy of non-vitamin K antagonist oral anticoagulants (NOACs) and warfarin among Asian patients to assess its outcomes of ischemic stroke and hemorrhagic stroke.
Methods:
A retrospective cohort study of 1000 patients on dabigatran and warfarin from 2009 to 2013.
Results:
Data were available for 500 patients on dabigatran and 500 patients on warfarin. The average follow-up duration was 315 ± 280 days in the dabigatran group and 355 ± 232 in the warfarin group. The time in therapeutic range (TTR) was 53.2% in the warfarin-treated group, with 32.8% of patients in the subtherapeutic international normalized ratio range of <2. None of the patients in the dabigatran group had ischemic cerebrovascular accident (CVA) compared to 4 (0.8%) patients in the warfarin group, hazard ratio (HR) 0.13, P = .3. There was 1 (0.2%) patient in both dabigatran and warfarin groups with hemorrhagic CVA (HR 1.16, P = .92). There were 3 (0.6%) patients with major bleeding in the dabigatran group compared to 2 (0.4%) patients in the warfarin group (HR 1.57, P = .59).
Conclusion:
There were similar rates of efficacy for outcomes of ischemic CVA, hemorrhagic CVA, and bleeding when comparing dabigatran with warfarin. Our study shows that despite similar efficacy, suboptimal TTR rates and inconveniences with warfarin demonstrate that NOACs are preferred for stroke prevention in AF.
Introduction
Dabigatran etixilate (trade name Pradaxa, Boehringer Ingelheim, Ingelheim, Germany) 1 is a direct thrombin inhibitor and one of several nonvitamin K antagonist oral anticoagulants (NOACs) used for stroke prevention in nonvalvular atrial fibrillation (AF). The large studies in NOACs have included Asian patients albeit in smaller proportions. The RE-LY study compared dabigatran to warfarin in a population spanning 44 countries but included only 15% of trial cohort patients from Asian countries. 2
Asian populations have been shown to have a higher overall risk of stroke than white populations. 3,4 Additionally, it has been suggested from studies that Asians have an increased risk of intracerebral hemorrhage with warfarin when compared to caucasian patients. 5 The RE-LY study, 2 RE-LY Asia study, 6 ROCKET-AF study, 7 and ARISTOTLE 8 trials all showed higher risks of stroke and systemic embolization in Asian patients when compared to non-Asian patients. 9 These studies also showed that the time in therapeutic range (TTR) was lower among Asian patients when compared to non-Asian patients, suggesting that the use of warfarin could be associated with a higher risk of stroke. 9
Aside from multinational trial settings, there have been few studies examining the effect of NOACs compared to warfarin among Asians in real-world clinical practice. For this reason, we conducted a study on the efficacy of dabigatran compared to warfarin among an Asian population.
Methods
The design was a single-center retrospective cohort registry at Malaysia’s National Heart Institute. Dabigatran was licensed for use in our center since 2009, and NOACs are recommended for stroke prophylaxis when the CHA2DS2-VASC score is ≥2. 10 The study included 1000 patients with nonvalvular AF who were prescribed dabigatran and warfarin for stroke prevention between January 2009 to December 2013. These patients were identified via hospital pharmacy electronic records. The sample size of 500 patients on dabigatran was selected based on available numbers of patients at the start of the study and matched equally with 500 patients who were prescribed warfarin in the same time frame. All data were collected from case notes retrospectively. Baseline patient characteristics collected including age and sex of patient, CHA2DS2-VASC score, HAS-BLED score, 11 and echocardiographic data. The dose of dabigatran prescribed was documented. Data on the incidence of any ischemic cerebrovascular (CVA) or hemorrhagic CVA, major bleeding (transfusion of 2 or more units of blood), and minor bleeding (any bleeding without transfusion or requiring <2 units of blood transfusion) were collected. All documented adverse effects, for example, dyspepsia were recorded. Data on follow-up length in days of drug prescription were recorded. Patients who were on warfarin had an international normalized ratio (INR) therapeutic range of 2 to 3. Time in therapeutic range was calculated for patients on warfarin by counting the number of INR values in therapeutic range between 2 to 3 and dividing by the total number of INR measurements (percentage of INRs in range) for the patient. 12 For patients who discontinued warfarin, the reason was recorded.
