
Abstract
Elevated circulating D-dimer levels have been shown to be a predictor of in-hospital mortality in a variety of diseases; however, the relationship between D-dimer and the in-hospital prognosis of non-ST-segment elevation myocardial infarction (NSTEMI) remains unclear. This retrospective study included 662 non-diabetic patients with NSTEMI. Independent risk factors were identified by multivariate analyses, and the receiver operating characteristic (ROC) curve analyses were performed to compare the predictive value of D-dimer, albumin (ALB), and D-dimer to albumin ratio (DAR) for in-hospital death in NSTEMI. Logistic regression model with restricted cubic spline (RCS) was used to further explore the linear or nonlinear relationship between D-dimer and the risk of death. In-hospital mortality occurred in 38 (5.7%) patients. Multivariate analysis showed that D-dimer (per increase of 500 ng) was identified as an independent predictor for in-hospital mortality in non-diabetic patients with NSTEMI (OR = 1.19, 95% CI: 1.03–1.40, P = 0.036). D-dimer demonstrated good predictive performance for in-hospital mortality with an area under the ROC curve (AUC) value of 0.75 (95% CI: 0.66–0.83), and there was no significant difference in the predictive ability of D-dimer, ALB (AUC = 0.70, 95% CI: 0.61–0.79) and DAR (AUC = 0.75, 95% CI: 0.66–0.84). In addition, RCS analysis showed a linear relationship between D-dimer and the risk of in-hospital mortality (P for nonlinear = 0.747). D-dimer can be used as a simple, reliable and valuable biomarker for predicting in-hospital mortality in non-diabetic patients with NSTEMI and is linearly associated with the risk of death.
Introduction
Acute myocardial infarction (AMI) is one of the most common causes of death worldwide. Based on electrocardiogram (ECG) characteristics, AMI can be categorized into ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI). In recent years, with advances in therapeutic techniques, the morbidity and mortality of STEMI have been significantly reduced. 1 However, unlike STEMI, the incidence and hospitalization rates of NSTEMI have shown a rapid increase in recent years, despite a decrease in its in-hospital and out-of-hospital mortality rates.1,2 In China, the rate of NSTEMI admissions was reported to have increased from 0.3 per 100,000 in 2001 to 3.3 per 100,000 in 2011. 3 Worldwide, the in-hospital mortality rate for NSTEMI is 5.1%-6.3%.4–6 Given the high morbidity and catastrophic complications of NSTEMI, there is an urgent need for a parameter that can easily and quickly predict the risk of death in order to allow early risk stratification of patients with NSTEMI, thereby facilitating early intervention and reducing in-hospital mortality.
D-dimer is a soluble fibrin degradation product that is produced in large quantities during thrombosis and activation of the fibrinolytic system.7,8 Thus, elevated circulating levels of D-dimer reflect the occurrence of thrombosis and lysis in vivo and are commonly used for diagnosis and therapeutic monitoring of thrombotic disorders. In recent years, there is growing evidence that elevated D-dimer levels are associated with a poor prognosis in a variety of diseases. D-dimer has been reported to be a strong predictor of in-hospital mortality in patients with infective endocarditis (IE), pulmonary embolism, and acute aortic dissection.9–11
In patients with AMI, rupture of the atherosclerotic plaque exposes subendothelial components to the blood stream leading to thrombosis, and at the same time, the fibrinolytic system is activated, with fibrinolytic enzymes digesting fibrin and producing D-dimer. This process is also accompanied by activation of inflammatory factors. Sakamoto et al. reported the diagnostic value of D-dimer levels in acute aortic dissection, acute pulmonary embolism, and AMI, and although D-dimer was abnormally elevated in patients with all of these disorders, circulating D-dimer levels were significantly lower in patients with AMI compared with the former, which may be related to the small inner diameter of the coronary lumen and the low thrombus load. 12 Huang et al. showed that D-dimer levels could predict adverse cardiovascular events such as death during hospitalization in patients with STEMI. 13 However, the relationship between D-dimer levels and in-hospital mortality in NSTEMI patients has not been elucidated.
We aimed to determine the predictive value of elevated D-dimer levels for in-hospital mortality in non-diabetic patients with NSTEMI and to explore the linear or nonlinear relationship between the two.
Materials and Methods
Study Design
This was a single-center retrospective research. Data for this study were obtained from a publicly available dataset (data available at https://peerj.com/articles/14346), which was shared by Yao et al. 14 The Ethics Committee of Zhongda Hospital affiliated to Southeast University (2020ZDSYLL164-P01) approved the original study, and all authors have waived their copyright to the original research data. For scientific research purposes, we used these data for secondary analysis.
