
Abstract
Background and Purpose
Deep venous thrombosis (DVT) makes spontaneous intracerebral hemorrhage (ICH) treatment more challenging. We aimed to determine the predictive ability of D-dimer combination with albumin for DVT in spontaneous ICH.
Methods
Spontaneous ICH patients were retrospectively included. Univariate and multivariate logistic regression analyses were performed. The restricted cubic spline (RCS) curve was adopted. Multivariate logistic regression analysis was further conducted to assess the predictive powers of D-dimer and albumin in different models. Besides, the incremental predictive ability of D-dimer combination with albumin was evaluated with areas under the curve (AUC), net reclassification improvement (NRI), and integrated discrimination index (IDI).
Results
D-dimer was significantly higher, while albumin was considerably lower in the DVT group than in the non-DVT group [D-dimer, 0.47 (0.29, 1.08) versus 0.98 (0.48, 2.49), P < .001; albumin, 39.45 ± 7.05 versus 36.93 ± 4.77, P < .001). The multivariate logistic regression analysis showed that higher D-dimer and lower albumin were independently related to DVT after controlling confounders (D-dimer, OR = 1.061, 95% CI = 1.012–1.112, P = .013; albumin, OR = 0.934, 95% CI = 0.895–0.973, P = .001). The best cut-off value of the D-dimer was 0.40, and the albumin was 37.15. Besides, D-dimer and albumin had good predictive abilities in different models. The AUC, NRI, and IDI revealed that models that included the D-dimer combination with albumin had better predictability than those without.
Conclusions
D-dimer combination with albumin has a good predictability of DVT in spontaneous ICH.
Introduction
Spontaneous intracerebral hemorrhage (ICH), which is caused by non-traumatic, is the second most prevalent form of stroke after acute ischemic stroke (AIS).1,2 Deep vein thrombosis (DVT), one type of venous thromboembolism (VTE), is a severe complication that emerges in the early period following ICH and links to high morbidity and mortality.2,3 ICH patients have a much higher risk of developing DVT than patients with AIS.4 However, the treatment options for ICH patients with DVT are full of contradictions. 4 Thus, early identification of the high DVT risk and taking appropriate precautions are crucial.
D-dimer is a sensitive but nonspecific indicator for DVT.5,6 At the conclusion of the coagulation process, fibrinogen converts into fibrin monomers in the presence of thrombin.7,8 As the concentration of fibrin monomers increases, they combine to form polymers.7,9,10 Soluble fibrin polymers act as cofactors with thrombin in activating coagulation factor XIII.7,9,11 At the same time, the activated coagulation factor XIII promotes the formation of cross-links of adjacent fibrin molecules, forming stable fibrin polymers.9,11 Fibrinolysis is associated with coagulation.12,13 Concurrently with thrombosis, the body will produce anti-fibrinolysis substances.8,12,13 D-dimers are fibrin polymers with D-D segments of fibrin molecules.9,14 The increase of D-dimers reflects the activation of coagulation and the fibrinolytic system.7,9,11 Clinically, D-dimer negativity is often used to exclude thrombotic disease.5,6 However, the relationship between the D-dimer level and DVT in spontaneous ICH patients has yet to be well studied. 15
According to past research, low albumin plays a role in the development of DVT. First, albumin inhibits the polymerization of fibrin and the aggregation of platelets.16,17 Additionally, albumin appears to have heparin-like effects.17,18 Second, low albumin levels can reflect the existence of certain disorders, such as nephrotic syndrome or chronic renal disease, both of which are risk factors for DVT. 19 Third, low albumin causes a decrease in plasma colloid osmolality, which increases blood viscosity, ultimately resulting in thrombosis. 20 However, the combination of D-dimer and albumin in predicting DVT in patients with spontaneous ICH remained unknown.
Therefore, this study aimed to explore the combination of D-dimer and albumin in predicting DVT in patients with spontaneous ICH.
