
Abstract
There are classical risk factors associated with arterial thrombosis (AT) or venous thromboembolic disease (VTD). However, less is known about these risk factors and AT or VTD episodes in patients with antiphospholipid syndrome (APS). Our aim was to elucidate whether APS-related thrombotic episodes are associated with the same risk factors as the non-APS population. We gathered demographics, medical history, complications, and causes of death associated with the risk factors for AT or VTD in patients with APS. We analyzed 677 thrombotic events in 386 patients. Type 2 diabetes mellitus and grade 3 obesity were associated with VTD instead of AT. There were no significant differences between the groups for almost all laboratory tests analyzed, although lupus anticoagulant was significantly higher in the VTD group. We suggest that thrombosis in APS is due to the APS itself and that the risks factors for AT or VTD do not have a main role. Our findings may have an ethnical background. Therefore, it may be difficult to elaborate predictive thrombotic clinical scores applicable to patients with different ethnical background.
Keywords
Introduction
Antiphospholipid antibodies (aPL), including lupus anticoagulant (LA), immunoglobulin (Ig) G and IgM anticardiolipin antibodies (aCL), and anti-β2-glycoprotein-1 antibodies (anti-β2-GP1), are associated with an increased risk of arterial thrombosis (AT) and venous thromboembolism (VTD). 1 The aPL may appear as the “classical” antiphospholipid syndrome (APS) in a patient with recurrent thrombosis or fetal loss and as asymptomatic “carrier” patients for aPL and patients with positive tests for aPL. The APS is an autoimmune prothrombotic clinical condition characterized by the occurrence of aPL and recurrent pregnancy morbidity and/or thrombotic events. The APS can be found in patients having neither clinical nor laboratory evidence of another clinically established condition (primary APS), or it may be associated with other diseases, for example, lymphoproliferative diseases, cancer, 2 autoimmunity, 1 infections, 3 and drugs. 1 Some other clinical abnormalities associated with APS are hematological, mainly thrombocytopenia or Coomb-positive hemolytic anemia, or livedo reticularis, 4,5 but thrombotic manifestations are absent. In a few patients, the APS appears as a life-threatening event called catastrophic APS characterized by rapid development of microthrombosis leading to a fast multiorgan failure. 6
The exact pathogenic mechanism underlying the aPL-mediated thrombosis is still a matter of debate. Despite the strong association between aPL and thrombosis, less is known about the pathogenic role of aPL in the development of these complications. Evidence shows that several APS-associated autoantibodies are directed against plasma proteins and proteins expressed on, or bound to, the platelet or endothelial surface. It is likely that aPL may interfere either with the normal processes of hemostatic and/or anticoagulant reactions or on the expression or secretion of cell-mediated mediators of the normal blood coagulation system. 7,8
Thrombosis is the leading cause of mortality worldwide, and there is a body of evidence demonstrating the association between specific or classical risk factors and the pathophysiological mechanisms leading to the occurrence of AT or VTD events. However, less is known about the association of these risk factors and the appearance of AT or VTD episodes in the population with APS. Therefore, the aim of this research was to elucidate whether AT or VTD in patients with APS is also associated with the classical risk factors as that occurs in the non-APS population.
Materials and Methods
In this cohort study, we performed an observational, prospective, comparative analysis of patients, both women and men, who fulfilled the international criteria for APS. We reviewed the clinical charts and databases of patients who attended our hospitals from January 1998 to December 2015. From all patients, we gathered demographic, medical history, information regarding the presence of the accepted classical risk factors for AT or VTD in the general population, and laboratory data. These data were obtained when the thrombotic event defining the APS diagnosis occurred or, in some of them, when a new thrombotic event appeared. During the follow-up period, we obtained information about complications and causes of death.
Sample Selection
At diagnosis, all participants must have at least 1 arterial or venous thrombotic event with 1 or more positive tests for aPL, namely, LA or ACL antibodies. Patients with primary or secondary APS were included. Bridging with low-molecular-weight heparin or rivaroxaban was indicated in those patients using vitamin K antagonists before obtaining blood samples in order to have appropriate plasma samples for the coagulation assays. Aspirin was never suspended.
Clinical Assessment
From each patient, the following clinical variables were obtained either at the moment of the APS-defining thrombotic event or, when applicable, when a new thrombotic episode was recorded: age, age at first thrombotic event, height and weight, abdominal circumference (AC), body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP). Patients were considered as having high blood pressure when they fulfilled the Joint National Committee (JNC) VIII criteria; 9 diagnosis of type 2 diabetes mellitus was established according to the 2015 criteria of the American Diabetes Association; 10 diagnosis of dyslipidemia was based on the 2002 criteria of the Adult Treatment Panel (ATP) III. 11 Of course, in diagnosis of APS or when a new thrombotic episode was recorded, none of the patients was under treatment for dyslipidemia. We also recorded the site(s) of thrombosis in order to classify the patients in 1 of 3 groups: AT, VTD, or AT/VTD (patients having both types of thrombosis). Information about history of cancer, smoking, or hormonal use as well as concomitant known diseases; the immediate antecedent of surgery, trauma, pregnancy, or puerperium; and prolonged hospitalization, intensive care unit hospitalization, and prolonged immobilization or traveling was gathered. Moreover, we obtained data about family history of early age arterial or venous thrombotic events. In those patients with AT, we specifically search for the history of chronic symptoms of heart, cerebral, or peripheral ischemia. In women, we also investigated about history of early severe eclampsia.