Study Population
The original study included 774 NSTEMI patients without diabetes who were hospitalized in the Department of Cardiology of Zhongda Hospital between March 2012 and December 2018. Inclusion criteria in the original study were (1) age >18 years old and (2) patients with a first diagnosis of AMI, and exclusion criteria were (1) pregnant or breastfeeding women, (2) patients with serious illnesses, such as advanced malignant tumors, and patients with an expected survival time of less than 3 months, and (3) patients with diabetes. 14 In the present study, we further excluded 112 patients with missing D-dimer value (Figure 1). Finally, a total of 662 non-diabetic patients with NSTEMI were included in the present study, including 624 patients who survived to discharge and 38 in-hospital deaths.
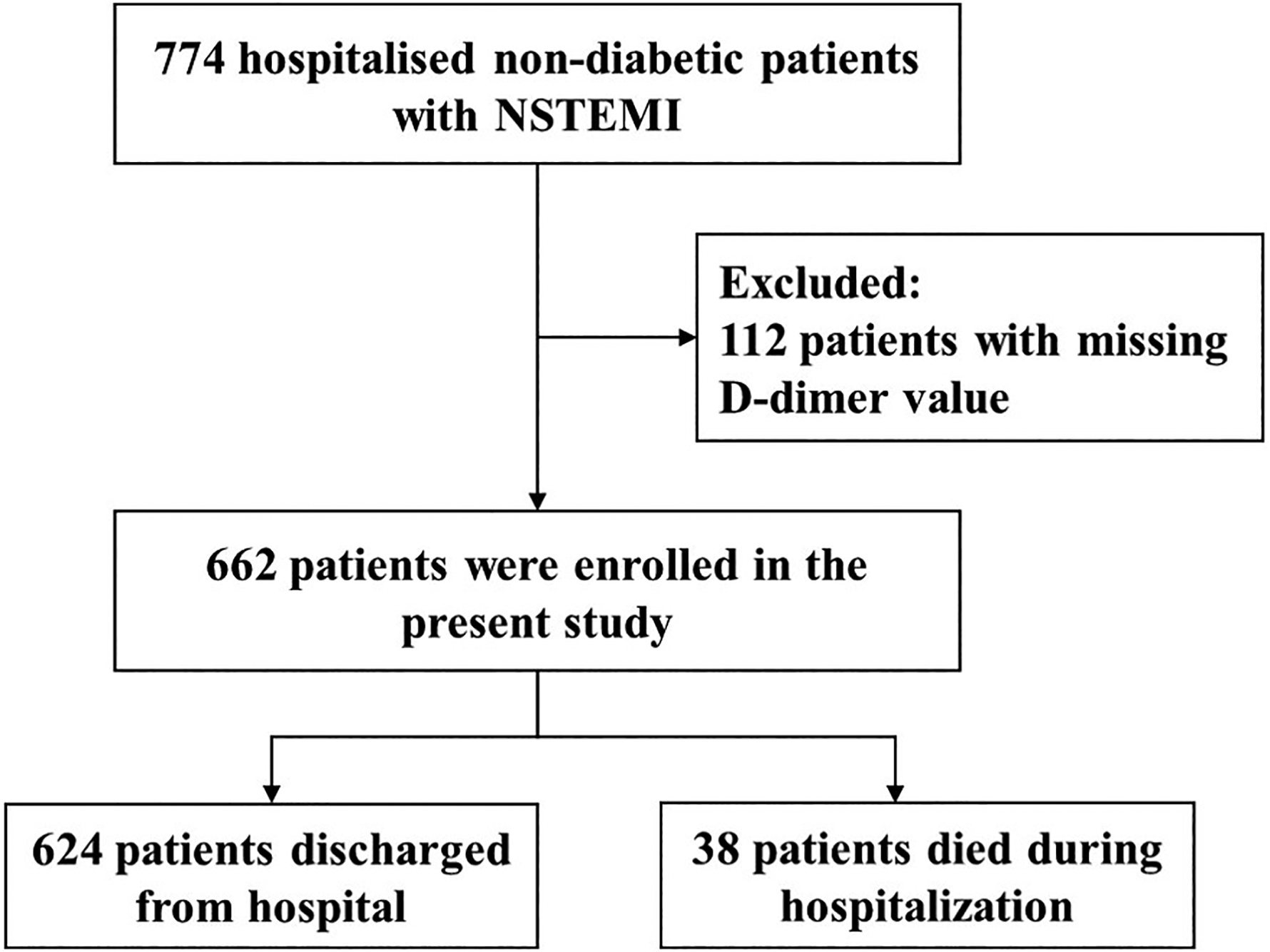
Research flow chart.
Data Collection
Based on literature reports, clinical experience, and availability of variables in the original dataset, we extracted the following variables: age, sex, hypertension, chronic kidney disease (CKD), smoking, alcohol, systolic blood pressure (SBP), diastolic blood pressure (DBP), left ventricular ejected fraction (LVEF), white blood cell (WBC), neutrophil, lymphocyte, monocyte, platelet (PLT), hemoglobin (Hb), D-dimer, alanine aminotransferase (ALT), aspartate aminotransferase (AST), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), total cholesterol (TC), creatinine, cardiac troponin I (cTnI), blood urea nitrogen (BUN), albumin (ALB), glucose (GLU), antihypertensive drug, lipid-lowering drug, aspirin, clopidogrel, nitrate, diuretics and β-blockers. Laboratory indicators were obtained 24 h after admission.