Mean scores were expressed with ±standard deviation. The baseline characteristics of the cohorts were compared by χ2 test for categorical data and independent sample t test for continuous data. The clinical outcome end points and bleeding events were compared using a Cox regression hazard model and reported with an adjusted hazard ratio with 95% confidence interval. The statistical significance was set at P <.05. The study protocol was approved by the research ethics committee of the National Heart Institute.
Results
Baseline Characteristics
There were 500 patients in the dabigatran group and 500 patients in the warfarin group. There were 205 (41%) patients on dabigatran 110 mg and 295 (59%) patients on 150 mg dabigatran doses. The baseline characteristics of the patients are shown in Table 1. The mean age was lower in the dabigatran group when compared to the warfarin group. There were fewer patients with paroxysmal AF and more patients with persistent AF in the dabigatran group compared to the warfarin group. There were also fewer patients with congestive cardiac failure, hypertension, diabetes mellitus, and vascular disease in the dabigatran group when compared to the warfarin group.
Population Characteristics of All Study Patients.
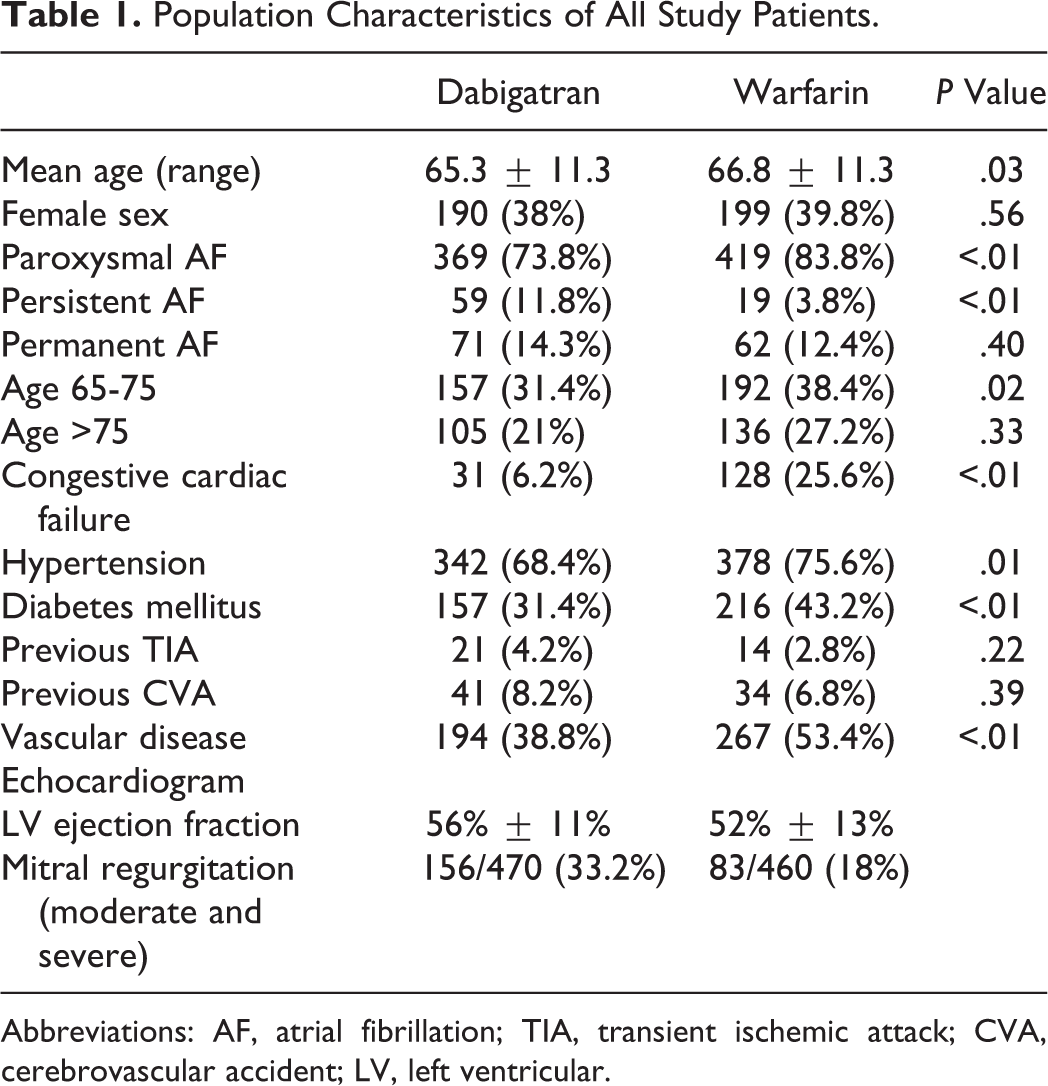
Abbreviations: AF, atrial fibrillation; TIA, transient ischemic attack; CVA, cerebrovascular accident; LV, left ventricular.