Sample Collection
Blood samples were collected immediately after diagnosis of APS or when a new thrombotic episode occurred. We collected 22 mL of blood from each patient in 2 vacuum tubes without anticoagulant (Vacutainer, Beckton Dickinson, Rutherford, New Jersey), 1 tube with EDTA (Vacutainer), and 2 tubes with 3.2% trisodium citrate (vol:vol = 1:9; Vacutainer). Samples were centrifuged immediately after collection at 2500 × g for 15 minutes, and platelet-poor plasma and serum samples were obtained using a disposable Pasteur pipette. All aliquots were prepared using 2-mL Eppendorf tubes and immediately frozen at −70°C until processing. Serum and plasma samples were always analyzed after collecting the last sample. For quality control tests, we used commercially available serum and plasma controls. Blood samples were never obtained in pregnant women, and, if necessary, assays were performed in these patients 3 months after childbirth.
Assays
We performed all assays using commercially available diagnostic kits and worldwide accepted techniques. Blood cell counts were immediately performed in the sample collected in EDTA using a Cell-Dyn 3700 automated blood cell counter (Abbott Park Laboratories, Abbott Park, Illinois). Red cells were used to determine the blood group using specific antisera according to standard techniques.
A Synchron LX 20 chemistry analyzer (Beckman Coulter, Fullerton, California) was used to assay serum levels of glucose, urea, creatinine, uric acid, alkaline phosphatase, lactic dehydrogenase, serum glutamic pyruvic transaminase, serum glutamic oxaloacetic transaminase, gamma glutamyl transpeptidase, total bilirubin, indirect bilirubin, direct bilirubin, total proteins, albumin, globulins, triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and very-low-density lipoprotein cholesterol (VLDV-C). Some of these tests were performed to assure that the patients did not have liver or renal insufficiency. Atherogenic index (AI) was calculated as follows: [TC (mg/dL)/HDL-C (mg/dL)]. An AXSYM equipment (Abbott Park Laboratories) was used to evaluate serum levels of high-sensitivity C-reactive protein (hsCRP). Platelet-poor plasmas were thawed at 37°C for 5 minutes. Most tests were performed with coagulometric techniques using an STA Compaq instrument (Diagnostica Stago, Asnieres, France): prothrombin time (PT; Neoplastin Plus, Diagnostica Stago, Asnieres, France), activated partial thromboplastin time (aPTT; STA-aPTT, Diagnostica Stago), and fibrinogen (STA Fibrinogen; Diagnostica Stago).
Using a Synergy HT plate reader (Biotek Instruments, Winooski, Vermont), enzyme-linked immunosorbent assay kits were used to evaluate IgG and IgM aCL (reference values: <20 GPL/mL and <13 MPL/mL, respectively; BioRad, Hercules, California) as well as anti-β2-GP1 (reference values: <10 U/mL; Diapharma, West Chester, Ohio). In patients with prolonged aPTT, we searched and confirmed the presence of LA by means of 2 coagulometric assays based on the worldwide accepted diluted Russel viper venom test, using commercially available kits: STA-Staclot DRVV Screen 5 and STA-Staclot DRVV Screen and DDV Confirm (Diagnostica Stago).
Statistical Analysis
We used the Statistical Package for the Social Sciences (SPSS, v.16; SPSS Inc, Chicago, Illinois). For the description of demographic characteristics of the patients and the results found of the variables analyzed, we used central tendency measures and dispersion. We used a chi-square, a student t test, and a paired t test in order to analyze any possible difference between quantitative and qualitative results between the groups, respectively. A P value <.05 was considered significant.
Ethics
The study protocol was accepted by the Ethics National Committee of our institutions. In this study, we required blood drawing, a procedure routinely performed in patients with APS. Therefore, all patients were informed about the study, and signed informed consent was obtained before being included in the protocol. In order to assure the confidentiality of the information, only the investigators had access to the complete data of the participants. Blinding was broken in case of significant clinical or laboratory abnormalities. The study fulfilled the national and international regulations for clinical research: Ley de General de Salud, the Helsinki Declaration, and the Code of Nuremberg.