Definitions
NSTEMI was defined as acute myocardial injury detected by abnormal cardiac biomarkers in the presence of evidence of acute myocardial ischemia and without ST-segment elevation on the electrocardiogram at the time of onset. 15 In-hospital death was defined as all-cause death due to cardiovascular and non-cardiovascular disease. 14
Chronic kidney disease (CKD) was defined as estimated glomerular filtration rate less than 60 mL/min per 1·73 m2 or the presence of albuminuria. 16 Hypertension was defined as a blood pressure of ≥140/90 mm Hg or taking antihypertensive drugs. 17
Statistical Analyses
The distributions of all quantitative variables were analyzed using the Shapiro-Wilk test. Following the normality analysis result, all quantitative data were non-normally distributed, presented as median (interquartile range), and compared using the Mann-Whitney test. Categorical variables were presented as counts and percentages, and differences between two groups were compared by the chi-squared test or the Fisher exact test.
The role of D-dimer as an independent predictor of in-hospital mortality in nondiabetic patients with NSTEMI was assessed by univariate and multivariate logistic regression analysis. Receiver operating characteristic (ROC) curve analyses were performed to assess the predictive ability of D-dimer for in-hospital mortality, and the area under the ROC curve (AUC) was calculated to compare the predictive ability of D-dimer, albumin (ALB), and D-dimer to albumin ratio (DAR). Logistic regression model with restricted cubic spline (RCS) was used to further explore the linear or nonlinear relationship between D-dimer and the risk of in-hospital mortality. All the statistical analyses were performed using R software (4.2.2). A p-value <0.05 (two-tailed) or the 95% confidence interval (CI) of the odds ratio excluding the value one was considered statistically significant.
Results
Baseline characteristics
A total of 662 patients were included in this study, 38 (5.7%) of whom died during hospitalization. The baseline characteristics of the participants are presented in Table 1. The median age of the patients was 76 (65–84) years and 209 (31.6%) were female.
Baseline Characteristics of Nondiabetic Patients with NSTEMI.
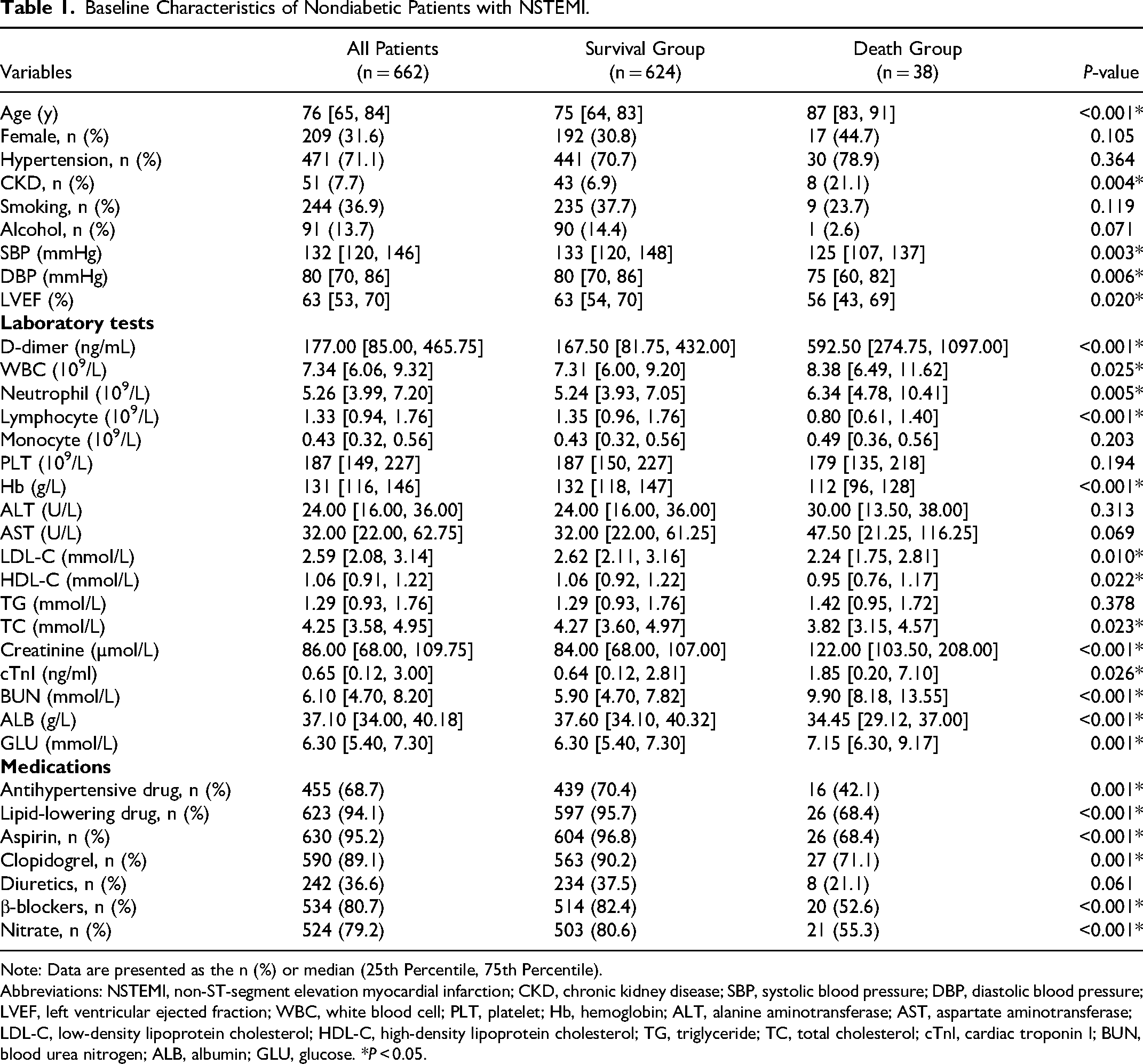
Note: Data are presented as the n (%) or median (25th Percentile, 75th Percentile).
