
Abstract
Introduction
A prospective, randomized, multicenter study compared rivaroxaban 2.5 mg twice daily plus aspirin 100 mg once daily against aspirin 100 mg once daily alone in patients with peripheral artery disease and intermittent claudication. The study demonstrated that rivaroxaban plus aspirin improved total walking distance. A better comprehension of coagulation and inflammatory biomarkers could serve as a prognostic indicator and inform clinical decision-making.
Methods
This is a subsequent biomarker analysis, including 36 patients from both arms and plasma from healthy controls. We used human plasma for comparison purposes of the baseline biomarkers for normality testing. Plasma levels of biomarkers relating to coagulation activation (DD, vWF, thrombin generation potential (TGP), fibrinolysis (PAI-1, TAFI) and inflammation (CRP) were assessed at baseline (day 0) and measured after 24 weeks.
Results
Samples from 16 patients allocated to the aspirin plus rivaroxaban group and 20 from the aspirin alone group were collected. No significant differences were observed in biomarkers between patients receiving rivaroxaban plus aspirin and those receiving aspirin alone.
Conclusion
There were no differences in coagulation or inflammatory biomarkers in patients with intermittent claudication treated with either rivaroxaban plus aspirin or aspirin alone.
Introduction
Peripheral arterial disease is now the preferred term denoting partial or complete obstruction of peripheral arteries and stands as one of the most prevalent manifestations of atherosclerosis. It's one component of atherosclerotic cardiovascular disease that impacts 27 million individuals in Europe and North America, with an additional 15 million in Latin America. 1 Intermittent claudication manifests as leg pain triggered by walking and alleviated by rest. It typically indicates ischemic pain provoked by physical exertion, especially in the calf. This condition significantly diminishes the quality of life and cardiovascular health and hampers mobility. 2
The effectiveness of treatments available for patients with intermittent claudication, including supervised exercise, drug therapy, and revascularization (either via surgical bypass or endovascular interventions), remains poorly established and yields inconsistent results. 3
The COMPASS trial demonstrated that rivaroxaban 2.5 mg orally twice daily plus aspirin in comparison to aspirin alone led to a significant decrease in major adverse cardiovascular events and major adverse limb events, resulting in a relative risk reduction (RRR) of approximately 59% of amputations. 4 With only cilostazol and pentoxifylline currently formally approved, there is a pressing need for new therapies that enhance mobility and promote independent living for PAD patients. New therapies must undergo rigorous evaluation.5,6 New biomarkers may facilitate earlier screening and detection, as well as potentially control of disease progression, leading to the development of new therapeutic approaches. 7
The COMPASS CLAUDICATION trial was a prospective, randomized, open-label, multicentre study, which assessed the use of a vascular dose of rivaroxaban (2.5 mg twice daily) plus aspirin 100 mg once daily in comparison to aspirin 100 mg once daily in patients with intermittent claudication. The trial demonstrated that rivaroxaban plus aspirin improved total walking distance compared to aspirin alone. 7 This current study is a pre-specified subsequent biomarker analysis.
Methods
Study Design and Patient Enrolment
This is a secondary analysis of the COMPASS CLAUDICATION trial (ClinicalTrials.gov Identifier: NCT04853719), focusing on biomarker variations of the two experimental groups (rivaroxaban plus aspirin and aspirin alone) and a control group of healthy individuals.
This study adhered to the principles of the Helsinki Declaration and received approval from the Ethics Committee of every participating institution under protocol numbers 40190420.0.1001.5485. Before participation, all patients signed the informed consent form.