The distribution of CHA2DS2-VASc scores is illustrated in Figure 1. The mean CHA2DS2-VASc score was lower at 2.69 ± 1.54 in the dabigatran group and 3.40 ± 1.54 in the warfarin group (P < .01). Our study population included some patients with CHA2DS2-VASc score of 0 due to patients being prescribed dabigatran for procedures such as AF ablation and Direct Current (DC) cardioversion of AF.
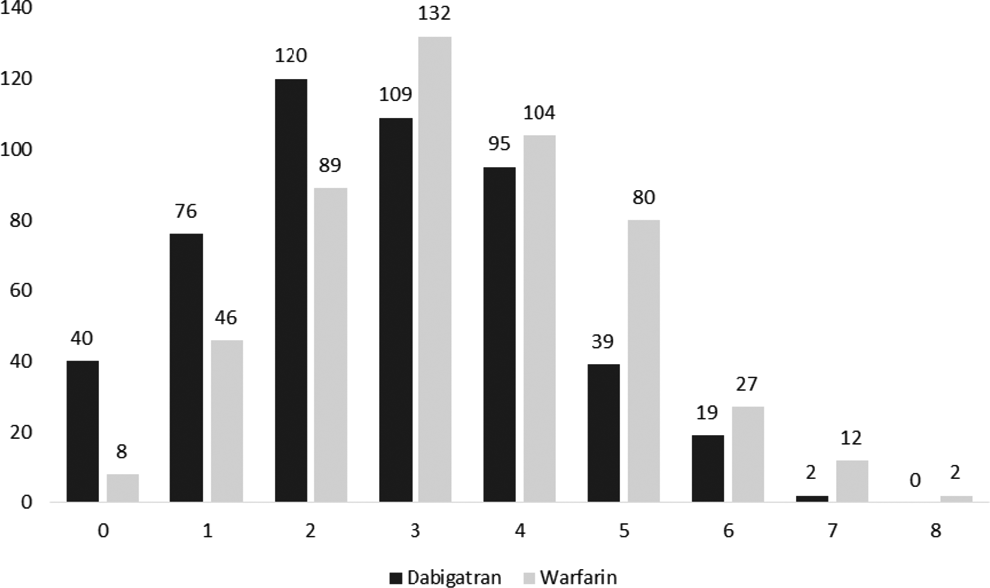
Comparison of CHA2DS2-VASc scores.
The distribution of HAS-BLED scores is illustrated in Figure 2. The mean HAS-BLED scores were similar, being 1.57 ± 0.96 in the dabigatran group and 1.67 ± 0.94 in the warfarin group (P = .11). There were relatively small number of patients (approximately 2% in both groups) with high bleeding risks who had HAS-BLED scores >3. Echocardiogram results were available for 476 (95%) patients in the dabigatran group and 478 (96%) patients in the warfarin groups (Table 1).
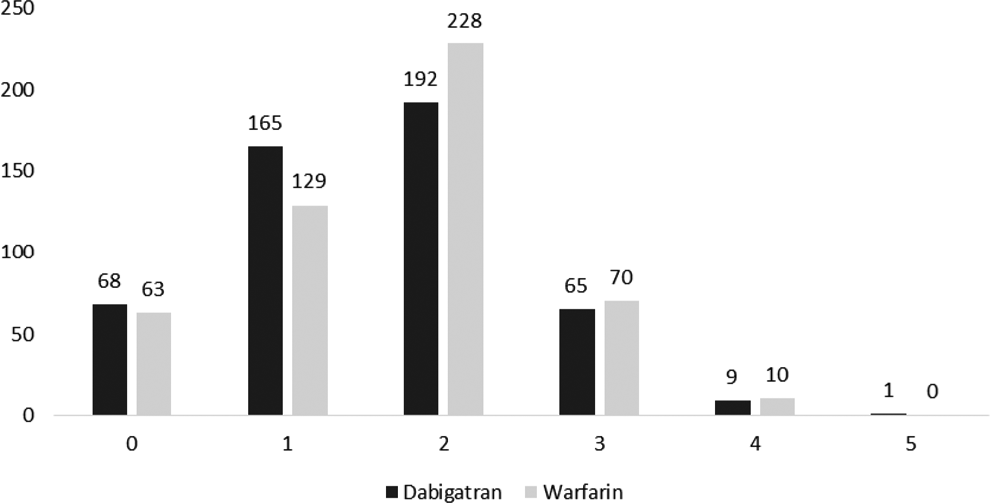
Comparison of HAS-BLED scores.
