
Abstract
Persons with bleeding disorders (PwBD) are at high risk for bleeding with invasive procedures. However, the risk of bleeding in PwBD undergoing major surgery and outcomes of patients managed perioperatively at a hemophilia treatment center (HTC) are not well described. We performed a retrospective review of surgical outcomes among PwBD undergoing major surgery between January 1st, 2017 and December 31st, 2019 at the Cardeza Foundation Hemophilia and Thrombosis Center in Philadelphia, PA. The primary outcome was postoperative bleeding, assessed according to the ISTH-SSC's 2010 definition. Secondary outcomes included use of unplanned postoperative hemostatic therapy, LOS, and 30-day readmission rate. Results were compared to non-PwBD population from a surgical database, matched for surgery, age, and sex. During the study period, 50 PwBD underwent 63 major surgeries. The most common diagnoses were VWD (64%) and hemophilia A (20.0%). The most common surgical procedure category was orthopedic (33.3%), predominantly arthroplasties. Postoperatively,4.8% of procedures were complicated by major bleeding and 1.6% by non-major bleeding. The mean LOS was 1.65 days, and 30-day readmission rate was 1.6%. In comparison to matched, non-PwBD patients in a national surgical database undergoing the same procedures, study patients had a similar rate of bleeding complications per procedure (5.0% vs 1.04% P = .071, Fisher's exact test). PwBD undergoing major surgeries have low rates of major bleeding when receiving comprehensive care at an HTC. Bleeding and hospital readmission rates were similar to non-PwBD baseline in a large database.
Introduction
Persons with bleeding disorders (PwBD)—including von Willebrand disease (VWD), hemophilia A and B, and other congenital rare bleeding disorders (RBD)—are at increased risk for bleeding with invasive procedures.
VWD, due to either quantitative or qualitative defects in von Willebrand factor (VWF), is the most common congenital bleeding disorder, inherited more often in autosomal dominant fashion with reported prevalence ranging from 0.0023% to 0.01%. 1 VWF plays a critical role in primary hemostasis and stabilization of factor VIII (FVIII) in circulation, and defects most often result in a mucocutaneous bleeding phenotype,1,2 which can be provoked by surgical procedures. 3 Hemophilia A and B are X-linked congenital deficiencies of FVIII and FIX, respectively, that occur in 0.001% of the population, with hemophilia A accounting for 85% of cases. 4 Bleeding can range from spontaneous hemarthrosis and soft tissue bleeds in patients with severe deficiency to no spontaneous bleeding in patients with mild deficiency, but all are at risk for hemorrhage with invasive procedures or trauma.5–7 Finally, other RBDs—including deficiencies of fibrinogen (FI), prothrombin (FII), FV, FVII, FX, FXI, and FXIII—are rare, occurring in between one in 500,000-2 million people in the general population. 8 Patients with these disorders represent a wide spectrum of bleeding phenotypes, though many are at risk for bleeding with invasive procedures.9,10
In the era before discovery and routine use of factor replacement therapy, perioperative mortality was high in PwBD, with a series of reports finding mortality rates of 60% in hemophilia A patients prior to 1966 and 3-5% by 1980. 11 With mainstream availability of both plasma-derived and recombinant factor concentrates by the late 1990s, 12 PwBD have been able to undergo surgical procedures more safely. Prospective studies established the efficacy and safety of plasma-derived VWF-FVIII concentrates in VWD patients undergoing elective surgeries, with bleeding rates varying between 3.6% and 15.9%.13–15 Another study of emergent surgeries in VWD patients who received perioperative plasma-derived VWF-FVIII concentrate found that excellent or good hemostasis was achieved 100% of the time. 16 Finally, a recent summary of systematic reviews found bleeding rates of 0−5% among VWD patients undergoing major surgeries. 17 Retrospective studies have demonstrated the safety of endoscopic procedures in PwBD treated with perioperative hemostatic therapy.18,19 Others have examined outcomes in patients with hemophilia undergoing orthopedic surgery, as chronic hemarthopathy often necessitates eventual arthroplasty in these patients. Bleeding complications occur in approximately 9% of these patients,20,21 and infection and re-operation are also common complications.21–23 However, data on PwBD undergoing other major surgeries 24 in the modern factor replacement era is scant, with one study finding excellent outcomes of patients undergoing abdominal surgeries at a hemophilia treatment center (HTC) 25 and another showing a bleeding complication rate of 3.4% among VWD patients undergoing both minor and major surgeries who received perioperative VWF-FVIII concentrate. 26 Finally, a study of 160 elective surgeries in VWD patients found that for dental and other minor surgeries, DDAVP with or without tranexamic acid was effective. Notably, the authors observed that bleeding did not correlate with age-related increased VWF levels, as all patients who developed bleeding complications had levels >50 IU/dL. 27
Overall, numerous studies have confirmed the effectiveness of periprocedural hemostatic therapy for preventing bleeding in PwBD undergoing various surgical procedures.13–15,18,25,26,28,29 Recent guidelines support the use of factor replacement therapy before and after major surgery to mitigate bleeding risk.1,3,4 Furthermore, outcomes may be better among patients treated at an HTC, 30 where factor replacement therapy is available and multidisciplinary teams can put into place hemostatic plans for complex surgeries. 31
The objective of this study was to evaluate the outcomes of patients undergoing elective major surgeries at an academic HTC. We measured bleeding rates, hospital length of stay (LOS), and unexpected postoperative factor replacement therapy in our patient population, then compared bleeding rates and LOS to a control population of patients without bleeding disorders undergoing the same surgeries, using a large national surgical database of academic medical centers.