Patient recruitment with intermittent claudication occurred between February and December 2022. The key inclusion criteria were adult patients (age ≥ 18) with symptomatic PAD who signed the informed consent form (ICF) were eligible for the COMPASS claudication trial if they had an Ankle-brachial index (ABI) < 0. 85 and absolute claudication distance (ACD) < 500 m, no history of lower-limbs arterial bypass surgery or angioplasties in the last year, walking ability limited by the symptom of claudication and the ability to complete a treadmill test. The key exclusion criteria were high risk of bleeding (bleeding in the last three months, hemorrhagic diathesis, abnormal blood coagulation (eg, INR > 1.5, aPTT ratio > 2), pulmonary bronchiectasis, active cancer, active gastroduodenal ulcer, use of dual antiplatelet therapy). Recent hemorrhagic stroke (within 1 month) or any history of previous hemorrhagic or lacunar stroke, if detected by occasional prior tomography, which is not part of the study protocol. Severe heart failure (NYHA class III and IV, advanced stable kidney disease (estimated creatinine clearance <15 ml per minute), defined as eGFR < 15 mL/min by 1.73 m2 calculated by the abbreviated formula Diet Modification in Kidney Disease (MDRD). Continuous use of pentoxifylline or cilostazol for cardiac conditions that may lead to heart failure, such as unstable angina, arrhythmias, and acute myocardial infarction in the last three months. The researcher considers non-cardiovascular conditions as associated with a poor prognosis (active cancer with a life expectancy of fewer than six months, collagen-limiting diseases, previous or scheduled surgeries that prevent functional evaluation, and orthopedic diseases that hinder functional evaluation). Pregnancy (women with the potential to bear children had to be under contraceptive strategies and take a negative pregnancy test to be enrolled). Patients with COVID in the contagious phase (PCR+) were also excluded.
The primary trial and functional results, is published elsewhere. 7
For this secondary biochemical analysis of 36 patients, a control group was included through analysis of healthy volunteers’ plasma purchased from the commercial supplier George King Biomedical, Inc. (Overland Park, KS, USA). Plasma analysis was conducted by the Haemostasis and Thrombosis Laboratory at Loyola University – Chicago – United States.
Hyphen Biomed provided the ELISA kit used in this study. Complete identification of the kit, including the manufacturer and reference number, was recorded to ensure traceability and transparency in the experimental process.
All data was recorded in a pre-established clinical record file (CRF).
Demographic and Clinical Data Collection
At baseline, demographic data was collected for all patients, including risk factors (smoking, sedentary lifestyle), clinical aspects of the patient's comorbidities, and quality of life (QoL) scores and in addition to collecting blood samples to evaluate biomarkers.
Serum Biomarker Collection
Serum biomarkers were collected on the day of diagnosis (baseline, D0) and after 24 weeks of treatment. Assessment included markers of:
- Coagulation activation: D-dimer (DD); von Willebrand Factor (vWF) and thrombin generation potential (TGP). - Fibrinolysis: Plasminogen Activator Inhibitor 1 (PAI-1) and Thrombin-activatable fibrinolysis inhibitor (TAFI) and - Inflammation: C-reactive protein. (CRP)
Blood samples were collected and appropriately stored for evaluation of DD, vWF, PCR, TAFI, TGP and PAI-1.
All blood collections and laboratory analyses were conducted following the Haemostasis & Thrombosis Research Laboratories guidelines at Loyola University. The frozen samples were shipped on dry ice and delivered to their destination within 24 to 48 h at the laboratory partner of this research.
Plasma levels of several biomarkers analyzed in this study were assessed using commercially available enzyme-linked immunosorbent assays (ELISA). The biomarkers assessed were from HYPHEN BioMed (Neuville du Oise, France). The closed kit protocol was followed for all biomarker assays conducted. Details on the kits used as follow: Anti-Xa: BioMedica Diagnostics Spectrozyme FXa Lot 211004 Ref 222 Exp. 2023-04-30, Bovine Factor Xa Enzyme Research Lot BFA 1822 Exp. 01/2022. Tris Buffer NaCl EDTA pH 8.4. Thrombin Generation: Diagnostica Stago.Thrombin Calibrator: Lot TC2002/01 Ref 86192 Exp. 2/15/24. Fluco-Buffer: Lot FLB2107/01 Ref 86197 Exp. 7/25/23. Fluco-Substrate: Lot FLS2107/01 Ref 86197 Exp. 7/7/23Thrombinoscope PPP Reagent High: Lot: PPH1902/01 Ref TS32.00 Exp. 2/12/21. DI Water: Lot 2276746 Ref 15230-147 Exp. 4/30/23. Water Bath 37 °C SN: 10BA-590 CAT NO: 66800 Precision Scientific. Fluoroskan Ascent Hemker Thrombinoscope SN 374-2697 Serial RS-2232 C. REF: 5210581 Diagnostica Stago Thermo Electron Corporation.
