
Abstract
Lung cancer is the leading cause of cancer-related mortality worldwide with an increasing incidence in many countries. There were few studies on arterial and venous thromboembolism (ATE/VTE) in patients with metastatic lung cancer. Our study focused on the clinical characteristics of stage IV lung cancer patients with ATE or VTE to further explore the risk factors and prognosis. Patients diagnosed with metastatic lung cancer were enrolled from January 2011 to June 2019 at a tertiary hospital in Jiangyin, China. Log-rank test was used to reveal the survival for patients with ATE or VTE. Univariable analysis and multivariable logistic regression were used to study the risk factors for ATE. A total of 587 patients were enrolled in our study, including 52 patients with VTE and 48 with ATE. ATE occurred earlier than VTE. Patients with ATE had a worse prognosis. Multivariable logistic regression revealed that older age and a history of hypertension were independent risk factors for ATE. Patients with metastatic lung cancer were at high risk of VTE and ATE. ATE occurred earlier and was associated with a worse prognosis. Attention should be paid to metastatic lung cancer patients who may develop thromboembolism, especially ATE.
Introduction
In 1865, Armand Trousseau first described the relationship between thrombosis and cancer. There is an increased risk of venous and arterial thromboembolism (VTE/ATE) in cancer patients. 1 VTE mainly includes deep vein thrombosis (DVT), pulmonary embolism (PE) and splanchnic vein thrombosis (SVT).2,3 Compared with the general population or patients without cancer, cancer patients have a several-fold increased risk of VTE, with relative risks ranging from 4 to 7. 4 ATE comprises acute coronary syndrome (ACS), ischemic stroke and acute peripheral artery occlusion. 5 Previous studies have reported an increased risk of stroke and ACS in patients with cancer.6,7
Compared with the decreasing incidence in some western countries, the incidence of lung cancer is still increasing in China. 8 And lung cancer is the leading cause of cancer-related mortality worldwide. Improved treatment accelerates progress in lung cancer. For example, the 2-year relative survival for non-small cell lung cancer (NSCLC) increased from 34% during 2009 through 2010 to 42% during 2015 through 2016. 9 A study from the Surveillance, Epidemiology, and End Results program reported that the 5-year survival of lung cancer rose from 15.6% in 2011 to 19.4% in 2019. Coupled with the fact that most patients with lung cancer are in the advanced stage at the time of diagnosis, the number of metastatic lung cancer patients is huge. 10 The quality of life of this group deserves our attention. The relative risk of VTE in lung cancer patients is surpassed only by pancreas, brain, stomach, and ovarian cancers. 11 The occurrence of VTE increases the mortality of lung cancer patients, 12 seriously affects the quality of life, and aggravates the medical burden of patients. 13 A study has documented that lung cancer was associated with a higher ATE risk. 5 And a large retrospective cohort study showed that the incidence of ATE at 6 months in lung cancer patients was 8.3%. 14 However, there were few articles that analyzed ATE in patients with lung cancer, especially stage IV lung cancer.
In the present study, we sought to identify the clinical characteristics and the prognosis of VTE and ATE in Chinese patients with metastatic lung cancer.
Methods
Study Design
We conducted a single-center retrospective study of patients with metastatic lung cancer at the time of diagnosis who were admitted consecutively to Jiangyin People's Hospital from January 2011 to June 2019. All eligible patients were selected according to the inclusion and exclusion criteria. The detailed protocol has been approved by the institutional Ethics committee of Jiangyin People's Hospital.
Patients Selected
Inclusion criteria: (1) over 18 years of age; (2) a histopathological diagnosis of primary lung cancer at stage IV 15 ; (3) intact medical records in the oncology department.
Exclusion criteria: (1) a history of other malignancy; (2) lung cancer-unrelated surgery within the last 3 months; (3) severe infection and trauma within the last 6 weeks; (4) a history of the thromboembolic event; (5) patients with an indication for prophylactic or therapeutic anti-coagulation or anti-platelet therapy within 3 months prior to VTE or ATE; (6) loss to follow-up.