Methods
Study Design and Population
We performed a retrospective chart review to evaluate outcomes among PwBD at the Cardeza Hemophilia and Thrombosis Center, the HTC affiliated with Thomas Jefferson University in Philadelphia, PA, who underwent elective major surgery between January 1, 2017 and December 31, 2019. The study was approved by the Thomas Jefferson University Institutional Review Board. We included all patients seen at our HTC with diagnoses of hemophilia A or B, VWD, or RBD. The study included planned surgeries requiring general anesthesia for >30 minutes, as well as any orthopedic and neurologic surgery, and only those occurring at Thomas Jefferson University Hospitals were included, in order to ensure that all data elements could be captured. Only patients who had been seen by a physician at our HTC preoperatively were included.
The primary outcome was postoperative bleeding, assessed according to the International Society on Thrombosis and Haemostasis (ISTH) Scientific and Standardization Committee's (SSC) 2010 definition in surgical patients. 32 The ISTH-SSC defined major bleeding in surgical patients as any bleeding that was fatal or occurred in a critical organ; extrasurgical site bleeding resulting in a hemoglobin (Hgb) drop of at least 2 g/dL or that required transfusion of ≥2 units of red blood cells; or surgical site bleeding that required a second intervention to achieve hemostasis or that was unexpected and resulted in at least a 2-g/dL Hgb drop or transfusion of ≥2 units of red blood cells. Any other bleeding events not meeting these criteria were designated as minor bleeding. Secondary outcomes included any use of unplanned postoperative hemostatic therapies or doses beyond what was recommended by the treating physician, inpatient LOS, and 30-day hospital readmission rate.
Data Collection
Electronic health records for all eligible patients were reviewed to determine their qualifying diagnoses, which for hemophilia A and B were classified according to ISTH-SSC criteria 33 and for VWD according to type by ISTH definition 34 and severity by physician documentation. The most recent outpatient factor level for each patient was recorded, as was the planned perioperative hemostatic therapy recommendation, such that determinations could be made as to whether patients required additional unplanned therapy postoperatively. Demographic data included age at the time of surgery, sex, and race. Baseline data collected included Hgb, hematocrit, platelets, glomerular filtration rate, prothrombin time (PT)/international normalized ratio (INR), activated partial thromboplastin time (aPTT), and markers of liver function, including transaminases and total bilirubin. The presence of any co-morbidities that may impact hemostasis and postoperative outcomes was also recorded. Finally, charts were reviewed to determine outcome data, including postoperative Hgb, transfusion of any blood products and factor replacement therapies, LOS, and hospital readmission.
Control Population
Given that our patient population underwent a variety of surgeries, determining baseline rates for surgical complications and outcomes for these procedures is challenging. In order to compare the outcomes of our population of PwBD to those without bleeding disorders undergoing the same surgeries, the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database was queried for 2018, the most recent available year. This is a validated surgical database containing de-identified individual patient data from over 600 participating hospitals, and measures data from the preoperative period through 30 days postoperatively. Only NSQIP patients with a surgical Common Procedural Terminology (CPT®) code matching any of our study patients were included and, in order to obtain a representative sample of the general population undergoing these procedures electively, any NSQIP patients with a known bleeding disorder or whose surgery was non-elective were excluded. Only NSQIP patients with a CPT code shared by our patients were included for comparison, but not all of our study patients had a surgery that was included in the NSQIP database, therefore the study population for comparison was smaller than the full study population.