Results
During the study period, 501 patients were analyzed, but 115 were not included because the information in the clinical records was incomplete (n = 63), they were lost to follow-up (n = 46), or because they did not accept to participate in the study (n = 6). At the end, 386 patients were included, 308 with VTD, 67 with AT, and 11 with both VTD and AT. General characteristics of these patients are shown in Table 1. Most patients were women (n = 249). For the whole group, median age was 40.7 years (ranges: 13-88), and median age when the first thrombosis appeared was 35.0 years (ranges 12-86). Total number of thrombotic events was 677. At diagnosis of APS, most patients had only 1 thrombotic episode being mostly VTD events. In the AT/VTD group, 9 patients had already had both types of thrombosis at the moment when the APS diagnosis was done: 7 had 1 VTD and 1 AT event, 1 had 1 AT and 2 VTD episodes, and 1 more patient had 1 AT and 3 VTD events.
General Characteristics of Patients With APS and Thrombosis.
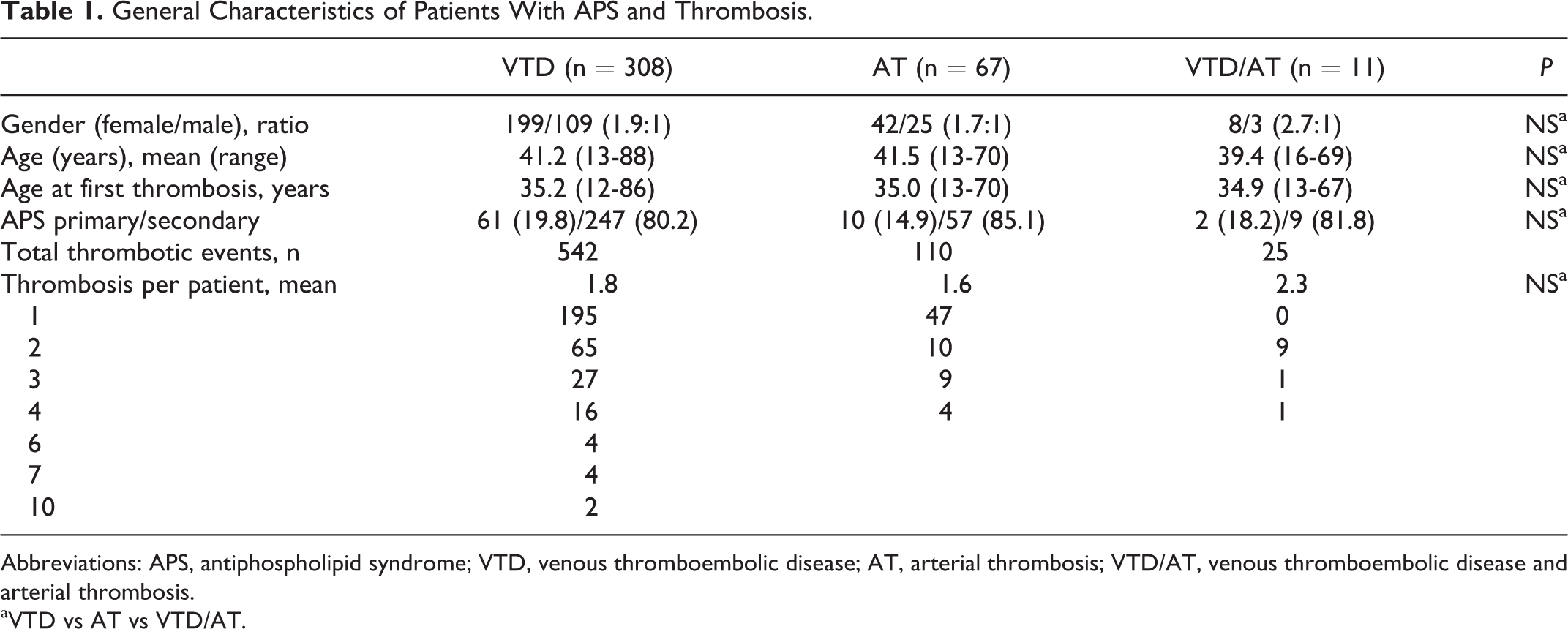
Abbreviations: APS, antiphospholipid syndrome; VTD, venous thromboembolic disease; AT, arterial thrombosis; VTD/AT, venous thromboembolic disease and arterial thrombosis.
aVTD vs AT vs VTD/AT.
During follow-up, 27 new thrombotic episodes were recorded: 21 were VTD events (16 deep vein thrombosis and 5 pulmonary embolism) and 6 corresponded to AT episodes (1 acute myocardial infarction and 5 strokes). These new thrombotic episodes occurred in 10 women (17 venous and 5 arterial events) and 5 men (4 venous and 1 arterial). One of these patients had history of an AT event, and she subsequently developed 1 VTD episode while another patient had a VTD event and had 1 new AT event.