Materials and Methods
Study Population
This research involved consecutive spontaneous ICH patients from the neurology inpatient department of the First Affiliated Hospital of Wenzhou Medical University from January 2019 to October 2021. Patients who fulfilled each one of the inclusion criteria were included: (1) ≥ 18 years old; (2) diagnosis of spontaneous ICH, including primary intraventricular hemorrhage (IVH); (3) within 48 h from the onset. Patients who fulfilled one or more of the exclusion criteria were excluded: (1) severe liver disease; (2) severe kidney disease; (3) previous anticoagulation; (4) incomplete data.
This study was permitted by the ethics committee of the First Affiliated Hospital of Wenzhou Medical University with the registration number KY2021-R077 and met the local Research Ethics Committee's ethical standards for human experimentation. Each procedure adhered to the Helsinki Declaration. Due to the application of a retrospective study design, written consent was not required.
Data Collection
The clinical information of patients with spontaneous ICH was retrieved from electronic medical records. Demographic characteristics (eg, age and gender); medical history (eg, smoking, drinking, hypertension, diabetes, atrial fibrillation, hyperlipidemia, malignancy, hyperlipemia, and history of ischemic or hemorrhagic stroke); medication history (eg, antiplatelet, antihypertensive, lipid-lowering, and antidiabetics); the position of ICH [eg, cerebellum, deep supratentorial (corpus callosum, basal ganglia, internal capsule, thalamus, and corona radiata), brainstem, lobar, and the presence of IVH]; surgery; other complications (pneumonia); laboratory tests [eg, leukocyte, neutrophil, red blood cells (RBCs), platelet, glucose, blood urea nitrogen (BUN), serum calcium, prothrombin time (PT), international normalized ratio (INR), fibrinogen (FIB), activated partial thromboplastin time (APTT), thrombin time (TT), D-dimer, albumin, alanine aminotransferase (ALT), estimated glomerular filtration rate (eGFR), serum uric acid (SUA), total cholesterol (TC), triglyceride, high-density lipoprotein (HDL), and low-density lipoprotein (LDL)] were obtained. Laboratory tests were collected within 24 h after admission the following day after an overnight fast for at least 8 h. The Glasgow Coma Scale, the National Institutes of Health Stroke Scale (NIHSS), and the previously modified Rankin Scale (Pre-mRS) were collected on admission. Lower limb Doppler ultrasonography is a routine test item for every stroke patient during hospitalization in our hospital within one week. Patients were evaluated for DVT with Doppler ultrasonography, regardless of symptomatology.
Statistical Analysis
Continuous variables that matched normal distribution were expressed as mean ± standard deviation (SD), whereas those that did not were presented as median (Q1, Q3). Categorical variables are shown as frequency (percentage). The Student's test and Analysis of Variance were employed to compare normally distributed continuous variables. To investigate the differences between non-normally distributed continuous variables, Mann–Whitney and Kruskal–Wallis tests were employed. Using Chi-square and Fisher's exact tests, the categorical variables were compared. Significant variables in the univariable logistic regression analysis were entered into the multivariate logistic regression analysis. Multivariate logistic regression analysis was adopted to determine further the association between D-dimer, albumin, and DVT in patients with spontaneous ICH. Variables with P < .05 in the multivariable analysis were preserved to generate a nomogram. The score for each variable was determined using the values of the regression coefficients. Areas under the curve (AUC) of the receiver operating characteristic (ROC) were utilized to assess the discrimination capability of the nomogram. The calibration curve was evaluated graphically by smoothing a scatter plot of predicted and actual probabilities. A decision curve analysis (DCA) was undertaken to estimate the model's clinical net benefit. The ROC was used to compare the predictability of D-dimer and albumin in DVT and determine the optimal cutoff values. Restricted cubic spline (RCS) curves were drawn to analyze the linear relationship. Multivariate logistic regression analyses were further used to determine the D-dimer and albumin's predictability for DVT in different models. Model 1 was adjusted for age, gender, and D-dimer or albumin. Model 2 was adjusted for covariates from Model 1 and for NIHSS and albumin or D-dimer. Model 3 was adjusted for all variables with a P-value < .05 in the univariable analysis. The area under the curve (AUC), net reclassification index (NRI), and integrated discrimination improvement (IDI) were utilized to evaluate the value of D-dimer combined with albumin in DVT prediction in patients with spontaneous ICH. Statistical analyses were performed in the R version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria, 2022) and the SPSS Statistics 28.0 software (SPSS Inc., Chicago, IL, United States, 2021). A P-value < .05 was considered to be statistically significant.