Citrated plasma controls were obtained from healthy volunteers without comorbidities through a commercial supplier, George King Biomedical, Inc., based in Overland Park, Kansas, USA.
Randomization
Randomization was carried out using an electronic form through our CRF registered on the Redcap platform, and no paired randomization was carried out for the biomarkers. Through statistical analysis that defined n = 9 for each group, we used the first patients who completed the sampling, who were included in a group of 36, where the rivaroxaban plus aspirin group (N = 16) and aspirin alone group (n = 20).
Statistical Analysis
Results were analyzed as median as mean and interquartile range (75%-25%)/2 as standard deviations (SD) with evolution scenarios at 5%, 10%, 15%, and 20%. The intra-evolution evaluation (gain within each group) was done using a paired t-test. The inter-evolution evaluation (gain between groups) was evaluated using the t-Student. All analyses were conducted with a significance level of 5% and a test power of 80%.
All statistical analyses were conducted using the SPSS software, version 25.0. Given the small sample sizes, non-parametric tests were utilized for data analysis, with a significance level set at P < .05. Significant data were represented using boxplots.
Results
Thirty-six patients (16 from the rivaroxaban plus aspirins and 20 patients from the aspirin alone group) and plasma from a pool of healthy volunteers were included. They were the first 36 from the original sample of 88 patients from the main trial. Plasma levels of biomarkers were measured at baseline and after 24 weeks of treatment.
In the study diagram, we had the evaluation of 766 patients, who after inclusion and exclusion criteria, we reached the final number of 88 patients included, of which 88, the first 36 to complete the study were used for the analysis of biomarkers- the CONSORT diagram of the original study sample is presented in Figure 1.

The CONSORT Diagram.
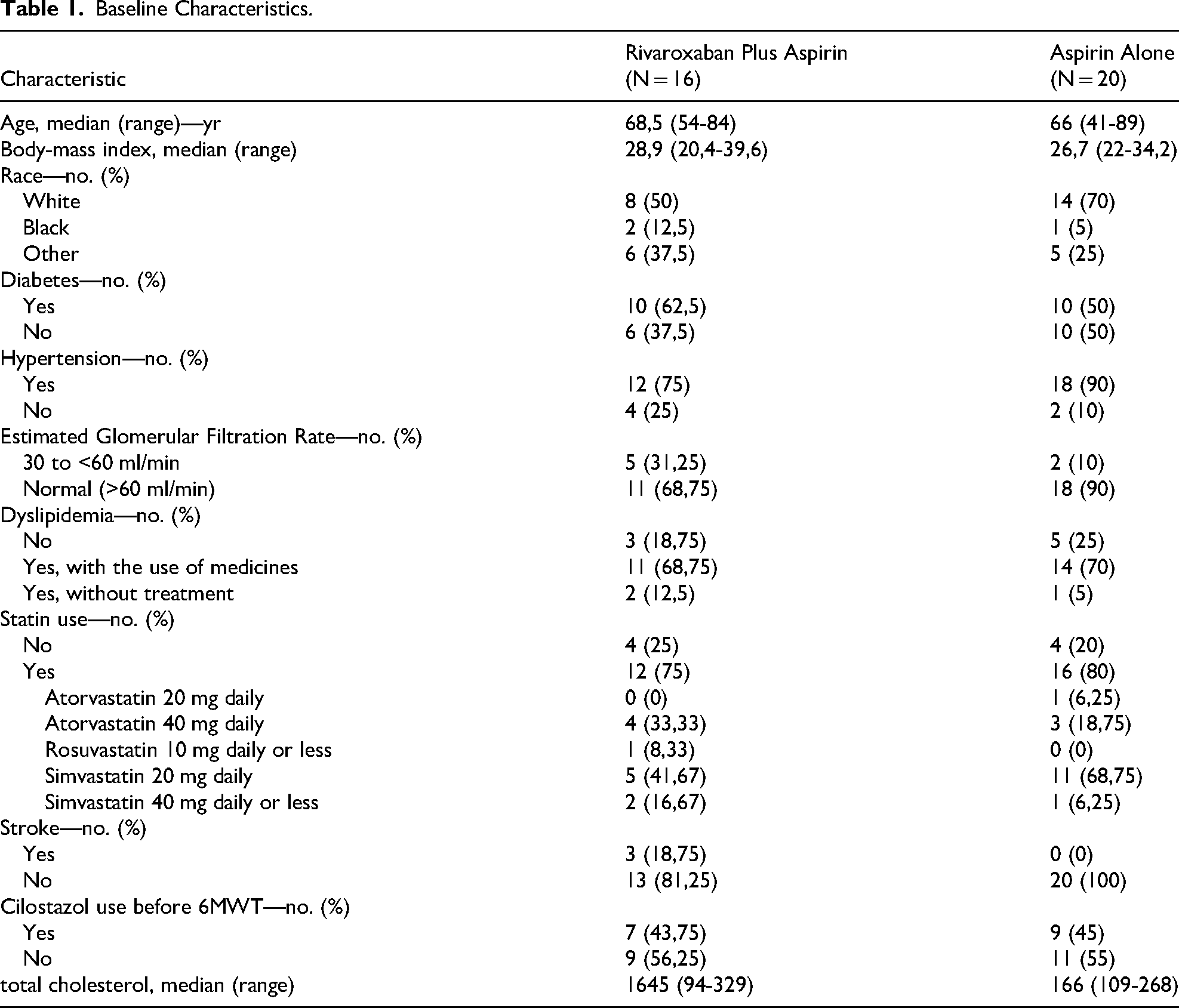
We had 16 patients allocated to the aspirin plus rivaroxaban group and 20 to the aspirin alone group – of these, an average age of 68.5 years and 66 years, respectively. In the aspirin plus rivaroxaban group, the majority were diabetic, unlike the aspirin group, where it was 50%. This was different from hypertension, which was prevalent in both groups. And both groups had high cholesterol levels – patient demographic and clinical characteristics are detailed in Table 1. Groups were homogeneous with regard to these findings.