Abbreviations: NSTEMI, non-ST-segment elevation myocardial infarction; CKD, chronic kidney disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; LVEF, left ventricular ejected fraction; WBC, white blood cell; PLT, platelet; Hb, hemoglobin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; TC, total cholesterol; cTnI, cardiac troponin I; BUN, blood urea nitrogen; ALB, albumin; GLU, glucose. *P < 0.05.
Compared with the survival group, patients in the death group were significantly older, more likely to have comorbid CKD, lower systolic and DBP, and worse LVEF (P < 0.05). In terms of laboratory tests, patients in the death group had higher levels of baseline D-dimer, WBC, neutrophil, creatinine, cTnI, BUN, and GLU; and lower levels of lymphocyte, hemoglobin, LDL-C, HDL-C, TC, and ALB (P < 0.05). In terms of medication use, Patients in the death group had significantly lower rates of use of antihypertensive drugs, lipid-lowering drugs, aspirin, clopidogrel, diuretics, nitrate, and β-blockers than those who survived (P < 0.05).
Risk factors associated with in-hospital mortality in nondiabetic patients
Variables with statistically significant differences (P < 0.05) between the two groups in Table 1 were included in the univariate logistic regression analysis and those variables that were statistically significant in the univariate analysis were subsequently included in the multivariate logistic regression model (Table 2). Using multivariate analysis, we identified D-dimer as an independent risk factor for in-hospital mortality in non-diabetic patients with NSTEMI (per increase of 500 ng, OR = 1.19, 95% CI: 1.03–1.40, P = 0.036).
Univariate and Multivariate Logistic Regression Analyses.
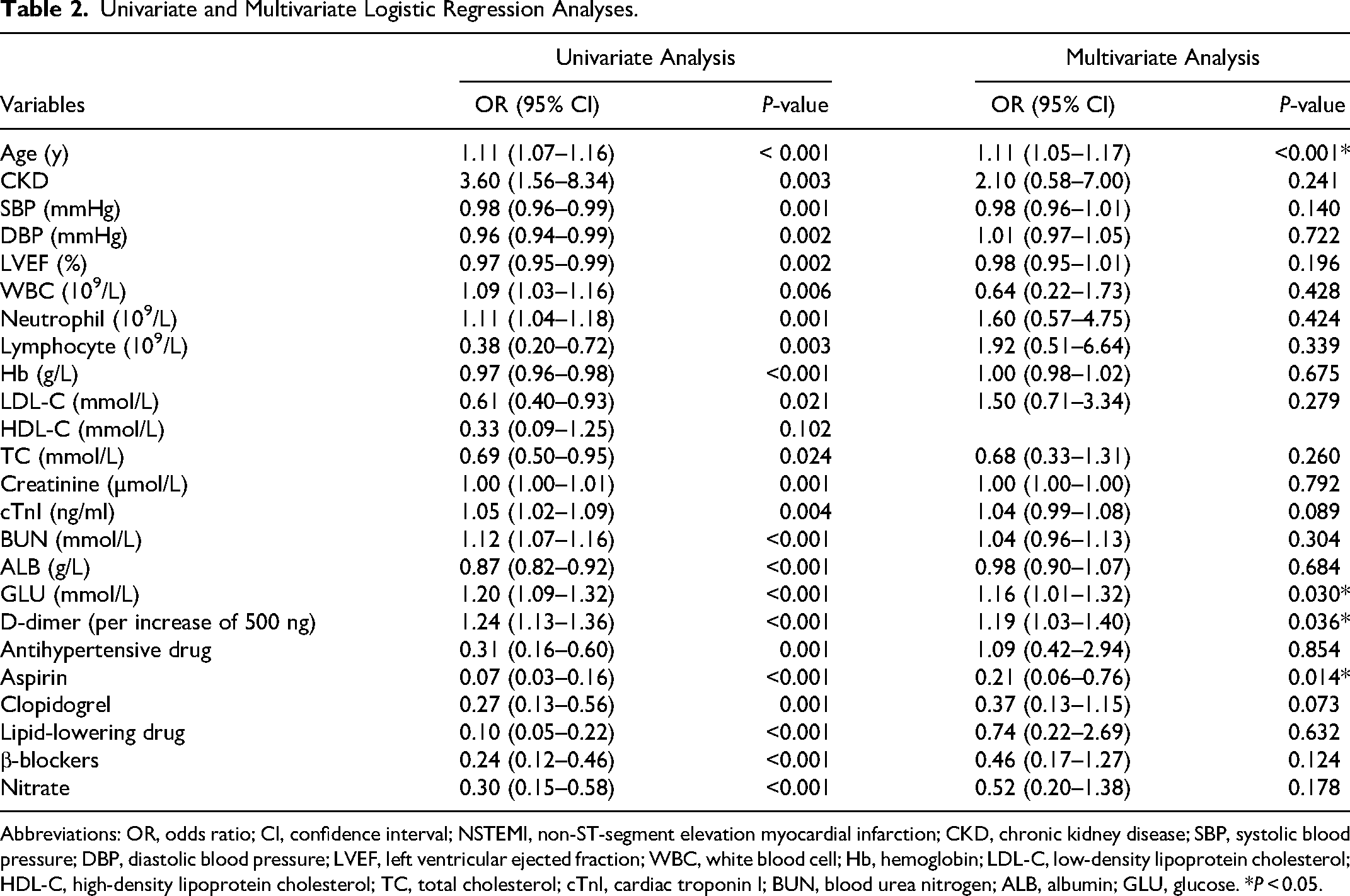
Abbreviations: OR, odds ratio; CI, confidence interval; NSTEMI, non-ST-segment elevation myocardial infarction; CKD, chronic kidney disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; LVEF, left ventricular ejected fraction; WBC, white blood cell; Hb, hemoglobin; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; cTnI, cardiac troponin I; BUN, blood urea nitrogen; ALB, albumin; GLU, glucose. *P < 0.05.
ROC curve analysis
According to the ROC curve, D-dimer demonstrated good predictive ability for in-hospital mortality with the AUC value of 0.75 (95% CI: 0.66–0.83), and the optimal critical value was 221.5 ng/mL, corresponding to a sensitivity of 84.2% and a specificity of 