Results
Characteristics of Spontaneous ICH Patients with or Without DVT
Eight hundred thirty-five eligible patients with spontaneous ICH were included in this study (Figure 1). The incidence of DVT in this study was 26.35%. Table 1 shows a comparison of the baseline features of DVT and non-DVT patients. D-dimer was significantly higher, while albumin was substantially lower in DVT than in non-DVT groups [D-dimer, 0.47 (0.29, 1.08) versus 0.98 (0.48, 2.49), P < .001; albumin, 39.45 ± 7.05 versus 36.93 ± 4.77, P < .001). Patients with DVT were older, more likely to undergo surgery and pneumonia, and had higher GCS and NIHSS scores, higher probability of the presence of IVH, lower RBC, more elevated glucose, higher BUN, more insufficient serum calcium, higher FIB, higher eGFR, and lower SUA (all P < .05). Besides, no statistical differences have been found in gender, smoking, drinking, hypertension, diabetes, atrial fibrillation, malignancy, hyperlipemia, pre-ischemic stroke, pre-hemorrhagic stroke, pre-antiplatelet, pre-antihypertensive, pre-lipid lowering, pre-antidiabetics, pre-mRS, cerebellum, deep supratentorial, brainstem, lobar, leukocyte, neutrophil, platelet, PT, INR, APTT, TT, ALT, TC, triglyceride, HDL, and LDL (all P > .05).

The flow of patient selection. ICH, intracerebral hemorrhage; DVT, deep venous thrombosis.
Characteristics of Spontaneous ICH Patients with or Without DVT.

Notes: ICH, intracerebral hemorrhage; DVT, deep venous thrombosis; pre, previous; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; mRS, Modified Rankin Score; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; PT, prothrombin time; INR, international normalized ratio; FIB, fibrinogen; APTT, activated partial thromboplastin time; TT, thrombin time; ALT, alanine aminotransferase; eGFR, estimated glomerular filtration rate; SUA, serum uric acid; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Multivariate Logistic Analyses of Risk Factors for DVT in Spontaneous ICH Patients
Multivariate logistic regression analysis was adopted to determine the association between risk factors and DVT in patients with spontaneous ICH (Table 2). After controlling the confounders (including age, gender, GCS, NIHSS, presence IVH, surgery, pneumonia, RBC, glucose, BUN, serum calcium, FIB, D-dimer, albumin, eGFR, and SUA, all P < .05 in univariate logistic regression analysis), multivariate regression analyses revealed that higher D-dimer and lower albumin were independently related to DVT (D-dimer, OR = 1.061, 95% CI = 1.012–1.112, P = .013; albumin, OR = 0.934, 95% CI = 0.895–0.973, P = .001). Meanwhile, elder patients (OR: 1.047, 95% CI = 1.030–1.065, P < .001) and patients with higher NIHSS scores (OR:1.071, 95% CI = 1.019–1.127, P = .012) were also associated with DVT in spontaneous ICH patients.
Multivariate Logistic Analyses of Risk Factors for DVT in Spontaneous ICH Patients.

Notes: DVT, deep venous thrombosis; ICH, intracerebral hemorrhage; OR, odds ratio; CI, confidence level; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; FIB, fibrinogen; eGFR, estimated glomerular filtration rate; SUA, serum uric acid.