Efficacy Outcomes
The mean follow-up period was 315 ± 280 days (10.5 months) in the dabigatran group and 355 ± 232 days (11.8 months) in the warfarin group. The rates of ischemic CVA were 0% per year on dabigatran and 0.82% per year on warfarin (Table 2). Of the 4 patients with ischemic CVA in the warfarin group, 1 patient had bilateral cerebellar infarct, 1 patient had left-sided basal ganglia infarct, 1 patient had a small thalamic infarct, and 1 patient had a frontoparietal infarct.
Efficacy Outcomes.

Abbreviations: CI, confidence interval; CVA, cerebrovascular accident.
The rates of hemorrhagic CVA were 0.32% per year on dabigatran and 0.20% per year on warfarin. There was 1 patient in each of the dabigatran and warfarin groups with hemorrhagic CVA. A 86-year-old patient who was on 110 mg of dabigatran had a frontoparietal brain hemorrhage (acute on chronic subdural hematoma), requiring burr hole and subdural drainage. The other patient who was on warfarin had a left-sided basal ganglia bleed diagnosed on computed tomography scan.
Bleeding
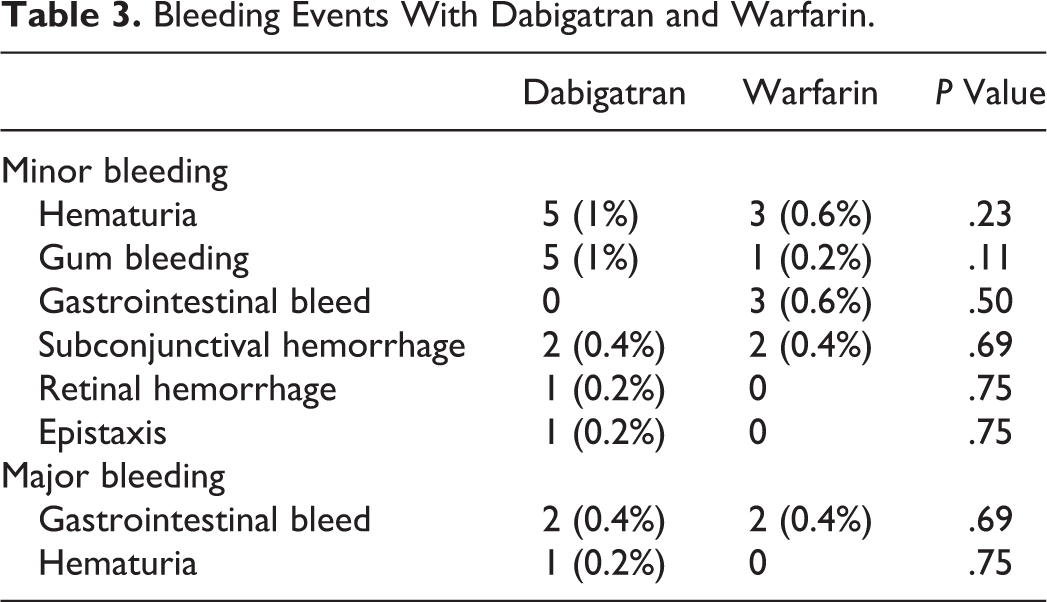
There were 3 (0.6%) patients with major bleeding in the dabigatran group compared to 2 (0.4%) patients in the warfarin group. Hazard ratios were not significantly different for major and minor bleeding when comparing the dabigatran and warfarin groups (Figure 2). The bleeding events are listed in Table 3. Of the major bleeding patients, 1 patient had a hemoglobin (Hb) drop from 13 to 7.8 g/dL and the second patient had an Hb drop from 12.7 to 6.6 g/dL in the dabigatran group. In the warfarin group, there were also 2 major bleeding events, 1 patient had melaena with an Hb drop to 7.7 g/dL and another patient had fresh per rectal bleeding. There were no significant differences in the rate of each type of bleeding, for example, hematuria when comparing dabigatran and warfarin (Table 3).