Fourteen patients died during the study period (12 women and 2 men), and in 11 of them (10 women and 1 men), the cause of death was directly attributed to a thrombotic episode (5 venous and 6 arterial thrombotic events, respectively).
Sites of VTD and AT events are shown in Table 2. As depicted, VTD events were more frequently recorded, and some patients had both the vascular beds affected. Table 3 shows the comorbidities associated with the thrombotic episodes just at the moment when an event appeared either at diagnosis or during the follow-up. Some risk factors associated with VTD were not significantly different in patients with AT: hormonal use, obesity, pregnancy, and cancer. Type 2 diabetes mellitus and grade 3 obesity were strongly associated with VTD instead of AT. Thrombocytopenia was significantly associated with VTD; however, it should be pointed out that of 56 patients with thrombocytopenia having VTD, 35 had platelet counts >100 × 109/L, 19 had platelet counts between 100 and 50 × 109/L, and only 2 patients had platelet counts of 40 and 41 × 109/L, respectively. Three patients had thrombocytopenia in the AT group, and their platelet counts were 105, 137, and 140 × 109/L. Other comorbidities previously described as risk factors for thrombosis, namely, small-vessel thrombosis, livedo reticularis, superficial venous thrombosis, and recent or current infections, were never present in our series.
Localization of 677 Arterial and Venous Thrombotic Events in Patients With APS.a
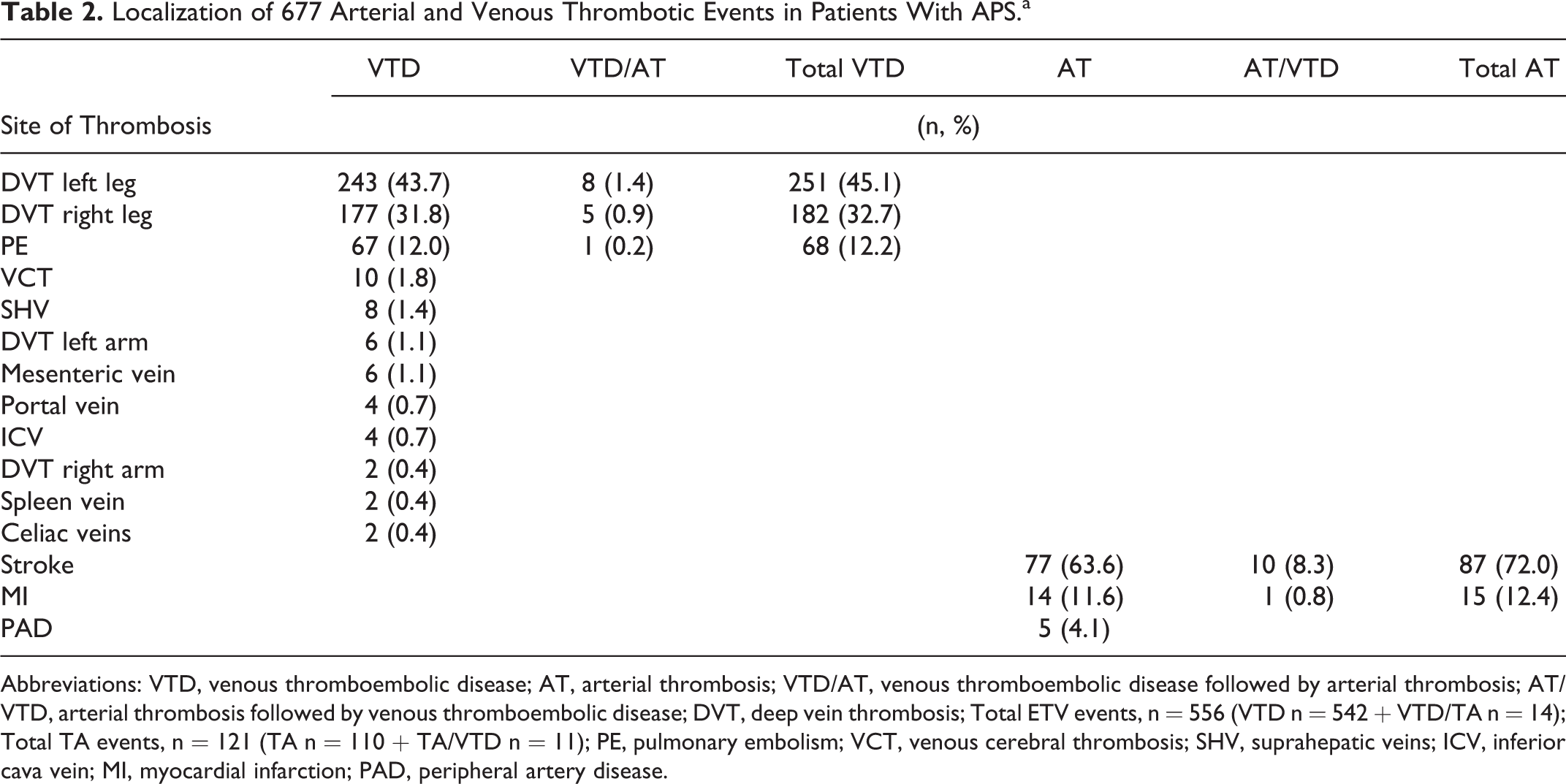
Abbreviations: VTD, venous thromboembolic disease; AT, arterial thrombosis; VTD/AT, venous thromboembolic disease followed by arterial thrombosis; AT/VTD, arterial thrombosis followed by venous thromboembolic disease; DVT, deep vein thrombosis; Total ETV events, n = 556 (VTD n = 542 + VTD/TA n = 14); Total TA events, n = 121 (TA n = 110 + TA/VTD n = 11); PE, pulmonary embolism; VCT, venous cerebral thrombosis; SHV, suprahepatic veins; ICV, inferior cava vein; MI, myocardial infarction; PAD, peripheral artery disease.
