
Abstract
The objective is to examine the separate and joint effects of dynapenia and abdominal obesity on the prevalence of peripheral artery disease (PAD) in older adults of different ages (60-74 and over 75 years old). This study comprised 1293 community-dwelling Chinese participants recruited from Shanghai, China, who were aged at least 60 years (753 women; mean age: 72.0 ± 5.9 years). Dynapenia was defined as low-grip strength (<28.0 kg for males and <18.0 kg for females) but normal skeletal muscle index (≥7.0 kg/m2 for males and ≥5.7 kg/m2 for females). Abdominal obesity was determined according to waist circumference (≥90 cm for males and ≥85 cm for females), and PAD was diagnosed by an ankle-brachial index ≤ 0.9. Binary logistic regression models were performed to determine associations between dynapenia, abdominal obesity, and the combination of dynapenia and abdominal obesity and PAD. According to dynapenia and abdominal obesity status stratified by age (60-74 or over 75), the patients were divided into 4 groups: normal, dynapenia alone, abdominal obesity alone, and co-occurring groups. A logistic regression showed that the co-occurring groups (odds ratio = 4.63, 95% confidence interval = 1.41-15.21) had a higher prevalence of PAD than the normal group after adjusting for the covariates in older adults over 75 years of age. The combination of dynapenia and abdominal obesity increase the prevalence of PAD in older adults over 75 years. The present findings have important implications for the early identification of older adults with PAD and appropriate interventions should be implemented.
Introduction
Peripheral artery disease (PAD) is an atherosclerotic disease of the arteries supplying the legs and is the third leading cause of atherosclerotic morbidity. 1 PAD affects approximately 238 million people worldwide, and the prevalence in people 60 years or older is 2.8% to 15.3% in China.1,2 The most severe symptoms of PAD can lead to amputations and increase the morbidity and mortality of cardiovascular disease. 3 Therefore, more attention should be paid to PAD. Studies have shown that both dynapenia and abdominal obesity are associated with poor cardiovascular outcomes.4,5 Thus, dynapenia and abdominal obesity may be related to the prevalence of PAD.
PAD is commonly accompanied by musculoskeletal abnormalities such as generalized loss of skeletal muscle mass and strength. 6 However, muscle strength decreases significantly faster than muscle mass and has a better prognostic value in predicting health-related outcomes. 7 Low muscle strength without low muscle mass is defined as dynapenia. 8 It is unclear whether dynapenia is related to PAD. Low muscle weakness is associated with peripheral arterial disease9,10 or only occurs in the lower extremities. 11 Notably, this age-related decrease in muscle strength is accompanied by redistribution of body fat, subcutaneous fat decreases, abdominal obesity, and ectopic fat increases. 12 It is especially essential to distingguish the relationship between muscle strength and fat infiltration.
According to research, 44% of patients with PAD suffer from abdominal obesity. 13 What's more, abdominal obesity has been highlighted as a worse condition than overall obesity, given that excessive intra-abdominal fat accumulation has better predictive value. 7 At present, several studies have analyzed the relationship between abdominal obesity and PAD, and they have reported conflicting findings. Several studies have shown that abdominal obesity is associated with PAD.14–16 However, other studies found that this connection only exists among women 17 and even has no correlation. 18 Therefore, the relationship between abdominal obesity and PAD is unclear and needs further research.
Muscle fat infiltration is an important part of low muscle strength, and abdominal obesity can reduce muscle strength through inflammation and endocrine mechanisms. 12 It is known that the coexistence of dynapenia and abdominal obesity has an impact on walking speed, falling, activities of daily living, disability, and death. 19 Therefore, we have reason to believe that dynapenia and abdominal obesity have additive effects, adversely affecting PAD. Generally, the young-old are active and their functional capacity remains relatively unchanged, while the old-old tend to be disabled and dependent. 20 Longitudinal studies have shown that, at age 75, muscle strength decreases at rates of 3% to 4% and 2.5% to 3% per year for men and women, respectively. 21 Notably, total body fat increases with age but decreases in adipose tissue at a later age. 22 Moreover, older age is one of the strongest risk factors for PAD and the prevalence of PAD more than doubled after age 75 in our latest study. 23 At present, the relationship between PAD and dynapenia and abdominal obesity is not clear, age may be an important factor in the correlation between the three. To distinguish the physical characteristics of the elderly in different age groups in order to better prevent the occurrence of PAD. Therefore, the purpose of our study was to evaluate the association between dynapenia and abdominal obesity with prevalent PAD in elderly individuals of different ages (60-74 and over 75 years old).