Bleeding Events With Dabigatran and Warfarin.
Adverse Effects
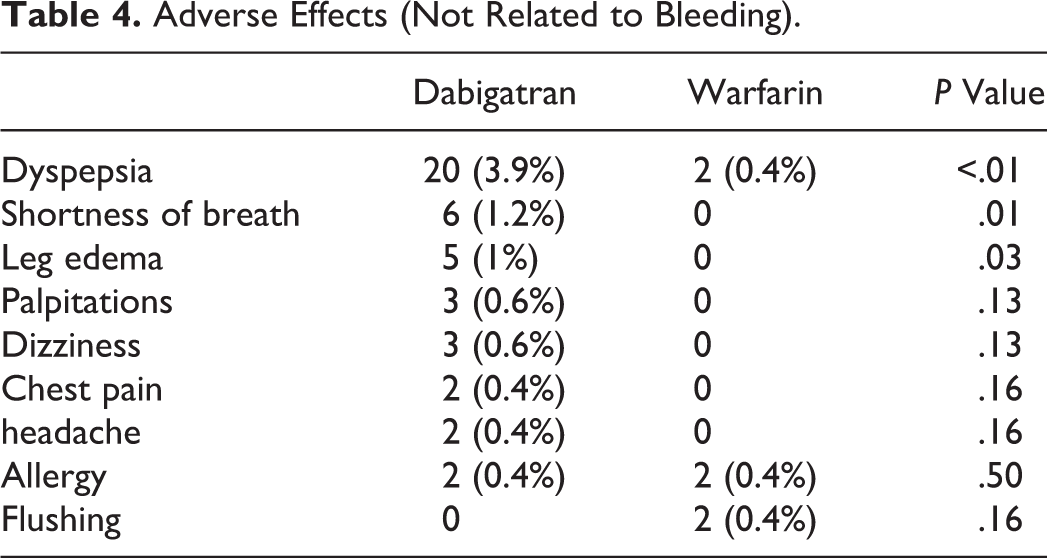
The commonest adverse effect was dyspepsia in the dabigatran group (Table 4). In the dabigatran group, there were significantly more patients who reported dyspepsia (3.9%), shortness of breath (1.2%), and also leg edema (1%).
Adverse Effects (Not Related to Bleeding).
Time in Therapeutic Range
For the 500 warfarin patients, the TTR ranged from 0% to 100% and mean TTR was 53.2% ± 18% (Figure 3).
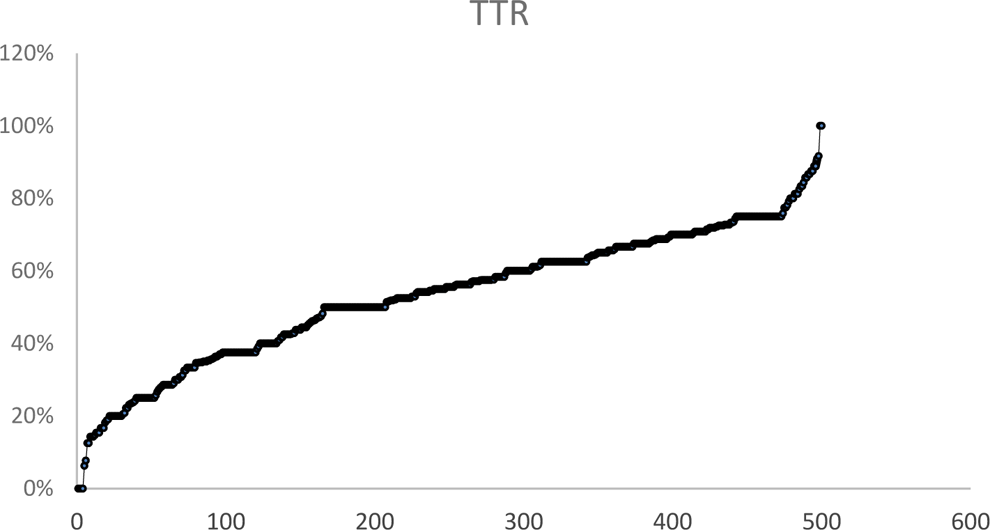
Time in therapeutic range for warfarin.