Classical Risk Factors for Thrombosis in Patients With APS.
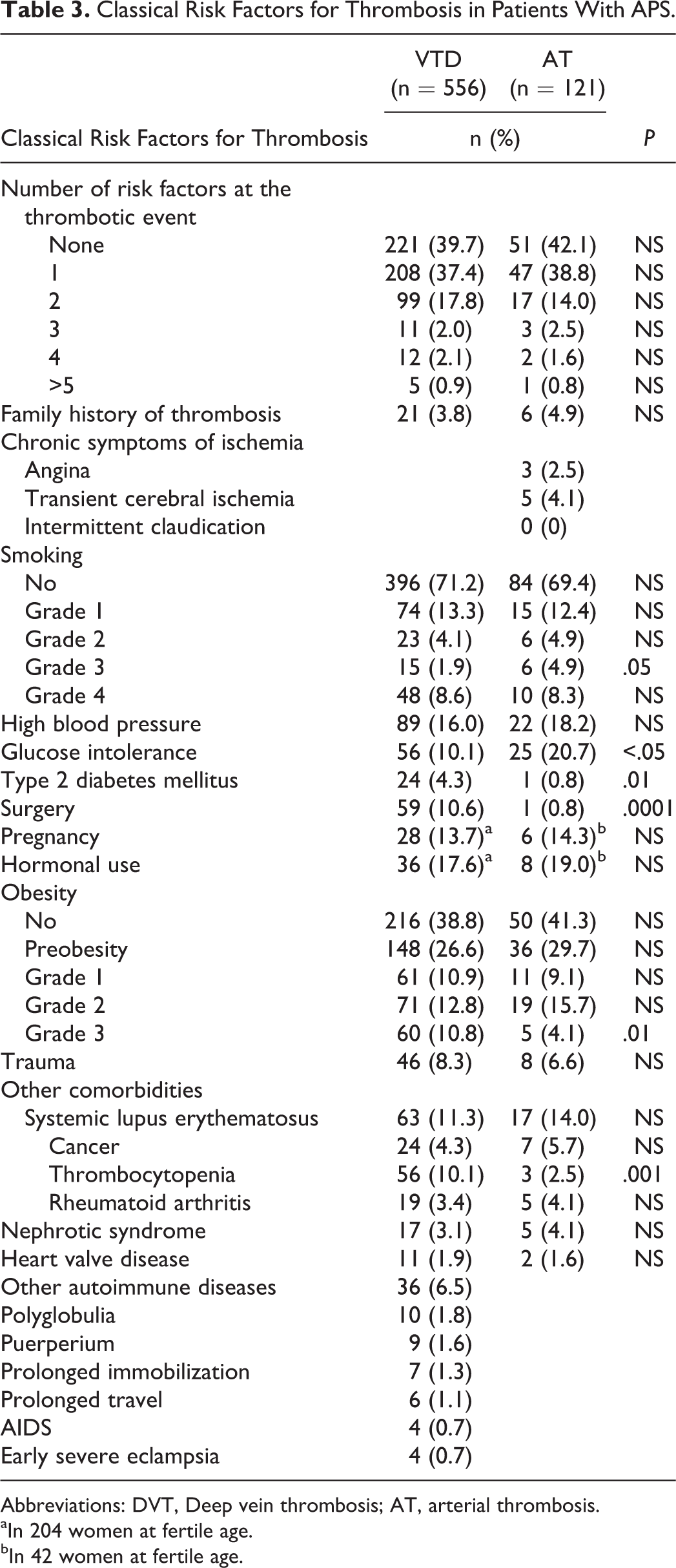
Abbreviations: DVT, Deep vein thrombosis; AT, arterial thrombosis.
aIn 204 women at fertile age.
bIn 42 women at fertile age.