Methods
Study Participants
Participants in our study were recruited from Chongming District of Shanghai, China, who joined China's national free physical examination program from March 2019 to September 2020. The inclusion criteria for participants were age at least 60 years and completion of the relevant tests. Exclusion criteria were as follows: (1) participants who were unable to undergo ankle-brachial index (ABI) test; (2) amputation patients; (3) lack of waist circumference (WC) information; (4) inability to perform the grip strength test; (5) unable or refused to complete the body composition test; (6) people unable to communicate due to severe hearing impairment; or (7) incomplete questionnaire information. Those participants whose ABI (n = 26), amputation (n = 1), WC (n = 27), grip strength test (n = 8), skeletal muscle index (SMI) (n = 91), or questionnaires (n = 27) were incomplete were excluded, and the final analysis included 1293 participants (Figure 1). All individuals have been thoroughly knowledgeable on the nature of the research and signed an informed consent form to participate.

Flow diagram of the study.
Diagnosis of PAD
ABI (the ratio of ankle systolic blood pressure to brachial systolic blood pressure) is the first-line noninvasive diagnostic method for PAD. 1 The value was determined using the OMRON BP-203RPEII (Kyoto, Japan), which robotically and concurrently measures blood pressures in both arms and ankles. The systolic and diastolic pressures of the upper and lower extremities were obtained by calculating the average of the systolic and diastolic pressures of the right and left side of the arm and ankle. Using the higher value of the right or left brachial systolic blood pressure as the denominator, the ABI was calculated for the right and left limbs. Comparing the right and left ABI data, the lower of the two numbers was used for the study, and an ABI ≤0.9 was considered PAD. 1
Definition of Dynapenia
Dynapenia was defined as participants with low grip strength but normal SMI. 24 Grip strength (kg) was quantified using a dynamometer (GRIP-D; Takei Ltd, Niigata, Japan). Participants have been requested to exert their most effort twice the usage of their dominant hand and the average grip strength used to be recorded. 25 SMI was defined as a relative skeletal muscle mass index, which is a ratio of appendicular skeletal muscle mass (ASM) to height (Ht)2. ASM values were obtained using a bioelectrical impedance analyzer (InBody 770; Biospace, Seoul, Korea). According to the sarcopenia definition by the Asian Working Group for Sarcopenia 2019, 26 low grip strength was defined as <28.0 kg for males and <18.0 kg for females; normal SMI was defined as ≥7.0 kg/m2 for males and ≥5.7 kg/m2 for females.
Definition of Abdominal Obesity
WC was measured by a trained evaluator with a flexible tape placed at the nearest 0.1 cm at the umbilical level. Participants have been recommended to stand with their arms beside their body and take measurements at the cease of the expiratory segment of the respiratory cycle. Abdominal obesity was defined as waist circumference ≥90 cm for males and ≥85 cm for females. 27
Covariates
We collected data related to sociodemographic variables and behavioral characteristics, including age, sex, marital status, living condition, educational level, smoking and drinking. Physical activity levels were assessed through the short form of the International Physical Activity Questionnaire (IPAQ). 28 The Mini Nutrition Assessment-Short Form (MNA-SF) were used to assess nutritional status. 29 Calculation of gait speed using 4 m walking test, the specific test method was mentioned in our previous study. 23 Body fat percentage (BF%) and lean body mass were measured by bioelectrical impedance analyzer (InBody 770; Biospace, Seoul, Korea). Blood samples were taken from the participants’ peripheral veins in the morning after fasting for 10 to 12 h. The tests included triglyceride, high-density lipoprotein cholesterol levels, and serum creatinine, using an automated analyzer. 30 The diagnosis of chronic kidney diseases (CKD) is based on the estimated glomerular filtration rate, as described in our previous study. 23 The prevalence of specific medical conditions about hypertension, hyperlipidemia, diabetes, coronary heart disease, stroke, and osteoarthritis was established using standardized criteria. Subject physical sickness data were assessed based on participants’ answers to questions (yes or no), health practitioner diagnosis, and taking corresponding medicine or undergoing other treatment now or in the past.