Baseline Characteristics.
The biomarkers did not show significant variations at baseline or at the end of the evaluations (24 weeks), in the observation measurements of the values, which can be seen in Tables 2 and 3, respectively and in Figures 2 and 3.

Intergroup Statistical Evaluation of Biomarker Variations at Baseline and 24 Weeks Using the Shapiro-Wilk Test in the Aspirin and Rivaroxaban with Aspirin Groups.

Boxplot of Thrombin Levels in the Rivaroxaban and Aspirin Intragroup at Baseline, 12 and 24 Weeks.
Analysis of the Baseline in Control Groups of Healthy Patients, Aspirin Alone Group and Rivaroxaban Plus Aspirin Group Using the Kruskal-Wallis Test. Analysis of Aspirin Alone Group and Rivaroxaban Plus Aspirin Versus Control Using the Shapiro-Wilk Test.

Biomarker serum Concentrations at Week 24 in the Aspirin and Rivaroxaban Plus Aspirin Groups.

When trying to find statistical relevance between groups to assess whether there were changes that could predict any biomarker as a prognostic factor, we were also unable to identify any. We used the Shapiro Wilk and Mann-Whitney tests, but without statistical relevance (Table 4).
Analysis of Intragroup Variation (Aspirin Alone vs Rivaroxaban Plus Aspirin Groups) Using the Shapiro-Wilk Test. Analysis of Intragroup Variation (Aspirin Alone vs Rivaroxaban Plus Aspirin Groups) Using the Mann-Whitney Test.

There was, nevertheless, a non-statistically significant tendency for a decrease in TGP biomarkers in the Rivaroxaban plus Aspirin group (Table 3).
Discussion
Through this inflammatory process, biomarkers can be identified to predict or indicate the presence of this process with predictive value. For example, they extensively cited CRP and suggested the potential involvement of interleukins and even TNF alpha. The primary aim of this study was to evaluate the presence of such biomarkers in peripheral artery disease manifesting with intermittent claudication, potentially helping identify target therapies and targeted clinical use, aiming for clinical improvement. 8
There was an increase in inflammatory biomarkers in patients with peripheral artery disease compared normal ranges and there were no differences between rivaroxaban plus aspirin and aspirin alone. Therefore, biomarkers analyses did not help in the understanding of the mechanism for which rivaroxaban plus aspirin improve walking distance in patients with PAD.