There were a total of 12 442 INR readings taken for all patients within the time period studied. There were 6944 (53.2%) INR readings in the 2 to 3 range, 3805 (32.8%) INR readings <2, and 1728 (14%) INR readings >3. This indicated that when the INR was outside the therapeutic 2 to 3 range, it was more frequently subtherapeutic than supertherapeutic.
Reasons for Discontinuation of Anticoagulant
There were 92 (18.4%) patients who discontinued dabigatran after a mean follow-up period of 315 days. There were 95 (19%) patients who discontinued warfarin after a mean follow-up period of 355 days. When patients discontinued either anticoagulant, the reasons for discontinuation were documented and are listed in Table 5. The reasons for discontinuation for warfarin frequently relate to inconveniences experienced with the drug and it was likely that the patients who were offered dabigatran as an alternative switched over for improved convenience.
Reasons for Discontinuation of Dabigatran and Warfarin.
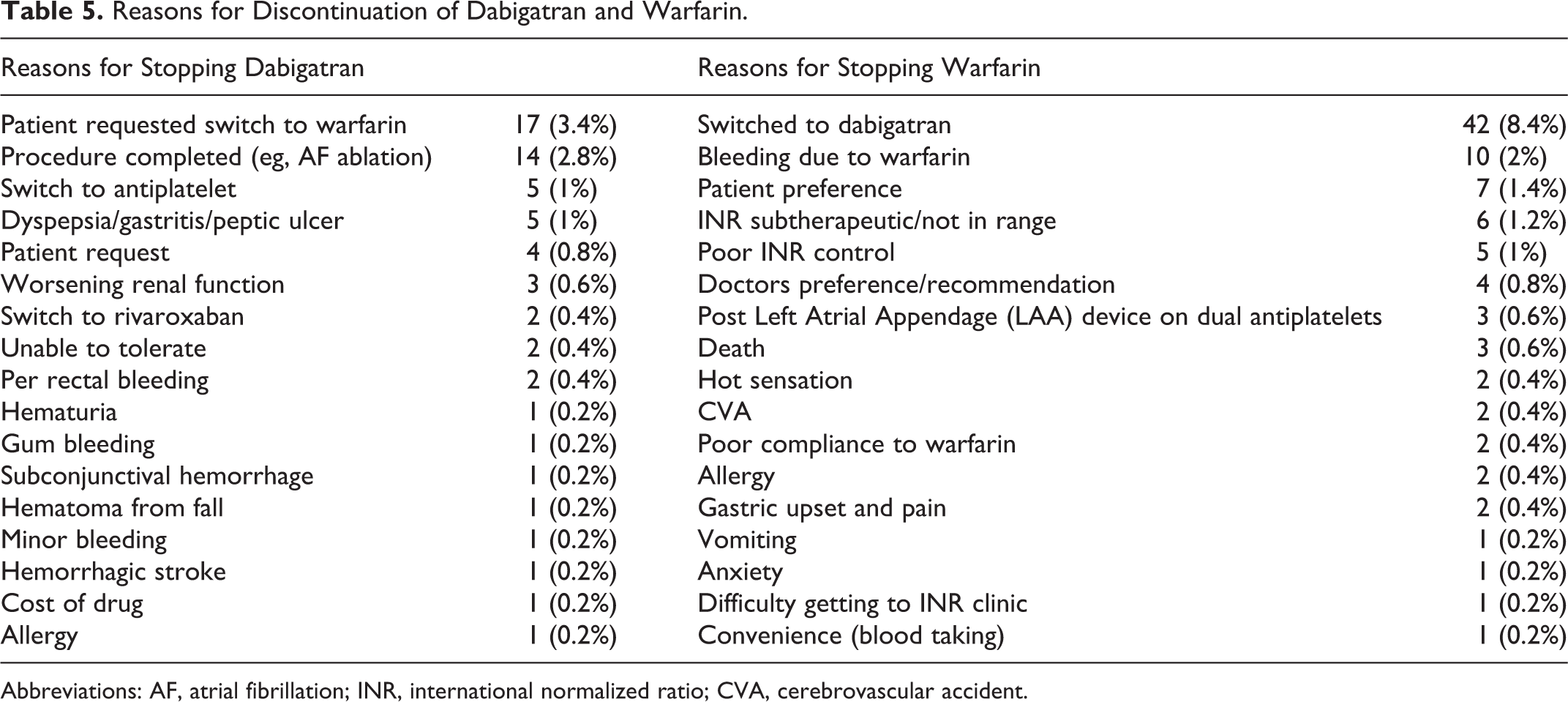
Abbreviations: AF, atrial fibrillation; INR, international normalized ratio; CVA, cerebrovascular accident.