Statistics
Compared with young-old people, the body of old people gradually loses independence, and the prevalence of PAD increases significantly after age 75. 20 Age-based exploration can provide a theoretical basis for clinicians to guide the rehabilitation training of the elderly in different age groups. Therefore, according to dynapenia and abdominal obesity status stratified by age (60-74 and over 75), the patients were divided into 4 groups: normal, dynapenia alone, abdominal obesity alone, and co-occurring groups. All continuous variables were expressed as the mean ± SD, and categorical variables were presented as percentages. Logistic regression analysis was used to estimate the odds ratio (OR) and 95% confidence intervals (CI) of dynapenia alone, abdominal obesity alone, and both to assess the additive effects of dynapenia and abdominal obesity on the prevalence of PAD. Participants with neither dynapenia nor abdominal obesity served as the reference group. The final model adjusted for age, sex, BF%, smoking, drinking, hypertension, hyperlipidemia, diabetes, CKD, IPAQ, and MNA-SF. All statistical analyses were performed using SPSS version 26.0 software (SPSS Institute Inc., Chicago, IL, USA), and P value <.05 were considered significance level in the study.
Results
The final sample comprised 1293 study participants (753 women; mean age: 72.0 ± 5.9 years). The baseline characteristics according to abdominal obesity and dynapenia status stratified by age are displayed in Tables 1 and 2.
Basic Characteristics According to Categories of the Prevalence of Dynapenia and Abdominal Obesity (60-74 Years).

P < .05 versus normal.
P < .05 versus dynapenia alone.
P < .05 versus abdominal obesity alone.
Abbreviations: ABI, ankle-brachial index; BMI, body mass index; BF%, body fat percentage; CKD, chronic kidney diseases; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; IPAQ, international physical activity questionnaire; LBM, lean body mass; LDL-C, low-density lipoprotein cholesterol; MET-min/wk, metabolic equivalent task minutes per week; MNA-SF, Mini Nutritional Assessment-Short Form; SBP, systolic blood pressure; SMI, skeletal muscle mass index; TCH, total cholesterol; TG, triglyceride; WC, waist circumference.
Basic Characteristics According to Categories of the Prevalence of Dynapenia and Abdominal Obesity (Over 75 Years).

P < .05 versus normal.
P < .05 versus dynapenia alone.
P < .05 versus abdominal obesity alone.
Abbreviations: ABI, ankle-brachial index; BMI, body mass index; BF%, body fat percentage; CKD, chronic kidney diseases; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; IPAQ, international physical activity questionnaire; LBM, lean body mass; LDL-C, low-density lipoprotein cholesterol; MET-min/wk, metabolic equivalent task minutes per week; MNA-SF, Mini Nutritional Assessment-Short Form; SBP, systolic blood pressure; SMI, skeletal muscle mass index; TCH, total cholesterol; TG, triglyceride; WC, waist circumference.
In the age group from 60 to 74, the co-occurring group of participants had more females and widows; higher body mass index (BMI) and WC; lower grip strength, gait speed, IPAQ, and MNA-SF scores; and higher prevalence of cardiovascular disease and CKD (Table 1).
In the group over 75 years, the co-occurring group had lower grip strength, gait speed, IPAQ, and more widows and living alone elderly individuals as well as lower levels of education than the group of participants aged 60 to 74 years (Table 2).
The prevalence of PAD in the general population was 8.3% (5.1% in 60-74 years, 15.6% in over 75 years). In participants over 75 years old, the prevalence of PAD in the 4 groups was 12.3% (n = 16), 16.7% (n = 5), 11.2% (n = 13), and 23.9% (n = 26) in the normal, dynapenia alone, abdominal obesity alone, and co-occurring groups, respectively (Figure 2). There is no significant association of dynapenia or abdominal obesity on prevalent PAD among all participants (P = .270). The combination of dynapenia and abdominal obesity was associated with PAD only in those over 75 years of age, rather than 60 to 74 years. Compared with the other groups, the co-occurring group had a significantly increased prevalence of PAD (P < .05) in over 75 years (Table 3). After adjustments for potential confounders, the following groups were associated with PAD prevalence: dynapenia alone (OR = 1.78, 95% CI = 0.48-6.55), abdominal obesity alone (OR = 1.58, 95% CI = 0.49-5.15), and co-occurring (OR = 4.63, 95% CI = 1.41-15.21).