58.8% (Figure 2 and Table 3). Subsequently, we further compared the predictive value of D-dimer, ALB, and DAR for in-hospital death; the AUC values were 0.70 (95% CI: 0.61–0.79) for ALB and 0.75 (95% CI: 0.66–0.84) for DAR, and there was no significant difference in the predictive ability of the three (All DeLong's test P > 0.05).
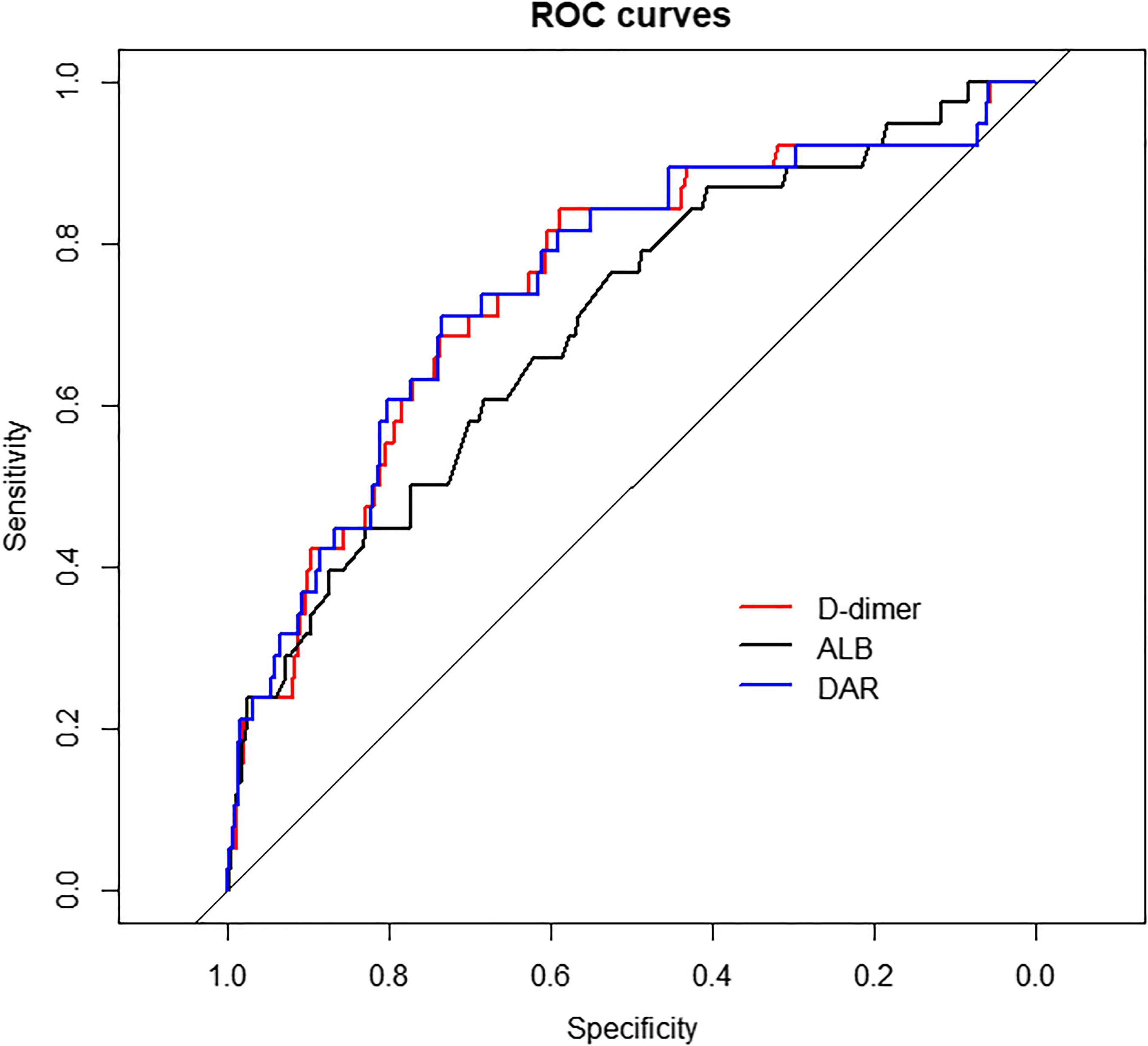
Receiver operating characteristic (ROC) curves for in-hospital mortality. Abbreviations: ALB, albumin; DAR, D-dimer to albumin ratio.
Analyses of the ROC Curve for Predictive Power of In-hospital Mortality.
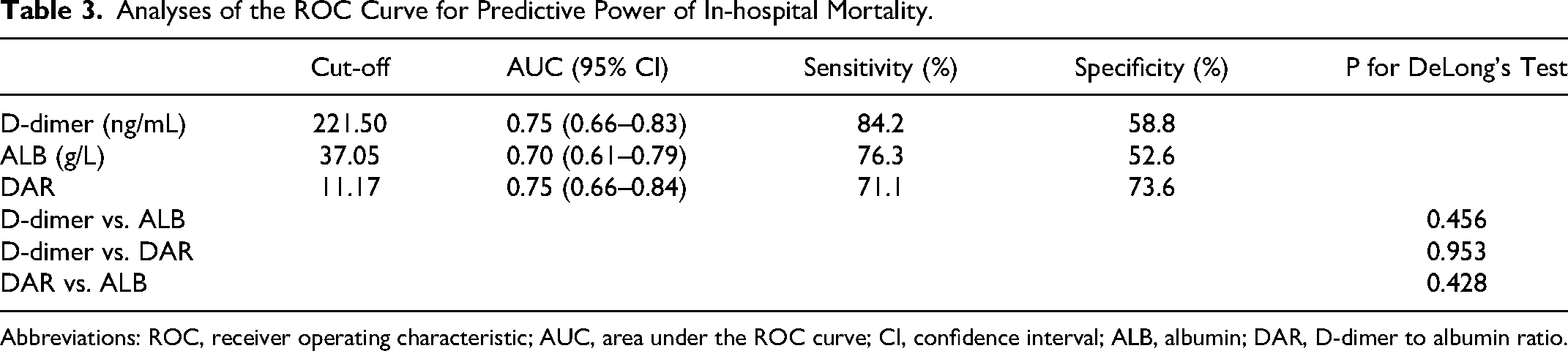
Abbreviations: ROC, receiver operating characteristic; AUC, area under the ROC curve; CI, confidence interval; ALB, albumin; DAR, D-dimer to albumin ratio.
Analysis of the association between D-dimer and in-hospital mortality
To further explore the linear or nonlinear relationship between D-dimer and the risk of in-hospital death, multivariable-adjusted (adjusted for age, GLU and aspirin) RCS model based on logistic regression was performed (Figure 3). RCS analysis showed a positive linear association between D-dimer and in-hospital mortality in nondiabetic patients with NSTEMI (nonlinear P = 0.747).
