
Abstract
We aimed to investigate prognostic factors of in-stent restenosis (ISR) within 3 years in older acute coronary syndrome (ACS) patients after drug-eluting stent (DES) implantation and establish a clinical model for predicting ISR. We retrospectively collected 215 older ACS patients who followed coronary angiography (CAG) after DES implantation, divided into ISR group and non in-stent restenosis (non-ISR) group according to the results of reviewed CAG. Logistic regression analysis was performed to screen independent predictors related to ISR and build the clinical predictive model, which clinical application was assessed by decision curve analysis (DCA) and clinical impact curve (CIC). Kaplan-Meier survival curves for ISR by independent predictors. In multivariate logistic regression analysis showed that the red cell distribution width (RDW) was higher in ISR group compared with non-ISR (odds ratio (OR) = 1.54, 95% confidence interval (CI): 1.14–2.08, p < 0.01). Instead, a negative correlation was observed between minimum stent diameter and ISR (OR = 0.28, 95%CI:0.09-0.86, p = 0.03). A novel nomogram composed of these significant features presented a concordance index (C-index) of 0.710, DCA and CIC suggested that the predictive nomogram had clinical utility. Schoenfeld residuals showed the model RDW ≥ 12.6% with minimum stent diameter <3 mm was consistent with the proportional risk assumption. The Kaplan-Meier estimate for ISR showed statistical significance. Higher levels of RDW and lower minimum stent diameter were associated with incidence of ISR within 3 years in older ACS patients after DES implantation.
Introduction
Currently, DES implantation is one of the major treatment methods for patients with ACS, but ISR after DES implantation is still noteworthy. 1 ISR is most commonly defined as luminal renarrowing of greater than 50% (binary angiographic restenosis), either within the stent or within the stent and including 5 mm proximal or distal to the stent margin on follow-up angiography. 2 With the development of interventional technology, the success rate of interventional therapy has been improved, 3 but the problem of ISR has not been completely solved. Therefore, the identification of risk factors associated with ISR is urgently needed to provide evidence for the prevention of ISR.
Although the mechanism of ISR has not been fully elucidated, the inflammatory response is thought to play a key role in the development of ISR. 4 The pathophysiology of ISR is characterized by neointimal hyperplasia and the mechanical vascular damage caused by percutaneous coronary intervention (PCI) responds to the matrix deposition of massive inflammatory responses that stimulate vascular smooth muscle cell proliferation and extracellular proliferation, leading to neointimal thickening and restenosis.4,5
Several studies have explored the risk factors of ISR risk or revascularization after PCI in coronary heart disease (CHD) patients, suggested that dyslipidemia, diabetes, hypersensitivity C reactive proteins (CRP), RDW, smoking, vessel size and complex lesion morphology were strongly associated with ISR.6–9,10 Some studies show that increasing age was one of the factors involved in the occurrence of ISR. 11 The risk factors affecting the occurrence of ISR may be different from the general population in older patients. Currently, little is known about the risk factors for ISR in older patients after DES implantation. Therefore, the identification of the risk factors associated with ISR provides a very urgent basis for preventing ISR. We sought to evaluate the characteristics and risk factors of ISR in older patients with PCI to provide insights into the prevention and treatment of ISR.
Materials and Methods
Study Population and Design
This study was a retrospective study, we enrolled 215 older ACS patients (aged 65 years and above) from two centers, whom follow-up reviewed CAG within 3 years after DES implantation from September 1, 2016, to December 1, 2018. The older ACS patients were divided into the two groups based on the results of follow-up angiography: ISR group (n = 30) and no-ISR group (n = 185). The types of stents used in all procedures included the Rapamycin series.
Exclusion criteria: severe heart failure, cardiomyopathy, prior coronary artery bypass surgery (CABG), severe liver and kidney dysfunction, various infectious diseases, malignant tumors, autoimmune diseases or immunosuppressive treatment, severe anemia, surgery and severe trauma within 3 months before PCI.
Clinical and Laboratory Assessments
Demographic characteristics (age and gender) and vascular risk factors (current smoker, hypertension, hyperlipidemia, and diabetes) were collected. Collected the medical history, physical examination, blood biochemistry tests of all patients, including: routine blood tests, liver function tests, renal function tests, blood lipid tests.