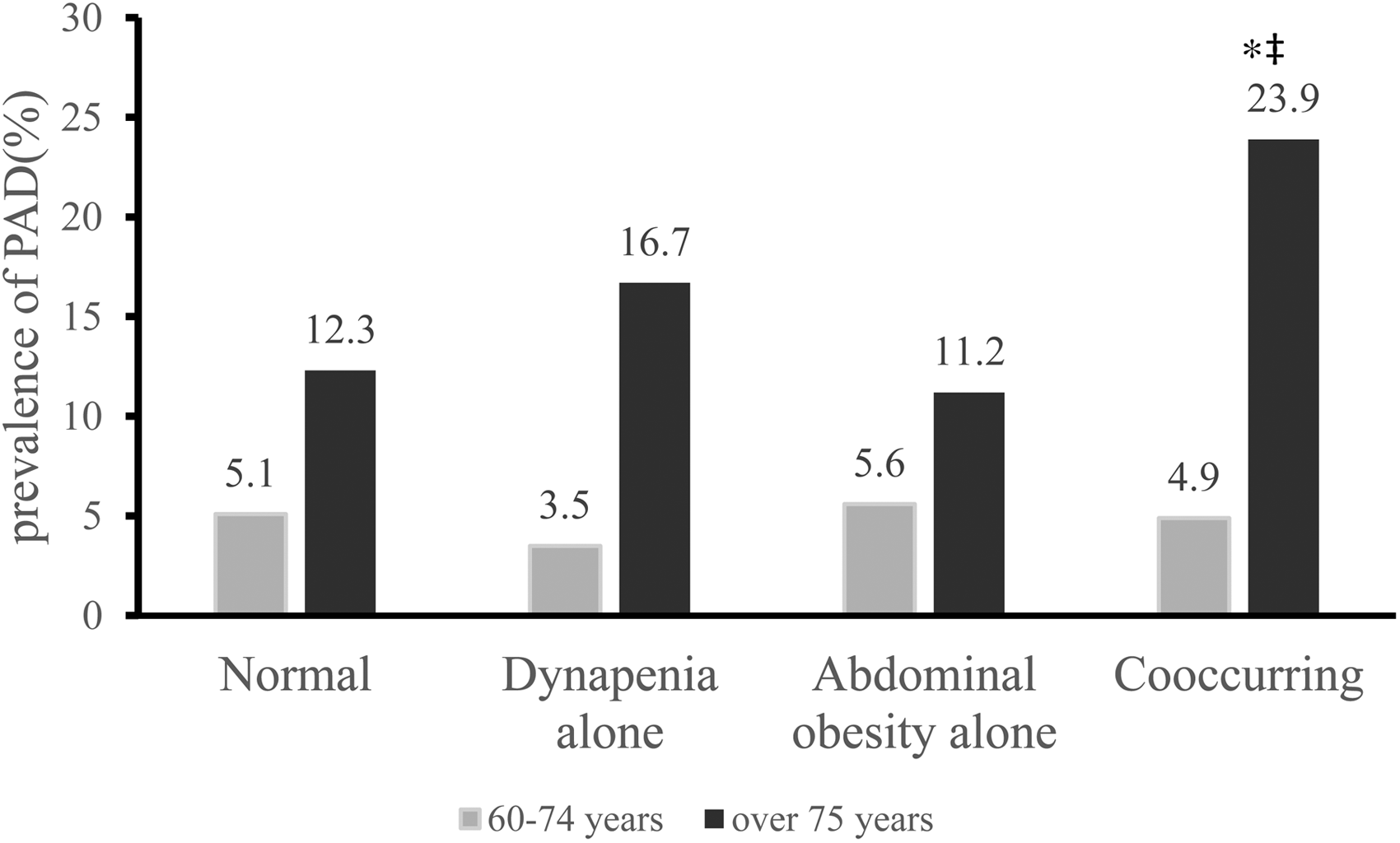
Difference of prevalence of PAD among different groups. *P < .05 versus normal; ‡ P < .05 versus abdominal obesity alone. Abbreviation: PAD, peripheral artery disease.
Association of Co-occurring Dynapenia and Abdominal Obesity With PAD.