Data Collection
Data on baseline demographics, comorbidities, laboratory and imaging data, and information about tumor and treatment were collected through the electronic record system. Tumor histopathology was divided into NSCLC and small cell lung cancer (SCLC). Laboratory data including leukocyte, platelet, hemoglobin, and D-dimer were collected. DVT events were mainly confirmed by Doppler ultrasonography. PE events were confirmed by computed tomography (CT) or pulmonary angiography. SVT events were confirmed by CT angiography. ACS events were confirmed by cardiac biomarkers, electrocardiography, echocardiography, and coronary angiography. Ischemic stroke events were confirmed by CT and magnetic resonance imaging (MRI). Follow-up for thromboembolic events started from the diagnosis of metastatic lung cancer and ended on June 30, 2021. The follow-up items included the history of tumor treatment and VTE, and the follow-up data were mainly from outpatient medical records, inpatient medical records, and doctors’ follow-up telephone records.
Statistical Methods
Descriptive analyses were used to describe baseline variables of patients with metastatic lung cancer and the number of VTE and ATE events. Results were given as median and ranges, absolute frequencies and percentages, or mean and standard deviations (SD). Median follow-up time was estimated by the reverse Kaplan–Meier method. The risk factors for ATE were investigated by univariable and multivariable analysis. Chi-square test was used for univariable analysis. To avoid missing important factors, variables with P < .2 in the univariable analysis were included in the multivariable logistic regression analysis. Multivariable logistic regression analysis further confirmed the risk factors for metastatic lung cancer patients with ATE. Median occurrence and survival time of VTE and ATE were calculated using the Kaplan–Meier method. Log-rank test was used to compare the curves of the 3 groups. All statistical analyses were performed using SPSS software, version 26.0 for Mac. Pictures were drawn by GraphPad Prism 9.0 for Mac. Statistical significance was set at two-side P < .05.
Results
Characteristics of the Study Population
A total of 587 patients diagnosed with metastatic lung cancer were enrolled in this study from January 2011 to June 2019. The median age of this group was 65 years (24-94 years), and 67.3% (395/587) were male. The average BMI was 22.29 (SD 3.05) kg/m2 with a range of 13.96 to 31.11 kg/m2. 33.2% (195/587) of patients had a certain history of smoking. 496 (84.5%) patients had a performance status of 0 or 1. With regard to comorbidities, 193 (32.9%), 33 (5.6%), and 19 (3.24%) patients had a history of hypertension, diabetes mellitus, and atrial fibrillation, respectively. The main pathological type was NSCLC (85.3%, 501/587). Of the 3 treatments included in this study, chemotherapy (76.7%, 450/587) accounted for the majority. Details on the characteristics of the 587 patients were shown in Table 1.
Clinical Characteristics of the 587 Patients With Stage IV Lung Cancer, Median (Range)/Count (%)/Mean (SD).