Based on the multivariable logistic regression analysis, a nomogram for predicting DVT risk based on the age, NIHSS score, D-dimer, and albumin concentration was constructed (Figure 2). The AUC of the nomogram for the whole cohort was 0.747 (Figure S1). The nomogram calibration plots demonstrated a moderate level of cohort prediction accuracy (Figure S2). Figure S3 depicts the DCA for the nomogram model used to predict DVT risk. The nomogram's clinical value is shown with the area enclosed by the model curve, black, and gray lines.

The nomogram predicting model for DVT risk. Each variable's locations on the appropriate axis were verified and connected vertically to the top “Points” axis to calculate the score. Users added up the scores of variables to acquire the final score on “Total Points” and then drew a vertical line from the axis of total points to the bottom scale to determine the risk of DVT. DVT, deep venous thrombosis; NIHSS; National Institutes of Health Stroke Scale.
ROC Curve to Determine the Prediction Ability of the D-Dimer and Albumin in DVT
The ROC curve was utilized to determine D-dimer and albumin prediction ability in DVT. The results indicated that the AUC of the D-dimer was 0.680 (0.641-0.719) with 43.9% specificity and 85.9% sensitivity, and the AUC of albumin was 0.639 (0.596-0.682) with 69.1% specificity and 53.2% sensitivity. Moreover, the best cut-off value of the D-dimer was 0.40, and the albumin was 37.15 (Figure 3).