Table 4 shows the results of the analysis of the laboratory tests performed immediately after a thrombotic event, when patients were included in the cohort or when a relapsing thrombotic episode occurred. Blood group distribution was not significantly different among the study groups, and 61% of the patients included in this study had O-type blood group. All liver and renal function tests were not significantly different between the groups. On the other hand, we did not find significant differences between the study groups for variables classically associated with AT: serum levels of TC, TG, HDL-C, and AI. Moreover, no significant differences between the groups were found in terms of the other laboratory variables analyzed (Table 4). The only exception was for the presence of LA, which was significantly higher in the group with VTD (Table 5).
Laboratory Data in Patients With APS and Venous or Arterial Thrombosis.
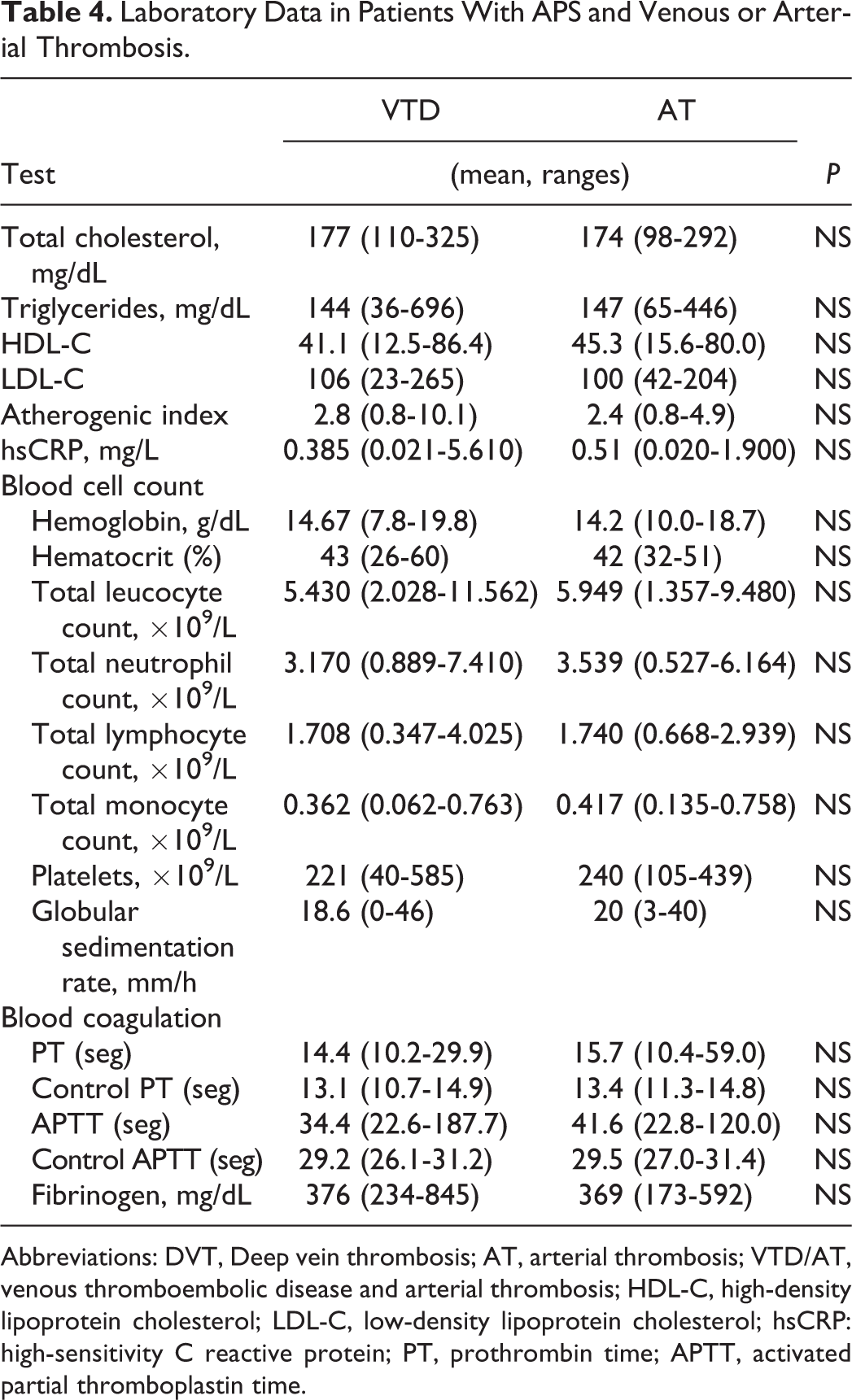
Abbreviations: DVT, Deep vein thrombosis; AT, arterial thrombosis; VTD/AT, venous thromboembolic disease and arterial thrombosis; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; hsCRP: high-sensitivity C reactive protein; PT, prothrombin time; APTT, activated partial thromboplastin time.