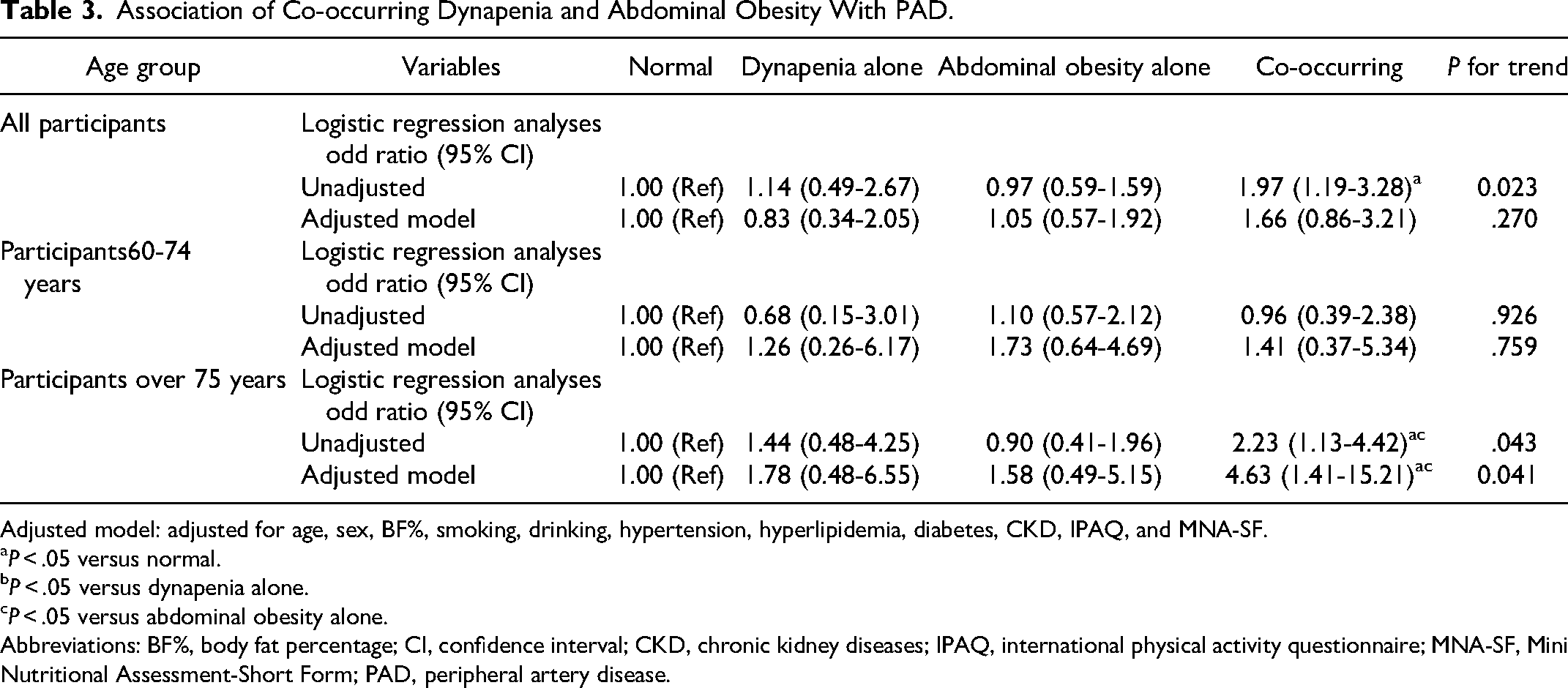
Adjusted model: adjusted for age, sex, BF%, smoking, drinking, hypertension, hyperlipidemia, diabetes, CKD, IPAQ, and MNA-SF.
P < .05 versus normal.
P < .05 versus dynapenia alone.
P < .05 versus abdominal obesity alone.
Abbreviations: BF%, body fat percentage; CI, confidence interval; CKD, chronic kidney diseases; IPAQ, international physical activity questionnaire; MNA-SF, Mini Nutritional Assessment-Short Form; PAD, peripheral artery disease.
Discussion
To our knowledge, this is the first study to show the joint effects of dynapenia and abdominal obesity on PAD prevalence among suburban-dwelling older adults in China. Those participants who suffered from both dynapenia and abdominal obesity had the highest prevalence of PAD (23.9%, P = 0.038) in the over 75 years group. In the adjusted model, neither dynapenia alone nor abdominal obesity alone or the combination of dynapenia with abdominal obesity were significantly associated with PAD in the general population or in the 60 to 74 age group. Our study found an association with PAD only in the combined group of dynapenia and abdominal obesity over the age of 75 years.