Abbreviations
SD: standard deviation
BMI: body mass index
NSCLC: non-small cell lung cancer
SCLC: small cell lung cancer
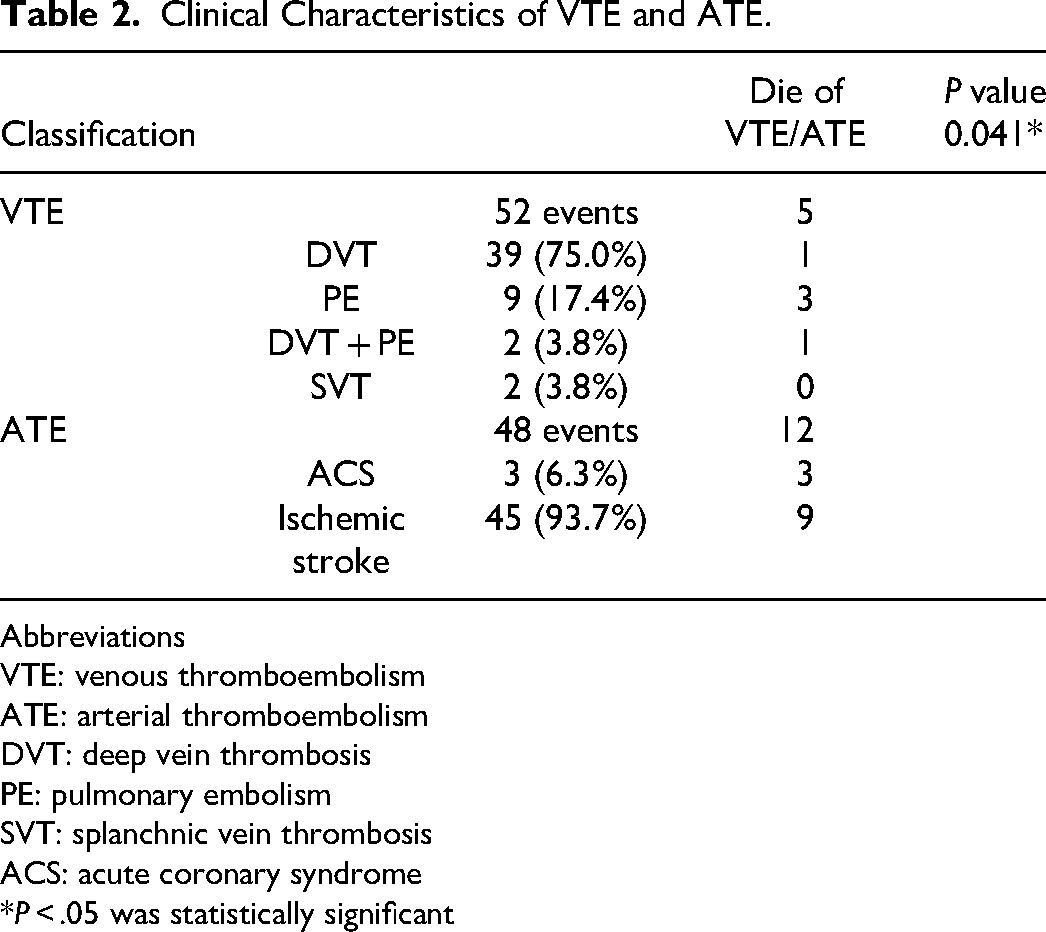
Patients with stage IV lung cancer in our research had a higher incidence of VTE and ATE, 8.86% and 8.18% than people without cancer. 16 Over a median follow-up of 14 months, 100 patients developed thromboembolism. 52 patients had VTE. Among them, 39 cases had DVT, 9 cases had PE, 2 cases had both DVT and PE, and 2 cases had SVT. 48 patients developed ATE, including 3 cases with ACS and 45 cases with ischemic stroke. No patient had both clinical VTE and ATE. Details were shown in Table 2.
Clinical Characteristics of VTE and ATE.
Abbreviations
VTE: venous thromboembolism
ATE: arterial thromboembolism
DVT: deep vein thrombosis
PE: pulmonary embolism
SVT: splanchnic vein thrombosis
ACS: acute coronary syndrome
*P < .05 was statistically significant
Comparisons of ATE and VTE in Occurrence and Survival
Figure 1 showed that ATE occurred earlier than VTE (P = .012). Median occurrence time of VTE was 4 months and that of ATE was 2 months.

Occurrence time for patients with ATE and VTE.
During the follow-up period, 556 deaths were observed. Median overall survival (OS) of 587 patients was 12 (95% CI: 10.636-13.364) months. For patients with ATE, the median OS was 7 (95% CI: 4.093-9.907) months. Median OS of patients with VTE was 9 (95% CI: 5.861-12.139) months. And for patients without VTE or ATE, the median OS was 13 (95% CI: 11.539-14.461) months (P = .002) (Figure 2). For further pairwise comparisons, the P-value level was adjusted to .0167. Median OS of patients with ATE was shorter than those without VTE/ATE (P < .001), while OS of patients with VTE and without VTE/ATE was not statistically significant (P = .978).

Os for patients with ATE, VTE and without VTE/ATE.