Tests for APS Diagnosis.
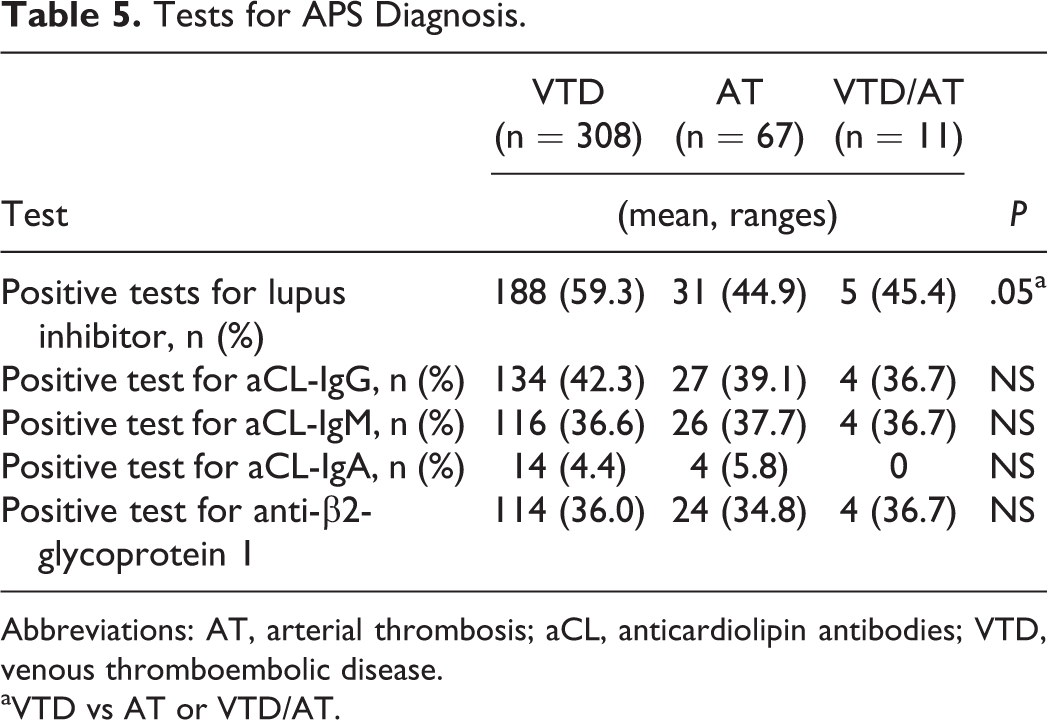
Abbreviations: AT, arterial thrombosis; aCL, anticardiolipin antibodies; VTD, venous thromboembolic disease.
aVTD vs AT or VTD/AT.
Discussion
The APS, an acquired thrombophilic condition, is currently defined by the occurrence of 1 or multiple thrombosis either venous or arterial, and recurrent pregnancy-related complications (including fetal loss) in association with the persistent positivity of aPL (at least 12 weeks apart), namely, LA, aCL, or anti-b2GPI antibodies. 12 Undoubtedly, the hallmark of this syndrome is the presence of a thrombotic event, either venous or arterial. However, even the pregnancy-related complications also show a clear thrombotic pathophysiology. Antiphospholipid syndrome is mostly diagnosed after an AT or VTD episode, and it should always be included in the thrombophilic screening.
The pathophysiological events leading to thrombosis in APS are still unknown, although some data suggest that aPL may induce thrombosis through several mechanisms. 13 –15 Thrombosis is a multigenic phenomenon in which a single risk factor is not enough to induce thrombotic events. 16,17 In non-APS patients with thrombosis, most of them have a clear association between specific risk factors and the thrombotic event. Some of these risk factors are associated with both types of thrombosis, and they may have additive effects in some patients. However, in APS, AT and/or VTD events are frequently, fully, and simply attributed to the APS itself.
Because APS is a disease recently described relatively, many issues are still unresolved. 18 For example, little is known about classic risk factors for VTD or AT described for the general population and their likely impact on thrombosis. This would allow to assessing best the concomitance of thrombotic risk factors for an accurate evaluation of aPL-associated events. Appropriate stratification of classic atherothrombotic risk factors is crucial in older patients who are more prone to AT events. Until now, environmental or genetic thrombotic risk factors in APS have been scarcely reported impeding a wider judgment about a causal relationship between aPL and clinical outcomes. 12 Therefore, our aim was to determine whether in the APS population, the association of the risk factors for VTD or AT is similar as in the general population.