Discussion
There are few real-world studies of the efficacy and effects of dabigatran when compared to warfarin. This is the largest real-world study of dabigatran and warfarin among Asian patients. We found that dabigatran had similar rates of ischemic CVA, hemorrhagic CVA, and bleeding events when compared to warfarin.
Ischemic CVA and Intracranial Bleeding
The RE-LY trial demonstrated the superiority of dabigatran (150 mg dose) over warfarin in preventing ischemic CVA and less hemorrhagic CVA events with dabigatran. 2 However, our study showed that dabigatran was equivalent to warfarin in prevention of ischemic CVA. Among our patients, the trend toward higher ischemic events in the warfarin group may be a reflection of a higher risk profile as demonstrated in the baseline characteristics and also higher CHA2DS2-VASc scores of the warfarin group. The RE-LY Asia study showed a higher rate of hemorrhagic stroke in the warfarin group when compared to dabigatran among Asians. 6 Additionally, intracranial bleeding has been shown to be of concern, particularly among the Asian population. 13 We found that there was a similar rate of hemorrhagic stroke in both dabigatran and warfarin groups (both 0.2%), which is reassuring since dabigatran is a relatively new drug compared to warfarin.
Adverse Effects and Bleeding
Our patients on dabigatran had a dyspepsia rate of 3.9% compared to a rate of over 11% with dabigatran in the RE-LY trial. However, only a small proportion of those patients with dyspepsia (1%) switched to warfarin (Table 5), and this is consistent with findings from other studies of real-world adherence to dabigatran. 14 The RE-LY Asia study showed that both dabigatran 150 mg and 110 mg doses were associated with less major bleeding when compared to warfarin. Our study however found that both groups had similar rates of major gastrointestinal bleeding (0.4% for both groups) with comparatively similar HAS-BLED scores.
Time in Therapeutic Range
When we examined reasons for discontinuing medication (Table 5), dabigatran or other NOACs appear to be preferable to many patients who have issues with the inconveniences of warfarin. This may be even more pertinent in developing countries where the average TTR can be suboptimal. A subgroup analysis of the RE-LY study showed that the TTR in Malaysia was 56%, 15 and in our study the TTR was low at 53.2%. Our study also confirmed that it is more common for the TTR to be subtherapeutic (32.8%) rather than supertherapeutic (14%) as has been previously published. 9 In many Asian countries, recorded TTR values have been suboptimal leading to high stroke rates of 14.3% in Japan in 2007, 16 15.4% in Singapore in 2008, 17 15.2% in Taiwan in 2002, 18 and 13% in China in 2004. 19 In Japan, a lower target INR range, for example, 1.6 to 2.6, is recommended for elderly patients due to concerns of risks of bleeding. 20 It has already been shown that patients with a low (≤30%) TTR have an increased risk of stroke and mortality. 21 Hence, it is likely that the Asian population, especially those with low TTR, could benefit even more from NOACs. 22
Study Limitations
There are limitations due to the study’s retrospective nature. The accuracy of data related to the quality of documentation of the hospital clinical notes, including clinical events and outcomes. The data recorded were dependent on the amount of information given by the patient to the clinician. Since dabigatran was a recently introduced drug, there may have been more awareness in reporting minor adverse events and minor bleeding. Follow-up for the patients was according to clinical indication, for example, at 6 monthly. Some adverse events may not have been reported by patients to our center, and this may account for the lower event rate we found when compared to clinical trials of dabigatran.
Conclusion
We report a real-world study of the clinical efficacy and adverse effects of dabigatran compared to warfarin among Asians. There were similar rates of outcomes of ischemic CVA, hemorrhagic CVA, and bleeding when comparing dabigatran with warfarin. Our study shows that despite similar efficacy, suboptimal TTR rates and inconveniences with warfarin demonstrate that NOACs are preferred for stroke prevention in AF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.