In our study, the overall prevalence of PAD is 8.3%, which is similar to a large Chinese population-based cross-sectional study, the China Hypertension Survey, which showed a PAD prevalence of 6.6%. 31 In addition, as with any atherosclerotic disease, older age is one of the strongest risk factors for PAD. 32 Our research also confirmed this, reaching 15.6% in the age group over 75 years old. This rate is similar to that in a Turkish study, in which the prevalence of PAD was 16.1% in the oldest group (over 75 years old). 15
The loss of muscle mass caused by disuse can only explain <10% of muscle strength decline. 33 Therefore, dynapenia should be considered separately from decreased muscle mass. A previous study that lower extremity ischemia is related with poorer distal lower extremity strength but not upper extremity strength, which suggests that there can also be larger global weakness in participants with PAD that influences upper and lower extremity strength. 11 In contrast, Matsushita et al found independent associations of lower ABI with lower grip strength and this association was independent of other cardiovascular subtypes, suggesting the involvement of systemic pathophysiology. Because a low ABI is an indicator of systemic atherosclerosis, people with a low ABI usually have other cardiovascular manifestations that may additionally lead to worse systemic physical function. However, the conceivable pathophysiological mechanisms of PAD related to the decline in muscle strength need further research. 10 Of note, dynapenia alone was not associated with the prevalence of PAD. One cause for the variations in these outcomes might also be due to the small number of individuals in the dynapenia alone group, since the co-occurring group also included people with dynapenia. When we included participants in the co-occurring group in the dynapenia group, the relationship with PAD became statistically significant (OR = 3.02, 95% CI = 1.10-8.29, P = .032) in the age group over 75 years old.
On the other hand, we found that abdominal obesity alone was not associated with the prevalence of PAD. Similar to our study, a previous study found that peri-aortic fat and not WC, BMI, or visceral abdominal fat was associated with PAD, which may be perivascular adipocytes contributing to adventitial inflammation and in turn the development of atherosclerosis. 18 However, some studies conflicts with ours. Research has shown that, in patients with hemodialysis, abdominal obesity, and not BMI, is associated with a 4-fold risk of developing PAD (OR = 4.532, 95% CI = 1.765-11.639). 14 Moreover, a study from Atherosclerosis Risk in Communities found that WC tends to be more strongly associated with PAD with critical limb ischemia than with PAD without critical limb ischemia. Adipose tissue has been related with elevated levels of pro-inflammatory cytokines, and those with PAD with critical limb ischemia have higher circulating levels of inflammatory markers causing the difference in the association strength. 16 Another study showed that WC was not a predictor of PAD in men but was in women. 17 One of the reasons for the variations in the results of these research may be the different population characteristics of the research samples. The specific cause is unclear, and future longitudinal research are wished to in addition look into the relationship between belly weight problems and PAD.
Of note, the most interesting finding in our study was that dynapenia combined with abdominal obesity increases the prevalence of PAD in older adults over 75 years old (OR = 4.63, 95% CI = 1.41-15.21). One viable underlying mechanism to give an explanation for our outcomes is that dynapenia and abdominal obesity may also generate additive effects. Previous studies have reported that high WC is associated with lower grip strength, and for every 10 cm increase in WC, grip strength declined 3.56 kg for men and 1.00 kg for women. 34 Therefore, abdominal obesity could negatively affect muscle strength. First, we found that both grip strength (20.85 ± 8.45 kg vs 25.18 ± 9.04 kg, P<.001) and gait speed (0.94 ± 0.26 m/s vs 1.13 ± 0.22 m/s, P < .001) were lower in the over 75 years group than in the 60 to 74 years group. What's more, in over 75 years group, individuals who suffered from both dynapenia and abdominal obesity typically had a lower gait speed (0.85 ± 0.24 m/s vs 1.02 ± 0.25 m/s,P < .001) than normal people. Low muscle strength and low grip speed represent poorer physical function in older adults, which significantly associated with the occurrence of cardiovascular events including PAD. 35 In turn, reduced muscle perfusion from PAD also accelerates muscle atrophy leading to decreased muscle function. 36 Both dynapenia and abdominal obesity are age related, and the cumulative effects of dynapenia and abdominal obesity may be more pronounced with age. During the ageing process, adipose inflammation leads to redistribution of fat into the abdomen and fat penetration into skeletal muscle, leading to a decrease in overall strength and function resulting in lipotoxicity, insulin resistance, and increased secretion of a range of pro-inflammatory cytokines. 