Angiographic Assessment and Follow up
At 1, 3, 6, 12, 24 and 36 months after PCI, there was follow up with all patients by telephone, outpatient service and hospitalization. Review CAG was performed within 3 years after PCI (Figure 1). Two experienced cardiologists in our hospital performed CAG and evaluated the angiography results. Coronary artery quantitative analysis was used to intuitively quantify the coronary artery stenosis. All patients were divided into ISR group and non ISR group according to results of Quantitative coronary angiography (QCA) from follow-up CAG. ISR was defined as restenosis ≥50% inside the stent or 5 mm proximally or distally in the target vessel. The parameters in the patient operation include: stent type, number, length, diameter from the cardiac interventional database.

Study Flowchart
Statistical Analysis
Statistical analysis was performed using the SPSS package, version 23.0 (Chicago, Illinois, USA) and R software (v.4.1.2; https://www.r-project.org). Quantitative variables were expressed as mean value ± SD for continuous variables and percentages for categorical variables. Normally-distributed continuous variables were compared using the independent-samples t-test. Categorical variables were compared by the Chi-squares test. Multivariable stepwise logistic regression was used to compare factors significantly associated with ISR in univariable testing (variables with a p-value of <0.1). OR with 95% CI were presented as results. Receiver operating characteristic (ROC) curves and areas under the curves (AUC) determined the predictive values of significant predictors. A nomogram based on independent diagnostic predictors from the univariate and the multivariate logistic regression model was established. The performance of the nomogram was assessed by C-index, and internal validation with 1000 repetitions bootstrap resampling was used to test discriminative value. The calibration was confirmed by the Hosmer-Lemeshow test, DCA and CIC were conducted to evaluate the clinical utility of the nomogram. Schoenfeld Residuals Test was used to investigate the independence of residuals from time to testing the proportional hazards assumption in the Cox model and the survival probability was estimated from Kaplan-Meier curves and compared using the log-rank test. A 2-tailed P < 0.05 was considered statistically significant.
Results
Our study enrolled a total of 215 older ACS patients, of these 30 patients occurred ISR according to the results of followed angiography, the incidence of ISR was 14.0% (Figure 1).
Baseline characteristics were shown in Table 1. There were statistically significant differences in RDW and minimum stent diameter between ISR and non-ISR groups (P = 0.02, 0.004, respectively)
Baseline Characteristics

Data are presented as N (%), mean ± (SD) and median interquartile range in parentheses.
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; apoA1, ApolipoproteinA1; apoB, ApolipoproteinB; ARB, angiotensin receptor blocker; HbA1c, Hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; ISR, in-stent restenosis; LDL-C, low-density lipoprotein cholesterol; NHDL-C, non-high-density lipoprotein cholesterol; non-ISR, non in-stent restenosis; PDW, platelet distribution width; RDW, red cell distribution width; TC, total cholesterol; TG, triglyceride; WBC, white blood cell
DAPT*: Dual Anti-Platelet Therapy in the first year after PCI
Multivariate logistic regression analysis was used to compare the variables with univariate analysis P < 0.1. RDW and minimal stent stents were significantly associated with the incidence of ISR (OR = 1.54, 95% CI: 1.14-2.08, p < 0.01; OR = 0.28, 95%CI:0.09-0.86, p = 0.03,respectively) in Table 2.
Univariate and Multivariate logistic regression analysis for predictors of ISR for older patients in pre-PCI

Abbreviations: CI, confidence interval; OR, odds ratio; RDW, red cell distribution width;
DAPT*: Dual Anti-Platelet Therapy in the first year after PCI
ROC Analysis and Nomogram
ROC predicted to ISR were exhibited in Figure 3A. The complex model (diameter of minimum stent and RDW) was represented AUC of 0.710. According to the results of the multivariable logistic regression, predictors diameter of minimum stent and RDW were identified to establish the predictive nomogram. A higher total sum of the designated points in the nomogram refers to a higher risk of ISR in older ACS patients after DES implantation (Figure 2A). The C-index of 0.710 (95% CI: 0.609-0.811) was calculated as the discriminative value of this nomogram, suggesting a good predictive power, bias corrected c index 0.704. In addition, the non-significant Hosmer-Lemeshow test result (P = 0.77) on the calibration curves indicated that the predicted outcomes matched well to the real ISR observed(Figure 2B).