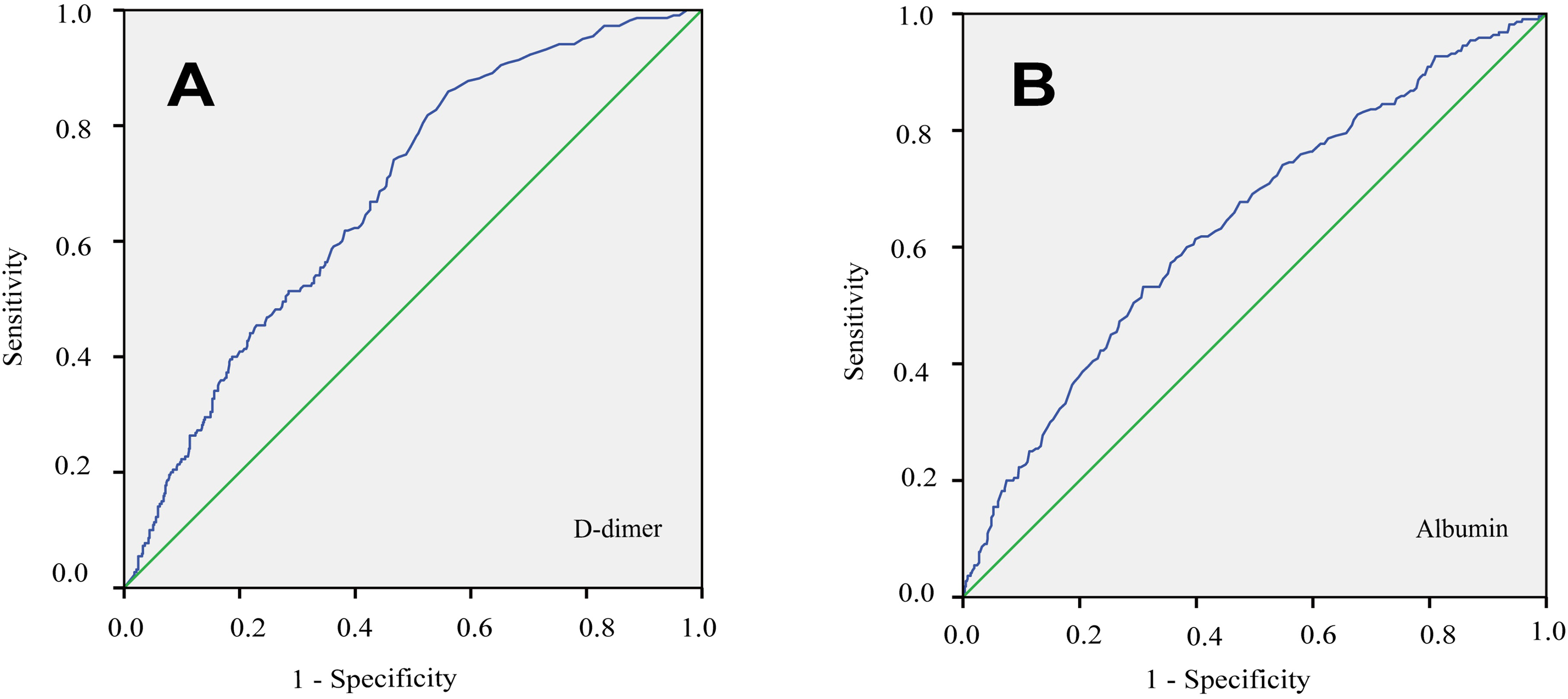
ROC analysis of D-dimer and albumin for DVT in patients with spontaneous ICH. ROC, the receiver operating characteristic; AUC, the area under the curve; DVT, deep venous thrombosis; ICH, intracerebral hemorrhage.
RCS to Determine Linear Relationships
RCS demonstrated a no-linear relationship between D-dimer and DVT (P for nonlinearity < .001). When the D-dimer value was between 0 and 3.43 mg/L, the risk of DVT increased fast with D-dimer elevation. In contrast, the risk of DVT was relatively steady, with the D-dimer levels of more than 3.43 mg/L (Figure 4A). Additionally, there was always a linear relationship between albumin and DVT in patients with spontaneous ICH (P for linearity < .001) (Figure 4B).
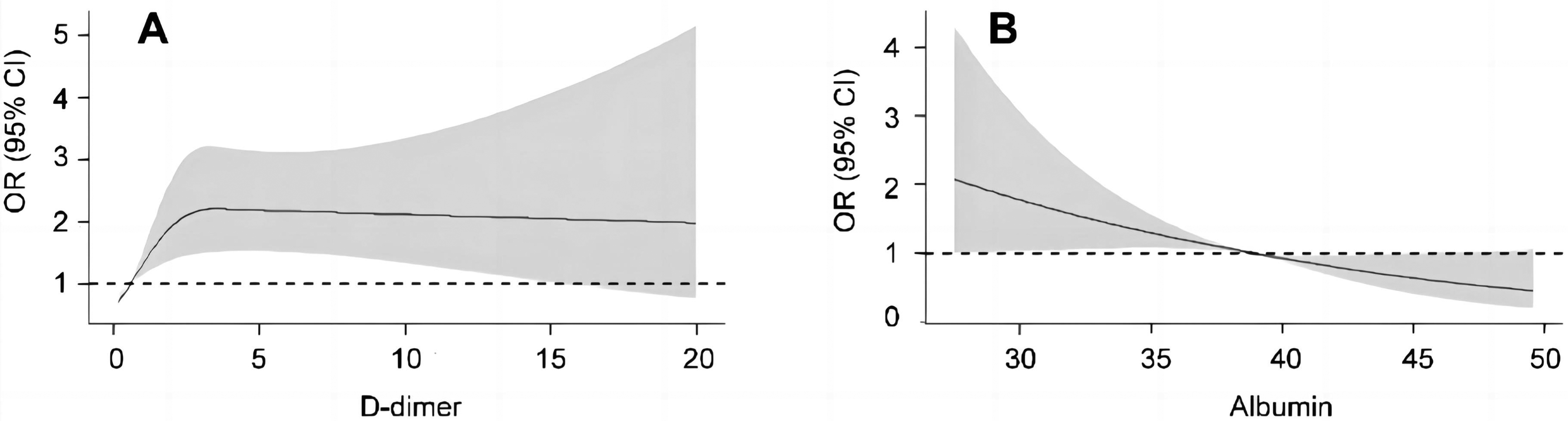
RCS analysis of D-dimer and albumin for DVT in patients with spontaneous ICH. (A) The model was adjusted for gender, age, surgery, GCS, NIHSS, presence-IVH, pneumonia, RBC, glucose, BUN, serum calcium, FIB, albumin, eGFR, and SUA. (B) The model was adjusted for gender, age, surgery, GCS, NIHSS, presence-IVH, pneumonia, RBC, glucose, BUN, serum calcium, FIB, D-dimer, eGFR, and SUA. RCS, restricted cubic spline; DVT, deep venous thrombosis; ICH, intracerebral hemorrhage; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; FIB, fibrinogen; eGFR, estimated glomerular filtration rate; SUA, serum uric acid.