Propensity Score Matching and Statistical Analysis
Propensity score (PS) matching was utilized to match PwBD procedures to non-PwBD in the NSQIP database with similar characteristics of age, sex, and surgical procedure. PS matching was conducted using Proc PSMATCH in SAS. All available observations were selected (NSQIP contained 245,978 procedures with any CPT code shared by a study patient), and an optimal matching algorithm matched the PwBD procedures to the NSQIP cohort by 1:60 without replacement. Following matching, 2400 surgeries were extracted from NSQIP to form a representative sample of surgeries in control patients without a bleeding disorder. Matching used a default caliper width of 0.20 times the standard deviation of the estimated logit of the PS. For good variable balance, the absolute standardized difference was less than to 0.25 and the variance ratio were between 0.5 and 2. The output data set created by the PSMATCH procedure served as the input for the statistical procedures run for the outcome analysis.
For outcome analysis, continuous variables are reported as mean (range) and were compared between study patients and matched NSQIP controls using independent samples T-test. Categorical variables were compared between groups using Fisher's exact test. A P value < .05 was used for statistical significance. Data were analyzed using the SAS v9.4 (SAS Institute Inc., Cary, NC).
Results
Patient Characteristics
During the study period, 50 patients underwent a total of 63 major surgeries. Among them, 29 (58.0%) were female and mean age at the time of surgery was 50.9 years. The most common diagnosis was VWD (64.0%)—with Type 1 (42.0%) the most frequent subtype—followed by hemophilia A (20.0%) and RBD (16.0%). Most patients (48.0%) were characterized as having a mild bleeding disorder by either baseline coagulation factor activity (in the case of hemophilia patients) or clinical judgment by the treating hematologist. Three (6.0%) had a severe phenotype, including one patient with an inhibitor, and two (4.0%) used chronic outpatient prophylaxis. 44% had no severity documented based on factor activity or bleeding assessment tool. Characteristics of the study population are summarized in Table 1 and details on each patient are shown in Supplemental Table S1 in the Supplementary Appendix.
Baseline Characteristics of Study Population.
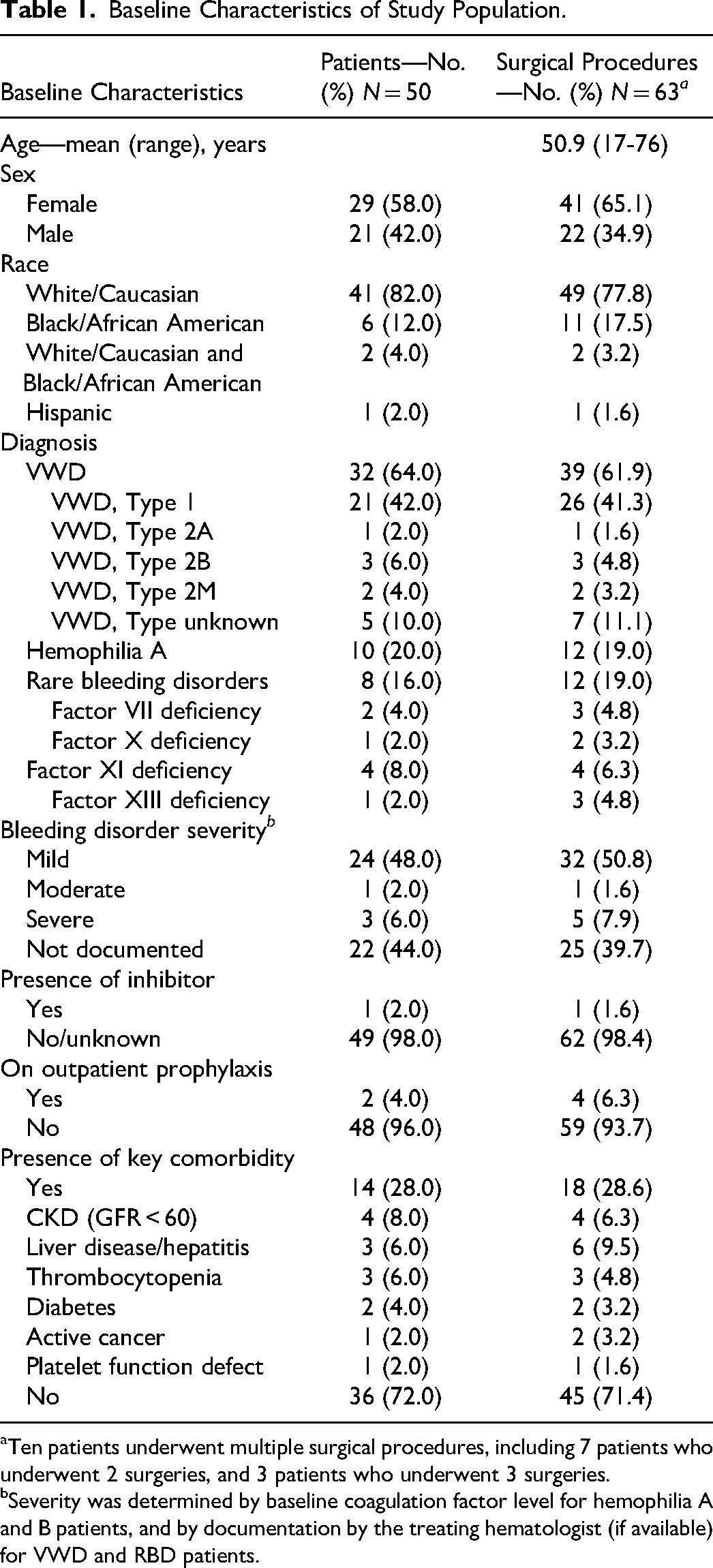
Ten patients underwent multiple surgical procedures, including 7 patients who underwent 2 surgeries, and 3 patients who underwent 3 surgeries.
Severity was determined by baseline coagulation factor level for hemophilia A and B patients, and by documentation by the treating hematologist (if available) for VWD and RBD patients.
Surgical Procedures and Hemostatic Therapies