Some of our data agree with previous published evidence. For example, in localization of thrombotic events, VTD was more frequently observed than AT, most patients were young women, and a high number had more than 1 thrombosis. 19,20 However, we found some uncommon facts, for example, 34 cases with VTD had an uncommon localization of the thrombosis: mesenteric, inferior cava vein, suprahepatic, mesenteric, portal, spleen, and celiac (n = 26). These types of thrombotic events have been associated with a worse prognosis and a more aggressive evolution. 21,22 Moreover, 8 had thrombosis of the veins of the arms. Finally, some patients have both vascular territories affected, an infrequent fact observed in the non-APS population.
On the other hand, classical epidemiological associations and clinical characteristics widely described in the general population in association with either VTD or AT were not always present in our patients. Surprisingly, some risk factors widely associated with VTD were not significantly different when compared to patients with AT: hormonal use, pregnancy, trauma, and cancer. Unexpectedly, some facts deserve attention. First, family history of AT and high blood pressure was not significantly different between patients with AT and VTD. This unexpected lack of association between APS and high blood pressure disagrees with previous data showing a significant relationship. 23,24 Second, except for grade 3 smoking, no significant association between AT events, and this risk factor was found. Third, frequency of clinical symptoms of chronic ischemia was very low in patients with AT (Table 3). Fourth, type 2 diabetes mellitus and grade 3 obesity were associated with VTD instead of AT, a fact that contrasts with previous evidence in patients with APS. 25 These associations found in our patients suggest that patients with APS are differently affected by the classical thrombotic risk factors versus the general population. However, the presence of risk factors affecting a general population, as occurs for example with diabetes mellitus and obesity in our country, also affect the APS population. Finally, near 40.9% of the patients have no classical risk factor associated with the thrombotic event.
In the particular case of patients with APS having AT, lack of chronic clinical data associated with the presence of ischemia in the cerebral, cardiac, or peripheral territories suggests that these thrombotic events have a sudden clinical presentation, and it is reasonable to assume that they cannot be considered as atherothrombotic events, at least in the vast majority of the cases. These data may also explain the lack of association between AT and classical atherogenic risk factors and strongly suggests that the presence of the aPL antibodies exerts by themselves enough damage on the endothelium-dependent blood coagulation system to induce an AT.
In terms of the laboratory data, three major findings need to be addressed. First, it becomes clear that the presence of LA confers a significant risk for VTD, while aCLs have no such thrombogenic potential. 26,27 Second, it has been widely described that non-O blood groups are closely related to VTD. 28,29 In our country, >85% of the general population is O-type but only 61% of our patients. In other words, non-O blood groups were more frequent in our patients versus the general population: 39% versus 15%, respectively. This finding suggests that the non-O blood groups may have a negative influence on the thrombotic risk and that the APS population does not escape to this negative prothrombotic effect. Third, thrombocytopenia, a finding in APS that represents a considerable challenge for patients requiring anticoagulation, is also considered a risk factor for thrombosis in some series. 30 In this study, despite the fact that thrombocytopenia was significantly associated with VTD in the majority of patients, it was almost always minor or mild.
Patients with APS are at high risk of recurrent thrombosis 26,27 ; however, during follow-up, we had a relatively low incidence of new thrombotic episodes, most of them being VTD events affecting women. A relatively low mortality rate was noticed, and most of the deaths were associated with thrombosis. These low incidences are likely due to the fact that patients were attended in an anticoagulation clinic. It is known that better results in terms of stability and effectiveness of the anticoagulant treatment are obtained when patients are controlled in such clinics.
There are 2 major limitations in our study. First, we did not evaluate inherited thrombophilic risk factors, a fact that may be an important bias of our study. However, it has been described that (1) inherited protein C, protein S, and antithrombin deficiencies are rarely found in patients with APS; (2) the prevalence of the prothrombin G20210A mutation is not significantly associated with thrombosis in patients with APS and; (3) the presence of factor V Leiden mutation may define only a small subgroup of patients who had high risk of both venous and arterial thrombosis. These findings suggest that thrombotic complications in APS are largely related to aPL-mediated mechanisms. 31,32 Second, we did not have data about endothelial cell dysfunction.
In conclusion, our findings strongly suggest that the thrombotic episodes in APS are largely due to the APS itself and that classical risks factors for arterial or venous thrombosis, although present in these patients, do not have a main role. Because some of our data contrast with previous data, we feel that these differences are related to the characteristics of our population as occurs in other thrombophilic states or clinical conditions. Therefore, it may be difficult to elaborate predictive clinical scores for thrombotic episodes that could be applicable to patients with different ethnical background. Of course, more scientific data to explain these differences and their likely impact on the thrombotic events in different populations are mandatory.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Instituto Mexicano del Seguro Social [R-2014-3609-26]. Daniel Navarro-Carpentieri received a grant during the period between June 2014 and December 2016 from the Consejo Nacional de Ciencia y Tecnologia (CONACYT, Mexico) and from the Instituto Politecnico Nacional (Mexico).