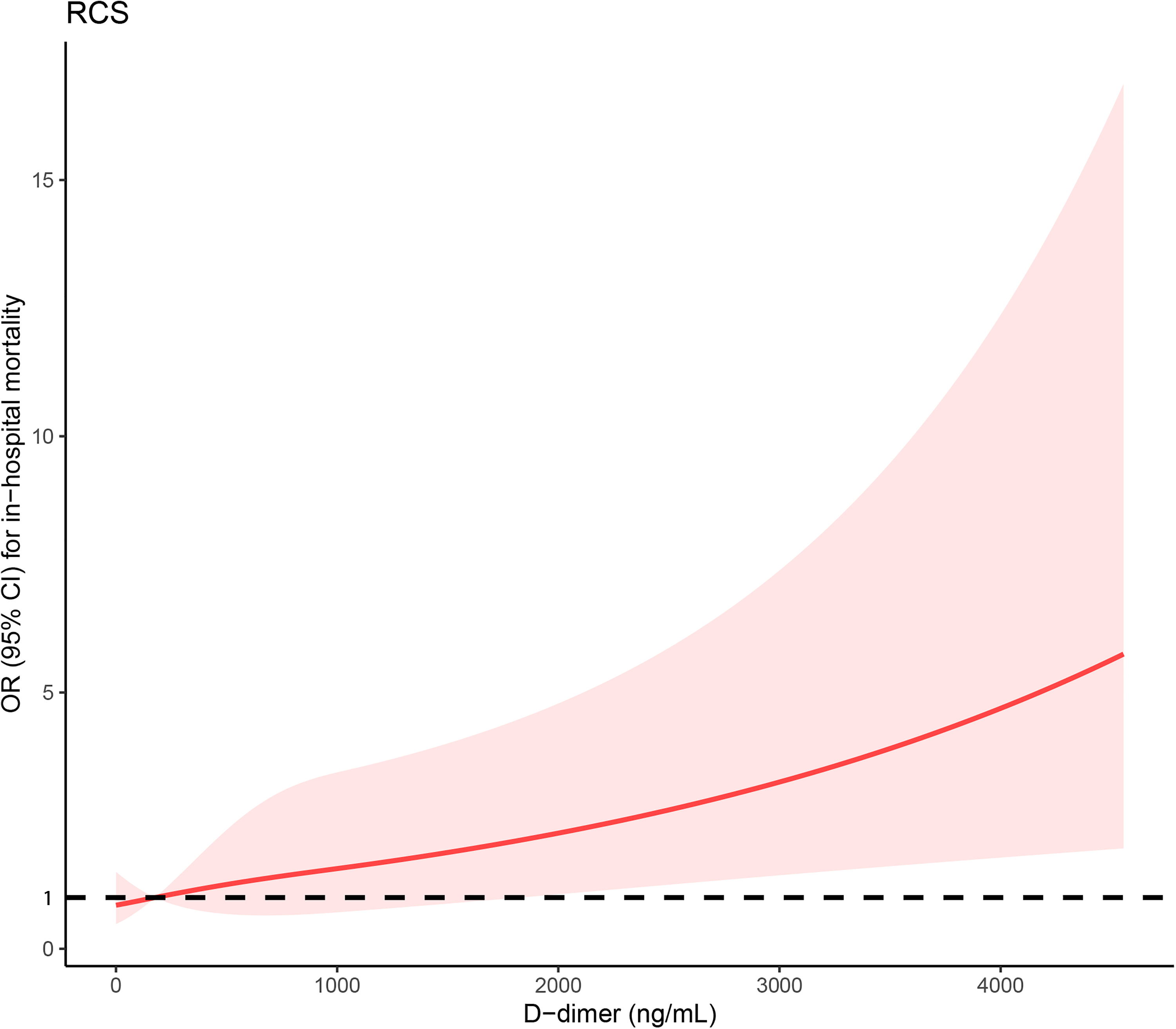
The restricted cubic spline (RCS) regression between D-dimer and in-hospital mortality in nondiabetic patients with NSTEMI.
Discussion
To our knowledge, this study is the first to investigate the relationship between D-dimer and in-hospital mortality in non-diabetic patients with NSTEMI. The main findings of this study can be summarized as follows: (1) We demonstrated for the first time that elevated D-dimer levels on admission were an independent risk factor for in-hospital mortality in non-diabetic patients with NSTEMI, and that this association was independent of traditional clinical factors and usual biomarkers; (2) Although there was no significant difference in the predictive ability of DAR, ALB, and D-dimer for in-hospital death, considering that ALB is not an independent predictor of in-hospital death, we only recommend D-dimer as an identifier of mortality risk; (3) There was a linear relationship between D-dimer and the risk of in-hospital death, suggesting that monitoring D-dimer levels could help with risk stratification and early identification of those at high risk of in-hospital death.