The types of surgeries undergone by our patients are shown in Table 2. Among 63 total procedures, the most common category was orthopedic (n = 21, 33.3%), including 12 arthroplasties, three spinal decompression/fusion surgeries, and two open reduction and internal fixations of the radius. Head and neck (n = 14, 22.2%), abdominal (n = 8, 12.7%), and gynecologic/pelvic (n = 7, 11.1%) surgeries were also common (see Supplemental Table S1 for details of all surgeries). Preoperative hemostatic therapy was recommended in 58 (92.1%) of surgeries and planned postoperative therapy in 34 (54.0%). The five surgeries performed without hemostatic prophylaxis included three surgeries in two patients (intrathecal pump replacement, hysterectomy/bilateral salpingo-oopherectomy, and repair of a cystocele and rectocele) with historic diagnoses of VWD but whose preoperative baseline VWF activity was near 100 IU/dL, a melanoma excision and sentinel lymph node biopsy in a patient with mild FVII deficiency, and a laparoscopic cholecystectomy in a patient with a diagnosis of FXI deficiency whose preoperative baseline had increased to >50%. The most commonly prescribed preoperative hemostatic therapy was plasma-derived VWF-FVIII concentrate (n = 28, 44.4%), followed by recombinant FVIII (n = 11, 17.5%), DDAVP (n = 7, 11.1%), and oral antifibrinolytic therapy (n = 4, 6.4%). All patients who received factor replacement therapy prior to surgery were given doses to target preoperative activity levels >80% to 100%, with postoperative doses individualized according to each patient and surgery.
Surgical Procedures and Outcomes among Study Population.

Five patients received two preoperative hemostatic therapies.
Hgb, hemoglobin; DDAVP, desmopressin.
Postoperative Outcomes
Postoperatively, there were no bleeding complications in 59 surgical procedures (93.7%). The primary outcome of major bleeding according to ISTH-SSC criteria was met in three surgeries (4.8%) among three distinct patients. One surgery (1.6%) in a different patient was complicated by clinical bleeding not meeting these criteria. Among the three patients with major bleeding, two met criteria via unexpected surgical site bleeding with Hgb drop ≥ 2 g/dL and one had a Hgb drop and required transfusion of ≥2 units of packed red blood cells. Specifically, the major bleeding events included the following: a patient with mild type 1 VWD who developed unexpected bleeding and a 3.4 g/dL Hgb drop following endoscopic sinus surgery with septoplasty and turbinectomy, which required use of unplanned plasma-derived VWF-FVIII concentrate and antifibrinolytic therapy; a patient with mild hemophilia A (baseline FVIII activity 12%) with a 3.1-g/dL Hgb drop from baseline after revision of a hip arthroplasty, who also required transfusion of one unit of packed red blood cells; and a patient with FVII deficiency (baseline activity 8%) who underwent partial hepatectomy for an adenoma and experienced unexpected bleeding postoperatively, with 2.8 g/dL Hgb drop and requirement of 5 units packed red blood cell transfusion.