Multivariate Logistic Regression Analysis of the D-Dimer and Albumin in Different Models
Multivariate logistic regression analysis was conducted to determine the D-dimer's and albumin's predictability for DVT in different models (Table 3 and Table 4). Regarding the D-dimer, model 1 was adjusted for age, gender, and D-dimer. Model 2 was adjusted for covariates from model 1 and for NIHSS and albumin. Model 3 was adjusted for all variables with P < .05 in the univariable analysis. All the results showed a positive correlation between the D-dimer level and the possibility of developing DVT (all P < .05). Regarding albumin, model 1 was adjusted for age, gender, and albumin. Model 2 was adjusted for covariates from Model 1 and for NIHSS and D-dimer. Model 3 was adjusted for all variables with a P < .05 in the univariable analysis. Except for albumin Q2 (35.50 - 38.90) and albumin Q3 (38.90 - 41.60) in model 2 and model 3 (Q2 in model 2, P = .134; Q2 in model 3, P = .187; Q3 in model 2, P = .073; Q3 in model 3, P = .113), all the other albumins had a negative correlation with DVT (all P < .05).
Multivariate Logistic Regression Analyses of D-Dimer for DVT in Different Models in Spontaneous ICH Patients.
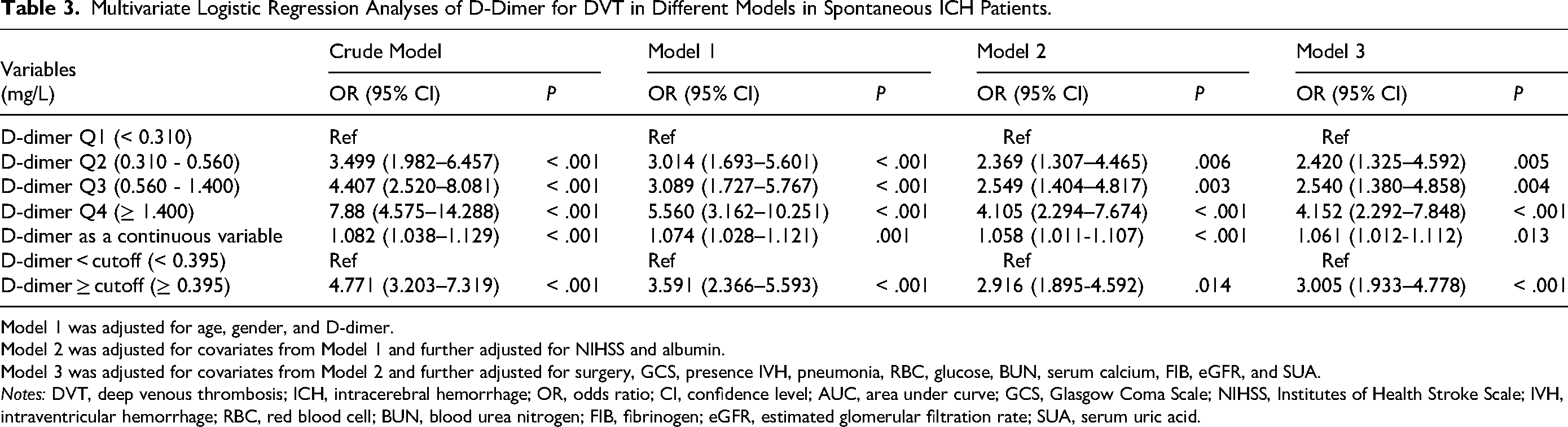
Model 1 was adjusted for age, gender, and D-dimer.