As for deaths directly caused by thromboembolism, there were 5 (29.41%) deaths caused by VTE and 12 (70.59%) deaths caused by ATE, which seemed to be more fatal (P = .041) (Table 2).
Risk Factors for ATE in Stage IV Lung Cancer Patients
Our research showed that compared with VTE, ATE occurred earlier, and had a worse survival. That was the reason why we further studied the risk factors for ATE. Among the 587 patients, 48 (8.18%) ATE events were observed. Table 3 showed the univariable analysis of potential risk factors for ATE. There were 2 factors with statistical significance: age and hypertension. ATE was more common in older patients. Patients with a history of hypertension were more likely to develop ATE. Table 4 showed the multivariate regression results. Age ≥65 years (vs age <65 years; OR: 2.603; 95% CI: 1.328-5.100; P = .005), and with a history of hypertension (vs without a history of hypertension; OR: 1.947; 95% CI: 1.057-3.585; P = .033) were associated with significantly greater odds of having ATE in stage IV lung cancer patients.
Univariable Analysis for the Stage IV Lung Cancer Patients With ATE.

Abbreviations
ATE: arterial thromboembolism
BMI: body mass index
NSCLC: non-small cell lung cancer
SCLC: small cell lung cancer
*P < 0.05 was statistically significant
Multivariable Logistic Regression for the Stage IV Lung Cancer Patients with ATE.

Abbreviations
ATE: arterial thromboembolism
OR: odds ratio
CI: confidence interval
*P < .05 was statistically significant
Discussion
As a country with a large population, and with the development of cancer treatment, there are a large number of patients with stage IV lung cancer in China. As a common complication of lung cancer, thrombosis deserves our attention. Although there are more and more studies exploring the relationship between cancer and ATE nowadays, few articles have examined the relationship between ATE and lung cancer, especially metastatic lung cancer. We mainly studied the relationship between metastatic lung cancer and thrombosis, especially ATE. Such articles were rare.
In our study, patients with stage IV lung cancer had a higher incidence of VTE and ATE. The incidence of VTE and ATE was 8.86% and 8.18%, respectively. The incidences of VTE in patients with lung cancer vary in previous retrospective studies. According to an earlier study, the 2-year cumulative incidence of VTE in California and Taiwan was 3.4% and 1.52%, respectively. 17 In 2014, Riedl et al reported that in their study, the incidence of VTE was 6.8% in patients with all stages lung cancer. 18 A large retrospective study based on the SEER-Medicare linked database showed that the incidence of ATE at 6 months and 1-year in patients with lung cancer was 8.3% and 10.3%, respectively. And compared with breast, prostate, colorectal, bladder, pancreatic or gastric cancer or non-Hodgkin lymphoma, lung cancer patients had the highest 6-month cumulative incidence of myocardial infarction (3.2%) and ischemic stroke (5.6%). 19 A retrospective study reported the incidence of VTE in nonmetastatic lung cancer patients was 1.25% (33/2630), greatly lower than that in patients with metastatic lung cancer in our study. 20 A real-world study from Japan confirmed that patients with active cancer had a higher risk for VTE, this may be one reason for the higher incidence of VTE in our study. 21 The incidence of ATE was also higher in patients with advanced stage cancer. 19 However, there were few studies reported the incidence of ATE in different stages of lung cancer. Therefore, for this group of patients, effective measures should be taken to diagnose thrombosis earlier, and anticoagulant therapy should be used when necessary.
Our study showed that ATE occurred earlier than VTE in patients with metastatic lung cancer. The relationship between the occurrence time of ATE and VTE in cancer patients had rarely been researched. Our result will provide a valuable piece of information for clinical work. Most VTE events occurred within the first 6 months after cancer diagnosis, 22 meaning that VTE occurred early in cancer patients. In our research work, the median occurrence time of VTE was 4 months and that of ATE was only 2 months. Risk factors for cancer-associated thrombosis include patient-related features, treatment-related features, and cancer-related features. 23 Our study found that older patients or those with a history of hypertension were prone to develop ATE events. While there was insufficient data on the risk of ATE, we do not yet know whether treatment will lead to ATE. 5 We did not further investigate risk factors for VTE. Previous studies had shown that treatment in lung cancer patients including erythropoiesis-stimulating agents, chemotherapy, targeted therapy, and use of central venous catheters may increase the risk for VTE.24,25 This may explain why VTE occurred later than ATE in our study.