Five patients undergoing five distinct surgeries (7.9%) required unplanned postoperative hemostatic therapy, including either more doses or additional products of factor replacement than specified before surgery. This included two of the above patients with major bleeding (the patients with VWD and FVII deficiency undergoing septoplasty and partial hepatectomy, respectively); one patient with VWD who was given a follow-up outpatient dose of DDAVP after septoplasty for an undocumented reason; one patient with VWD who received 2 days more of plasma-derived VWF-FVIII concentrate than planned after a shoulder arthroplasty, despite no reported bleeding; and one patient with VWD who received one additional dose of plasma-derived VWF-FVIII concentrate prior to hospital discharge following hysterectomy, but also had no bleeding. The mean inpatient LOS for all surgeries was 1.65 days, and was significantly lower for those that were not complicated by major bleeding (mean 1.37 days, vs 7.33 days for those with major bleeding, P < .001). One surgery was followed by an inpatient readmission within 30 days (1.6%), and three additional ones (in three distinct patients) required a follow-up emergency department visit related to the procedure. No patients experienced a venous thromboembolism (VTE) during the surgical admission.
Comparison to NSQIP Control Population
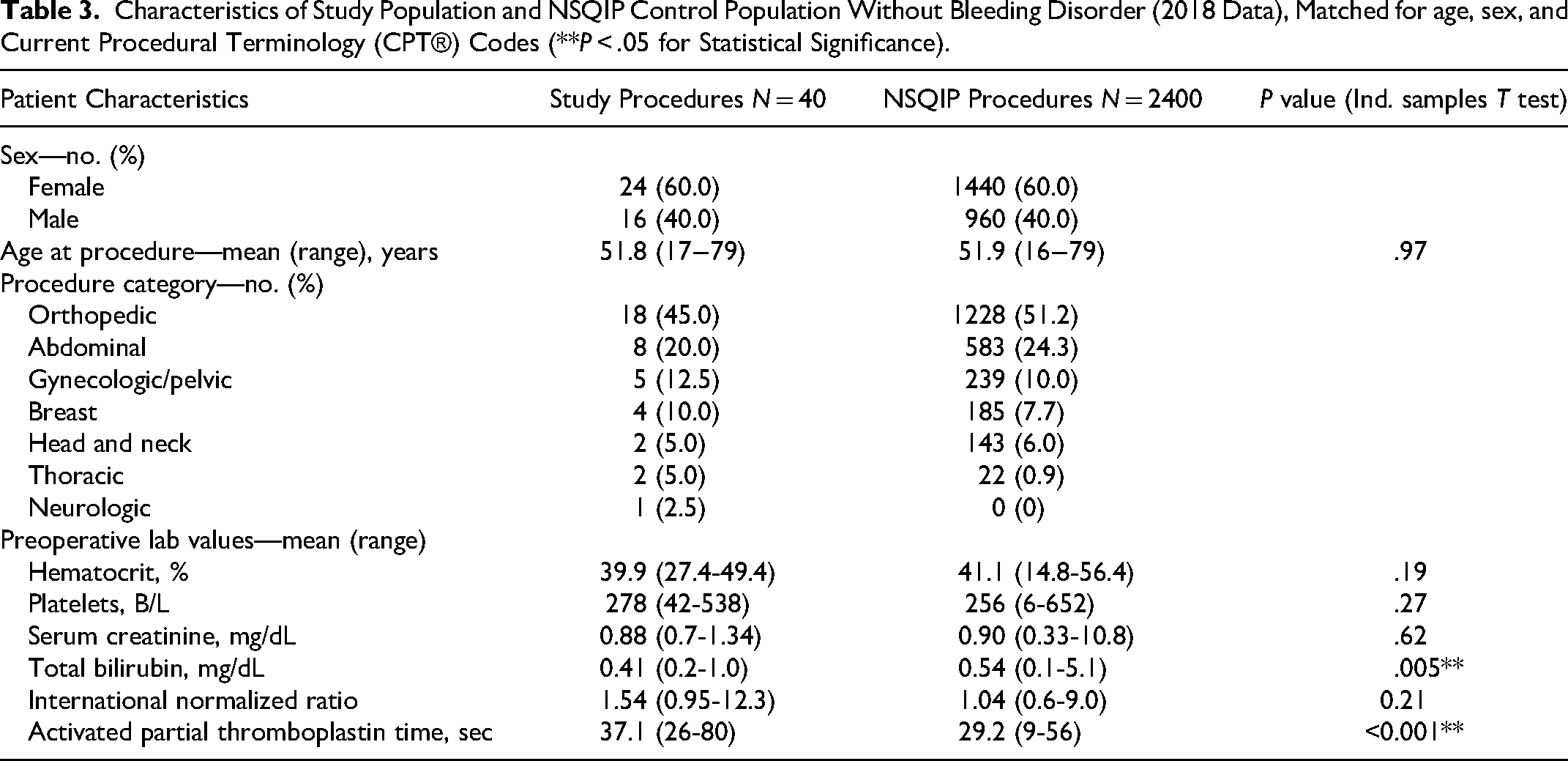
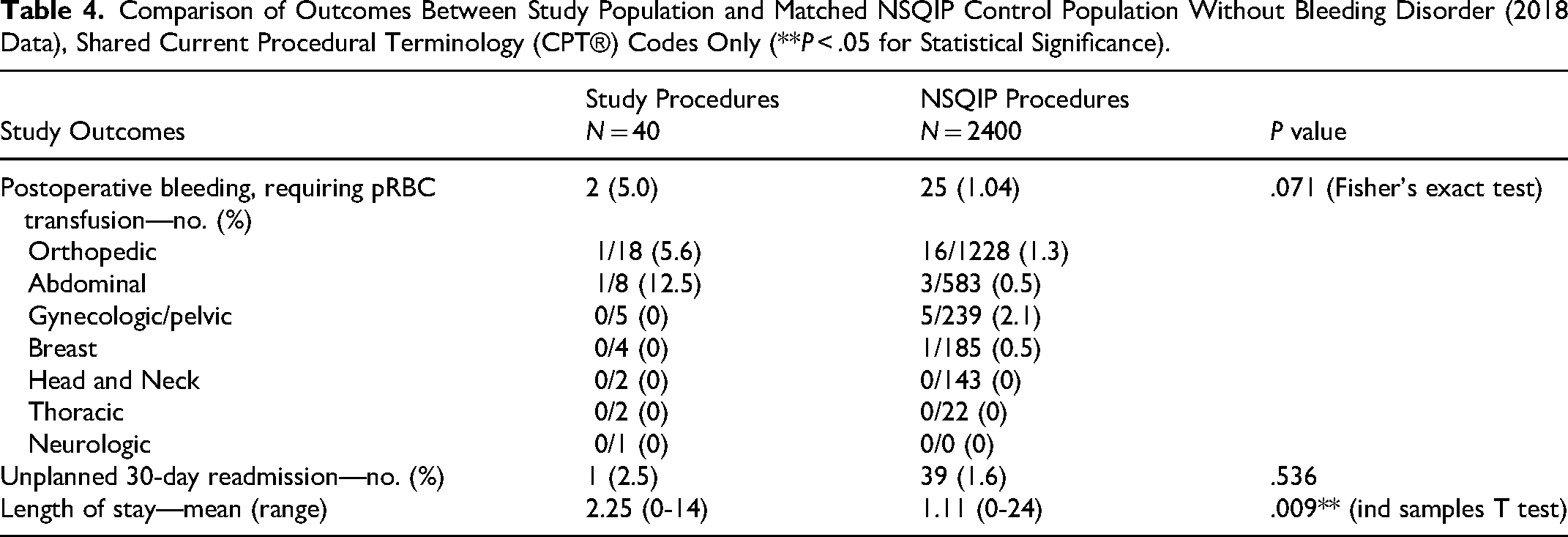