37 In turn, muscle-secreted cytokines may exacerbate adipose tissue atrophy, cause chronic low-grade inflammation, and establish a vicious cycle of local hyperlipidemia, insulin resistance, and inflammation. 38 Inflammation increases vascular endothelial damage becoming an important risk marker of systemic atherosclerosis and has been associated with the development of PAD. 32 In the future, testing myokines and adipokines in blood samples from participants will contribute to verify the connection between dynapenia and abdominal obesity and PAD, which may further find the potential markers of this association. What's more, insulin resistance promotes vasoconstriction through the increased production of vasoconstrictor factors such as endothelin and/or pathological vascular stiffening, which promotes the development of atherosclerosis. 39 Therefore, dynapenia and abdominal obesity may have additive effects, adversely affecting PAD. This may help explain why our results showed an increased prevalence of PAD in the co-occurring group only in the age group over 75 years. Of note, PAD frequently accompanied by atherosclerosis in other vascular beds exhibits more serious adverse consequences. 40 Therefore, in view of the current lack of awareness and diagnosis of PAD, improving awareness, detection, and management of PAD in the future will help with the early detection of diseases that pose a threat to the health of elderly. This will encourage early interventions to avoid the occurrence of adverse and serious consequences.
Strengths and Limitations
The strength of this study is that it is the first to report the combined effect of dynapenia and abdominal obesity on the prevalence of PAD among the elderly individuals of different ages. However, there have some limitations that still exist in our study. Firstly, our research was a cross-sectional study, therefore, it was difficult to determine the causal relationship between them. Second, our study participants were asymptomatic PAD, we did not describe the severity of PAD, therefore, we cannot make conclusions on the effect of the combination of dynapenia and abdominal obesity on the severity of PAD symptoms. Third, we lack information about the lower body fat mass and fatty liver, because lower body fat mass can independently affect the cardiometabolic risk. 41 What's more, fatty liver, disproportionate fat mass and diabetes strongly interact with each other to determine the risk of atherosclerosis. 42 Fourth, our female participants rarely used hormones, which may be related to the lack of attention to hormone therapy among Chinese females, as most postmenopausal Chinese females lack knowledge of hormone therapy and their hormone therapy use is low compared to developed countries. 43 We will further explore the effect of hormone use on PAD in the future study. Fifth, to study the effect of dynapenia and abdominal obesity on PAD among different sexes in different age groups is also a worthy direction for future research, and we will further expand the sample size and conduct further studies in the future. Sixth, the health status of participants in our study was relatively good because we did not include elderly individuals who were unable to participate in the free annual national physical examination (eg, those who were bedridden or had serious disease). Finally, we should note that because this study was conducted in Shanghai, China, it may not represent results in other parts of the country. Therefore, extrapolation of conclusions should be done with caution. We will assess the validity of our method by using more datasets in the future.
Conclusions
In conclusion, our study showed that individuals who suffered from both dynapenia and abdominal obesity had a significantly higher prevalence of PAD among community-dwelling individuals over 75 years old, after adjusting for confounding factors. This suggests that measures should be taken in participants to prevent the prevalence of PAD, thereby reducing poor outcomes in older adults to extend healthy lifespan expectancy.
Footnotes
Acknowledgments
All the authors would like to thank Peijuan Jin and Xiaoyue Gu from the Chongming public health center for providing place and organization.
Author Contributions
YuZ and XC conceived the concept and design of the study. PH, CX, HY, WZ, RW, YiZ, and YiS contributed to data collection, data entry, and data cleaning. YaZ, ZZ, and ML contributed to the data analysis and interpretation of the study results. YuZ, YuS and ZZ drafted the article or revised it critically for important intellectual content. QG provided administrative support and contributed to the acquisition of funding. All authors have approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
The research involving human participants were reviewed and approved by the Ethics Committee of Shanghai University of Medicine and Health Sciences. The participants provided their written knowledgeable consent to take part in this study. The research method was in line with the principles of Helsinki declaration.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the funding of Capacity Building project of Local Colleges of Shanghai Science and Technology Commission (23010502800), National Natural Science Foundation of China (82172552) and Scientific Research Foundation of SUMHS (SSF-21-03-005).