With an understanding of the endothelium and its biochemical expression, biomarkers such as PCR, DD, VWF, TGP, PAI-1 and TAFI were identified as biomarkers of interest.9-12
Additional markers, such as anti-factor Xa (anti-Xa), are being investigated in clinical practice as potential indicators for anticoagulant therapy, although their reliability has not yet been firmly established. 13
Our study focused on patients with claudication rather than those who meet critical limb ischemia criteria. The choice of assessed biomarkers was guided, focusing on those related to hemostasis, thrombotic formation and inflammation. Given this context, we recognize that the analysis of conventional biomarkers focused mainly on atherosclerosis may not be definitive, as our study population was receiving the vascular dose of rivaroxaban plus aspirin 100 mg once daily. Therefore, our study aimed to investigate inflammatory biomarkers, such as CRP, and biomarkers directly linked to the coagulation cascade, such as the product of TGP. 14
The COMPASS trial showed a significant reduction in both MACE and MALE. This reduction included a remarkable decrease in the relative risk of amputations by around 59%. Nevertheless, the mechanisms underlying the antithrombotic effects of this dose of rivaroxaban have yet to be fully elucidated. 15 This finding was further supported by the study by Narula et al in 2018, which demonstrated that thrombotic luminal occlusion might play a more significant role than isolated atherosclerosis, underscoring the potential benefits of anticoagulant therapies. The benefits of a biomarker-guided antithrombotic strategy are still unknown.16,17
The observed decrease in TGP can be coherently explained by administering the rivaroxaban dose. This finding aligns with previous data that associated higher blood viscosity and elevated fibrinogen levels with male and female patients presenting with intermittent claudication. 18
Potential reasons for the lack of significance in our results includes the small sample size and possible medication-related issues. Most of our patients were taking statins, as well as antidiabetic and antihypertensive drugs, and there are numerous studies reporting the variation of the biomarkers analyzed when using these drugs.19-21 This may be the reason for the variation identified that did not allow us to find a valid biomarker. For example, in patients with VTE and taking statins, the D-dimer values are statistically significantly lower. 22
The observed decrease in TGP can be coherently explained by administering the rivaroxaban dose. This finding aligns with previous data that associated higher blood viscosity and elevated fibrinogen levels with male and female patients presenting with intermittent claudication.
We were unable to define statistically significant biomarkers to serve as a prognostic factor, but the sustained drop in thrombin leads us to the hypothesis that a longer analysis time, in new studies, may define how this drop will occur and whether it will become statistically relevant. Associated with this finding, we see that many of the biomarkers already interact with other drugs that are already commonly used by patients with peripheral artery disease and intermittent claudication. 18
The current study has some limitations. This exploratory analysis was conducted with a small sample within a relatively short timeframe, which proved insufficient for the definition of a sustained response or identification of a biomarker with positive predictive value. We also did not evaluate specific markers for rivaroxaban as well as soluble platelet factor biomarkers.
Further studies are therefore warranted, ideally with more robust samples and extended duration to confirm this hypothesis.
Conclusion
In peripheral artery disease patients presenting with intermittent claudication, no significant variation in coagulation or inflammatory biomarkers was observed between baseline and after 24 weeks of treatment with rivaroxaban plus aspirin or aspirin alone.
Footnotes
Acknowledgment
This study was partially supported by the Cardiovascular Research Institute of Loyola University, Chicago, USA, and by Science Valley Research Institute, Santo André, São Paulo, Brazil. We appreciate the skillful assistance of Ms. Erin Healy-Erickson for her help in the preparation of this manuscript.
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bayer SA.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The COMPASS CLAUDICATION trial was investigator-initiated research with financial support from BAYER S.A. ER discloses research grants and consulting fees from Bayer, Novartis, and Pfizer, grants from the Brazilian Ministry of Science and Technology, and personal fees (educational) from Aché Pharma, Sanofi, and Daiichi Sankyo. SSA reports honoraria and consultancy fees from Bayer and Janssen. John Eikelboom has received honoraria and/ or research funding from Bayer, BI, BMS, DSI, Janssen, Merck, Pfizer, and Servier. RDL reports grants and personal fees from Bristol Myers Squibb, Pfizer, GlaxoSmithKline, Medtronic PLC, and Sanofi and personal fees from Amgen, Bayer, and Boehringer Ingelheim, outside of the submitted work. The remaining authors have no conflicts of interest to declare.