The 2018 ACS NSQIP database was queried to establish baseline rates of complications and outcomes in non-bleeding disorder patients undergoing the same procedures as our PwBD population. Not every surgical CPT® code in our population matched to those available in NSQIP, thus our PwBD comparison population included 35 patients undergoing 40 surgeries. The NSQIP database included 245,978 surgeries with a CPT code shared a study patient. Following matching for age, sex, and surgical procedure, 2400 NSQIP procedures served as the control group. Characteristics of each group are shown in Table 3. NSQIP defines bleeding only as that which requires postoperative transfusion—a different definition than that of the ISTH-SSC which we used for our full study population, which considers Hgb drop, interventions required to achieve hemostasis, and number of transfused red blood cell units—however, all bleeding events in the PwBD patients in the comparison arm included transfusion (one patient who did not share a NSQIP CPT code met major bleeding via Hgb drop), so none that met other ISTH-SSC criteria were excluded. Postoperative major bleeding rates were low in both groups (5.0% in PwBD procedures vs 1.04% in NSQIP controls, P = .071) and there was no significant difference in unplanned 30-day readmission rates related to surgery (2.5% following PwBD procedures vs 1.6% in NSQIP controls, P = .536). Mean LOS was longer following surgeries among study patients (2.25 vs 1.11 days, P = .009), though there was no significant difference when considering only procedures for which there were no bleeding complications (1.82 vs 1.28 days, P = .062). These data are summarized in Table 4.