Model 2 was adjusted for covariates from Model 1 and further adjusted for NIHSS and albumin.
Model 3 was adjusted for covariates from Model 2 and further adjusted for surgery, GCS, presence IVH, pneumonia, RBC, glucose, BUN, serum calcium, FIB, eGFR, and SUA.
Notes: DVT, deep venous thrombosis; ICH, intracerebral hemorrhage; OR, odds ratio; CI, confidence level; AUC, area under curve; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; FIB, fibrinogen; eGFR, estimated glomerular filtration rate; SUA, serum uric acid.
Multivariate Logistic Regression Analyses of Albumin for DVT in Different Models in Spontaneous ICH Patients.

Model 1 was adjusted for age, gender, and albumin.
Model 2 was adjusted for covariates from Model 1 and further adjusted for NIHSS and D-dimer.
Model 3 was adjusted for covariates from Model 2 and further adjusted for surgery, GCS, presence IVH, pneumonia, RBC, glucose, BUN, serum calcium, FIB, eGFR, and SUA.
Notes: DVT, deep venous thrombosis; ICH, intracerebral hemorrhage; OR, odds ratio; CI, confidence level; AUC, area under curve; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; FIB, fibrinogen; eGFR, estimated glomerular filtration rate; SUA, serum uric acid.
Incremental Predictive Ability of D-Dimer and Albumin
In the AUC, the P values of the comparison of predictive ability between the new model (conventional model + D-dimer + albumin) and conventional model was 0.06, which was close to statistically significant. Furthermore, in the NRI and IDI, the new model showed a statistical improvement in predicting DVT after adding D-dimer and albumin into the conventional model (both P < .001) (Table 5).
Reclassification and Discrimination Statistics for DVT in Spontaneous ICH Patients.

The conventional model was adjusted for age, gender, surgery, GCS, NIHSS, presence IVH, pneumonia, RBC, glucose, BUN, serum calcium, FIB, eGFR, and SUA.
Notes: DVT, deep venous thrombosis; ICH, intracerebral hemorrhage; CI, confidence level; AUC, area under the curve; NRI, net reclassification improvement; IDI, integrated discrimination improvement; GCS, Glasgow Coma Scale; NIHSS, Institutes of Health Stroke Scale; IVH, intraventricular hemorrhage; RBC, red blood cell; BUN, blood urea nitrogen; FIB, fibrinogen; eGFR, estimated glomerular filtration rate; SUA, serum uric acid.
Discussion
DVT often results in poor outcomes in patients with spontaneous ICH.2,21 Finding relevant predictive markers for spontaneous ICH patients at high DVT risk is vital.1,21 D-dimer and albumin were routine tests and can be obtained in almost all medical institutions. Few articles have systematically studied the relationship between D-dimer, albumin, and DVT in patients with spontaneous ICH. According to our study, the combination of D-dimer and albumin has a good predictability for DVT in spontaneous ICH patients. More attention and further medical care are needed for spontaneous ICH patients with a higher D-dimer or/and lower albumin.
The incidence of DVT in the present study concurs with that reported in the past literature: 22.6% during initial hospitalization in one study and 21% at two weeks in another.22,23 An American retrospective study from 19 centers and 41 sites found that the incidence of VTE was 2%. 24 While, a systemic review showed that the incidence of DVT varied from 10-75% in immobilized post-stroke patients. 25 The differences in racial disparity, drug therapy, the use of elastic stockings, the diagnostic method, and evaluation time may explain this phenomenon.