D-dimer is a degradation product of cross-linked fibrin and reflects activation of coagulation and fibrinolysis. 18 In the past, D-dimer was commonly used to rule out and diagnose thromboembolism and acute aortic dissection,19,20 and several studies have shown that D-dimer is also an inflammatory marker that is strongly associated with the development of inflammatory diseases.21,22
NSTEMI is a common type of AMI, the incidence of which has shown a rapid increase in recent years. Despite advances in medical diagnosis and treatment, the short- and long-term prognosis of NSTEMI remains poor. 23 In terms of pathogenesis, NSTEMI is caused by rupture of atherosclerotic plaques leading to thrombosis and impaired coronary blood flow, which is accompanied by activation of the fibrinolytic system and massive fibrin degradation in the process, leading to a rapid increase in D-dimer levels. In this study, we found that NSTEMI patients without diabetes who died in-hospital had significantly higher D-dimer levels than survivors (P < 0.001).
Recent studies have emphasized the promise of elevated D-dimer as a poor prognostic biomarker for patients with a range of diseases. A small study that included 79 patients with IE demonstrated that high D-dimer is a prognostic marker for predicting in-hospital mortality in patients with IE. 9 The results of a French multicenter study that included 1154 patients with COVID-19 support the use of elevated D-dimer as a predictor of in-hospital mortality in patients. 24 In addition, other studies have reported an association between elevated D-dimer and adverse outcomes in different diseases.25,26 However, the value of D-dimer in assessing the in-hospital prognosis of patients with NSTEMI remains unclear. Therefore, we herein investigated the predictive value of D-dimer for in-hospital death in patients with NSTEMI.
In this study, we report for the first time the independent predictive value of abnormally elevated D-dimer for in-hospital death in non-diabetic patients with NSTEMI. By ROC curve analysis, we determined the good predictive power of D-dimer. Low serum albumin is associated with poor prognosis in cardiovascular disease. NSTEMI may be accompanied by a hypercoagulable state, which may lead to an increase in D-dimer and a decrease in albumin. Some studies have reported the predictive value of DAR for the prognosis of different diseases,27–29 and in our study, we found that there was no significant difference in the predictive ability of DAR, ALB, and D-dimer for in-hospital death in NSTEMI. Considering that ALB was not an independent risk factor in the multivariate analysis and the simplicity of clinical application, we recommend D-dimer as an independent predictor of in-hospital death in NSTEMI. RCS analysis confirmed the linear relationship between D-dimer and hospital death. With the increase of D-dimer level, the risk of hospital death gradually increased, which further demonstrated that D-dimer is a strong predictor of hospital death in NSTEMI patients with non diabetes. There are several mechanisms that can explain the predictive value of D-dimer for hospital death in NSTEMI patients without diabetes. Firstly, as an inflammatory marker, the elevated level of D-dimer reflects the high inflammatory state of the body, and inflammation plays an important role in the progression and prognosis of AMI.30,31 Secondly, as a breakdown product of fibrin, higher levels of D-dimer can cause blood to become viscous, which may further exacerbate myocardial infarction. The results of these analyses suggest that D-dimer can be used for risk stratification of non-diabetic patients with NSTEMI and the development of different intervention strategies accordingly, with the aim of reducing the risk of in-hospital death in non-diabetic patients with NSTEMI.
This study also has some limitations. First, this study is a secondary analysis based on the original study, and given that the original study was retrospective, there may have been some confounding factors that were not included. Secondly, our study only explored the predictive value of D-dimer levels on admission for in-hospital death in non-diabetic patients with NSTEMI and did not analyze the dynamics of D-dimer concentrations at different time points during hospitalization as well as the D-dimer maxima, which could potentially provide greater value in the in-hospital prognostic assessment of non-diabetic patients with NSTEMI. Finally, the sample size of this study was relatively small, and large multicenter prospective cohort studies will be needed in the future to confirm our findings.
Conclusions
In conclusion, D-dimer on admission can be used as a novel biomarker to assess the risk of in-hospital mortality in non-diabetic patients with NSTEMI, which is linearly and positively correlated with the risk of death.
Footnotes
Acknowledgments
The authors thank Dr. Yao from Zhongda Hospital affiliated to Southeast University for sharing the data.
Author contributions
Yujie Zhao designed the study. Bin Li wrote the manuscript, which was revised and statistically supervised by Wensen Yao. Xiaojing Liu, Miaomiao Gao and Lin Ma participated in the analysis of the data.
Disclosure
The authors report no conflicts of interest in this work.
Ethics approval
The Ethics Committee of Zhongda Hospital affiliated to Southeast University (2020ZDSYLL164-P01) approved the original study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This study was supported by Henan Key Laboratory of Cardiac Remodeling and Transplantation; Henan Provincial Science and Technology Key Research and Development Project (222102310667); Zhengzhou Science and Technology Benefit People Project (2022KJHM0033); Zhengzhou Second-tier Famous Doctor Support Special Project in 2021 (15). There was no additional external funding received for this study. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.