Characteristics of Study Population and NSQIP Control Population Without Bleeding Disorder (2018 Data), Matched for age, sex, and Current Procedural Terminology (CPT®) Codes (**P < .05 for Statistical Significance).
Comparison of Outcomes Between Study Population and Matched NSQIP Control Population Without Bleeding Disorder (2018 Data), Shared Current Procedural Terminology (CPT®) Codes Only (**P < .05 for Statistical Significance).
Discussion
To our knowledge, this is among the largest descriptive analyses of outcomes of PwBD undergoing major surgery. We demonstrated that with comprehensive care and preoperative planning, PwBD can undergo elective major surgeries with risks of major bleeding complications similar to those of the general, non-bleeding disorder population. In our population of 50 PwBD undergoing 63 surgeries, we observed a major bleeding rate of 4.8%, using the ISTH-SSC definition 32 and 30-day hospital readmission rate of 1.6% of all surgeries.
Few prior studies have specifically measured outcomes of PwBD undergoing major surgery. An earlier report from 1986 of 22 patients undergoing 23 major abdominal surgeries observed bleeding in 17.4% and deaths in two patients. 35 Another study of 55 PwBD in the modern factor replacement era found minor bleeding in 5.5% of patients undergoing appendectomy, cholecystectomy, hemorrhoidectomy, and inguinal hernia repair, with mean LOS varying between 7.5 and 10.9 days for different surgeries. 25 While primary endpoints and classification of bleeding differ between studies, our results compare favorably to these published outcomes. Among hemophilia patients undergoing total joint arthroplasty, bleeding has been reported in 8.7% to 8.9% of cases.20,21 In our study, four hemophilia patients (all with mild hemophilia A) underwent native total joint arthroplasty (three knee, one hip) with no bleeding events. One patient with mild hemophilia A underwent revision of a prior hip arthroplasty and had a major bleeding complication, with unexpected bleeding and ≥2 g/dL Hgb drop. This patient also required a prolonged inpatient admission of 14 days due to insurance issues necessitating him completing his course of factor replacement therapy in the hospital. In general, however, the LOS of our study patients was shorter than that reported among the PwBD population getting elective abdominal surgeries. 25 No other studies in a major surgery population reported the use of unplanned hemostatic therapies, but we feel that the rate of 7.9% of surgeries in our study population represents an excellent outcome and successful preoperative planning, given this high-risk population. Another strength of our study was its inclusion of >50% female patients, as most early studies of PwBD included men with hemophilia. Gynecologic and breast surgeries—which represented 15/63 (23.8%) of surgeries in our study—are common and carried the highest risk of bleeding among NSQIP patients included in our study.
Because our PwBD patients underwent a variety of surgeries, comparing complication rates to baselines for each procedure represented a challenge. To determine how the complication rates in our study patients compared to those of a general, non-bleeding disorder population undergoing similar procedures, we utilized the ACS NSQIP database. This database includes risk-adjusted data gathered by trained staff directly from medical charts of patients at participating institutions nationally, with data collected from the preoperative period to 30 days postoperatively. Rather than create matched pairs with small numbers of patients for different surgeries, the NSQIP database allowed us to estimate complication rates in the general population. Including only NSQIP patients who had a primary surgical CPT® code in common with at least one study patient, and excluding those with a diagnosed bleeding disorder, we generated a list of 245,978 patients in 2018, the most recent year available in their database. PS matching was then employed, and study patients were matched to controls in a 1:60 ratio by age, sex, and surgical CPT® code, to generate a set of 2400 matched non-PwBD controls for comparison.