We found that ATE not only occurred earlier than VTE, but also had a worse prognosis compared to those without VTE/ATE. Although median OS of patients with ATE and VTE was not statistically significant in our study, there was a trend that the occurrence of ATE was associated with shorter OS (P = .017). A study included 1880 patients with lung, breast, colorectal, prostate, stomach, and other cancers showed that the occurrence of ATE had a 3.2-fold higher risk of mortality, and the median OS after ATE in this study was only 63 days. 5 Similarly, Navi et al found a 3.1-fold increased risk of death in cancer patients who had ATE events by analyzing the SEER database. 19 In 2020, Japanese researchers carried out a retrospective study of 1471 lung cancer patients, and 28 patients developed VTE. The median survival time after VTE was 135 days in this study. 26 Khorana et al once conducted a prospective study about the causes of death in 4466 patients with cancer undergoing chemotherapy. 141 deaths were observed, ATE was the cause of death in 5.6% (n = 8), and that of VTE was 3.5% (n = 5). 27 And in our study, we observed 12 out of 48 ATE and 5 out of 52 VTE deaths due to thrombosis, respectively. It suggested that ATE was more lethal than VTE. Although there was no study comparing the survival time of ATE and VTE in the cohort of lung cancer patients, it can be inferred from the above studies that ATE posed a greater threat to death in cancer patients than VTE. As to the reasons for the worse prognosis of ATE than VTE, we made the following hypotheses. One of the reasons is that ATE occurs earlier than VTE, which affects the subsequent treatment of patients earlier. Second, American Society of Clinical Oncology (ASCO) has published clinical practice guideline recommendations for thromboprophylaxis in cancer patients. Treatment of VTE is well known, including anticoagulant drugs (low molecular weight heparin, warfarin, rivaroxaban, and so on) and implantation of inferior vena cava filters.1,28,29 In contrast, the treatment of ATE has been poorly studied. In our study, ATE was mainly composed of ischemic stroke, which would reduce the quality of life of patients and affect subsequent therapy, thus worsening the prognosis, while VTE patients could continue to receive antitumor therapy after appropriate anticoagulant therapy.
Our study confirmed that older age and a history of hypertension were risk factors for ATE. This finding is consistent with previous studies.5,30 It is well known that age and hypertension are classic cardiovascular risk factors, while ATE is mainly composed of cardiovascular and cerebrovascular events, which may explain the increased rate of ATE in this population. Because of hidden symptoms and poor prognosis in some ATE events, it is particularly important to identify patients at high risk of ATE and improve prevention, diagnosis, and treatment strategies in clinical works.
There are some limitations to our study. First of all, it was a single-center retrospective study with a small number of patients and may not be representative. Moreover, most VTE and ATE events in our study were symptomatic, and the actual incidence may be underestimated, which may bias our results. Lastly, due to the limitations of the retrospective study, we did not further clarify the sequence of thromboembolism and treatment, that is the reason why we did not include treatment in the risk factor study for ATE. In the future, we will conduct a prospective study to further verify and extend our findings.
Footnotes
Acknowledgments
None to declare.
Authors’ Contributions
YQ and LZ: substantial contribution to the design of this research, data acquisition, statistical analysis, and manuscript drafting; XL and XS: substantial contribution to the data collection and the statistical analysis; NW and MY: substantial contribution to the data collection; QW and DW: substantial contribution to the conception of the research and critical manuscript revision. All authors read and approved the final manuscript.
Conflict of Interest
None declared.
Data Availability
The authors declare that the data supporting the findings of this study are available in this manuscript.
Ethics Approval
Ethical approval to report this case was obtained from the institutional Ethics committee of Jiangyin People's Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by grants from the General project of Wuxi Municipal Health Commission (No. MS201908).
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.