Some reports have revealed that ICH patients with severe neurologic dysfunction and a higher D-dimer level were more likely to develop DVT.15,26 Cheng et al reported that a high serum D-dimer level was related to DVT in patients with ICH. After adjusting other potential predictive indicators, an elevated plasma level of the D-dimer was found. The plasma D-dimer levels ≥1.20 mg/L were an independent predictor of DVT (OR = 12.99), which was consistent with the present study. 15 However, they had a smaller sample size than that used in this study and excluded dead patients whose cause of death might be due to DVT/pulmonary embolism. Conversely, other research, which was prospective, demonstrated no significant difference in the D-dimer levels upon admission between ICH patients with and without DVT. However, they only included 17 DVT-positive patients and 64 DVT-negative patients. 23 Our study has a much larger sample size. We showed that a high level of D-dimer is a substantial risk factor independently connected to DVT in patients with spontaneous ICH. When the D-dimer value was between 0 and 3.43 mg/L, the risk of DVT increased fast with D-dimer elevation. In contrast, the risk of DVT was relatively steady, with the D-dimer levels of more than 3.43 mg/L. This phenomenon is congruent with our clinical observations, although its precise mechanism remains unknown.
Low serum albumin is a powerful predictor of VTE occurrences in nephrotic syndrome. The risk increases proportionally as the albumin levels decrease. 27 Furthermore, baseline albumin concentrations were collected from 7266 participants with evaluable VTE outcomes in the APEX trial. With decreasing albumin levels, the risk of VTE, asymptomatic proximal deep vein thrombosis, and VTE-related death increased progressively. 19 Neha Bhasin et al found hypoalbuminemia to be extremely frequent in children with venous thrombosis. 28 While, other studies had different results. A recent Japan paper reported no significant differences in albumin levels between ICH patients with or without DVT. 23 Racial differences may be essential when exploring the relationship between albumin and DVT in ICH. To the best of our knowledge, this is the first study to combine D-dimer with albumin to predict DVT in patients with spontaneous ICH.
In addition, consistent with previous studies, our research also found that advanced age and high NIHSS scores were related to DVT in patients with spontaneous ICH.1,2,24
Inevitably, there were several limitations of this research. Given that this was a retrospective observational study, it could not determine if there was a causality relationship between them. Besides, our study was designed to collect data from one hospital, which may lead to selection bias. In the future, more rigorous prospective investigations will be required.
Conclusions
A D-dimer combination with albumin has a good predictability of DVT in spontaneous ICH patients. More attention and further medical care are needed for spontaneous ICH patients with a higher D-dimer or/and lower albumin.
Supplemental Material
sj-docx-1-cat-10.1177_10760296231165054 - Supplemental material for Combination of D-dimer and Albumin in the Prediction of Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage
Supplemental material, sj-docx-1-cat-10.1177_10760296231165054 for Combination of D-dimer and Albumin in the Prediction of Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage by Lingli Chen, MD, Wanli Zhang, MD, and Chunfeng Liu, MD in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
We express our gratitude to all the patients in our study.
Author Contributions
Chunfeng Liu: methodology, data curation, validation, formal analysis, and supervision; Lingli Chen and Wanli Zhang: investigation, data collection, curation, and writing. All authors have read and agreed to the published version of the manuscript.
Ethics Approval
Ethical approval to report this study was obtained from the Human Research and Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (KY2021-R077).
Funding
The present study was supported by the Zhejiang Provincial Natural Science Foundation of China (Grant No. LQ22H020003 to Lingli Chen; Grant No. LQ21H090018 to Wanli Zhang) and Wenzhou's Science and Technology Bureau Project (Grant No. Y2020934 to Lingli Chen)
Informed Consent
Informed consent for patient information to be published in this article was not obtained because this was a retrospective study.
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Conflicts of Interest
The authors declare that the study was conducted without any commercial or financial relationships construed as a potential conflict of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.