The rate of major bleeding—defined by NSQIP as postoperative bleeding requiring red blood cell transfusion—was 1.04% for all included procedures in the matched NSQIP population, which was not significantly different than the observed per-surgery rate in PwBD study patients sharing a common CPT® code (5.0%). This suggests that with proper preoperative planning and hemostatic therapy before and after surgery, PwBD carry a risk of bleeding from major surgery similar to the general population. The mean LOS for procedures in PwBD patients was significantly longer than in matched NSQIP controls, though this was driven by a prolonged 14-day hospital stay in a patient with hemophilia A who was required to complete his planned course of factor replacement therapy inpatient for insurance reasons. This patient was not a long-term member of our HTC and had been seen only once preoperatively. Among patients who did not experience bleeding, there was no significant difference in LOS, suggesting that administering perioperative hemostatic therapy may not prolong the hospital stays of PwBD undergoing surgery. This contrasts with another study of major surgeries in PwBD, which observed longer LOS than control patients. 25 In aggregate, these findings highlight the importance of receiving multidisciplinary care at an HTC to safely manage surgical procedures in PwBD.
Our study had certain limitations, including the small number of patients and retrospective design. Only patients whose surgeries were performed at our hospital were included for the purposes of adequate data collection, thereby excluding many of our HTC patients whose procedures occurred at local institutions. The small study size precluded meaningful subgroup analyses that may have shed light on risks for each bleeding disorder. In addition to the small sample size, the fact that the PwBD population underwent a variety of surgeries made it difficult to draw conclusions about how their outcomes compared to the general population. Similarly, the fact that the study population comprised a heterogeneous group of bleeding disorders and severities, including some RBDs that carry an inherently lower risk of bleeding, makes it difficult to draw strong conclusions about the surgical risks among specific disease entities or severities. Our study population also included only three patients with severe disease and one with an inhibitor, which may limit the generalizability of our findings to other HTC populations. Further, most VWD patients had VWF activity >30%, including 33/42 (78.6%) with preoperative levels in the normal range. However, these patients all carried historic diagnoses of VWD with previously low levels and were included in the study in accordance with data showing high rates of VWF mutations in persons with VWF activity between 30 and 50 IU/dL 36 and inconsistent and variable improvement in the bleeding phenotype in patients with a historic diagnosis of VWD whose levels normalize with age.27,36–38
Another limitation was that we did not measure other potentially important surgical outcomes, including time of operation and wound complications, which have been reported to be high in PwBD for certain surgeries.21,25 The ACS NSQIP database was chosen to establish baseline complication rates for each surgery type, but it carries specific limitations. Some study patients underwent surgeries that were not included in NSQIP, thus limiting the number of PwBD who could be compared to controls. The NSQIP database also does not include all variables that we collected and uses a different definition of bleeding than that of the ISTH-SSC that we used for study patients. Thus, NSQIP may underestimate rates of major bleeding for these procedures in a general population. Our statistical analysis was also limited by the deidentification of NSQIP, as it is unknown whether the same patients may have undergone multiple surgeries captured in the database. Finally, while we did not observe any instances of postoperative VTE during the admission for surgery, we did not measure whether patients received pharmacologic VTE prophylaxis, which is a challenging clinical decision in PwBD.
Conclusions
This retrospective study at a single HTC suggests that, with comprehensive care and preoperative planning, PwBD can safely undergo major surgical procedures with risks of bleeding complications similar to those of a general, non-bleeding disorder population. We observed few bleeding complications or inpatient readmissions, and while LOS was significantly longer in PwBD than control patients, overall it remained relatively short despite most patients being planned for postoperative hemostatic therapy.
Supplemental Material
sj-docx-1-cat-10.1177_10760296231165056 - Supplemental material for Perioperative Outcomes of Patients with Bleeding Disorders Undergoing Major Surgery at an Academic Hemophilia Treatment Center
Supplemental material, sj-docx-1-cat-10.1177_10760296231165056 for Perioperative Outcomes of Patients with Bleeding Disorders Undergoing Major Surgery at an Academic Hemophilia Treatment Center by Ruben Rhoades, Zachary French, Amy Yang, Karen Walsh, Douglass A. Drelich and Steven E. McKenzie in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors would like to thank all of patients and staff of the Cardeza Foundation HTC. They also would like to thank the Eastern Pennsylvania Bleeding Disorders Foundation for their generous grant support of this work.
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Author Contributions
All authors conceived and designed the study, and approved the final version of the article. RR and ZF collected the data. KW, AY, and RR performed data analysis. RR, KW, and AY drafted the manuscript. SM reviewed the manuscript for intellectual content, and provided critical revisions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DD received honoraria from CSL Behring, OctaPharma, Bayer, NovoNordisk, and Pfizer. Since the completion of data collection, analysis, and manuscript writing, he began employment at CSL Behring. RR, ZF, KW, AY, and SM declare no relevant interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.