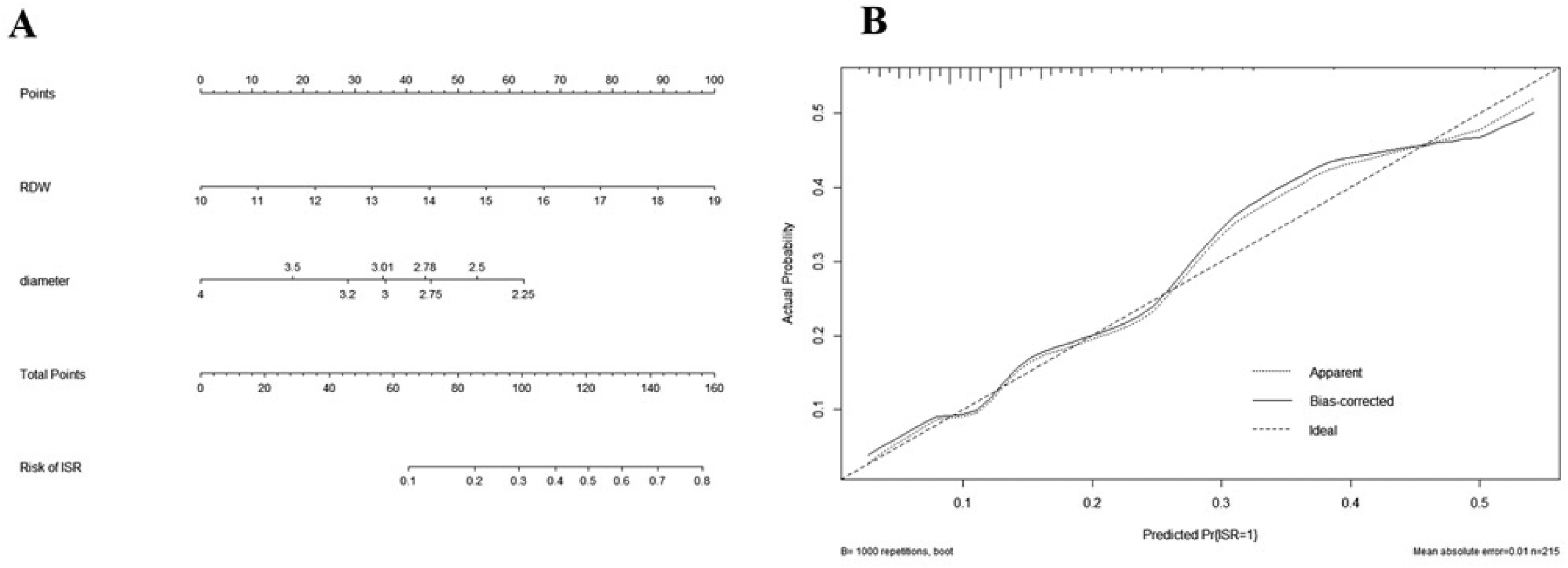
Nomogram to pridict ISR in older ACS patients after DES implantation and calibration curve

A: ROC curves; B: Decision curve analysis; C: Clinical impact curves
Validation of Clinical Application of the Nomogram
decision curve analysis (DCA) was performed to investigate the net benefit of this predictive models (Figure 3B). The results suggested that the nomogram (complex model) could provide greater net benefit than other models when the threshold probability ranged from 30% to 60%. The clinical impact curve (CIC) for the ISR in older ACS patients was illustrated in Figure 3C. This curve reveal the estimated numbers of participants deemed to be at a high risk of ISR, and the true positive value was in the range of 0.0 to 1.0. For example, at a 30% risk threshold, out of 1000 patients screened, approximately 400 would be deemed high risk through model analysis and >400 would be deemed high risk using the other models analysis.
COX Model and Kaplan-Meier Curve
In the Figure 4, each co-variate was not statistically significant (p > 0.05), and the global test is not statistically significant. Therefore, we could assume that this Cox model fits the proportional hazards assumption by Schoenfeld Residuals Test and calculated cutoff values of RDW (12.6%) and minimum stent diameter (3 mm), which corresponding to the co-variates when HR is equal to 1. The cohort was divided into three groups: the higher RDW group (RDW >12.6%,) the lower a minimum stent diameter group (minimum stent diameter < 13mm), and higher RDW combined lower minimum stent diameter group.
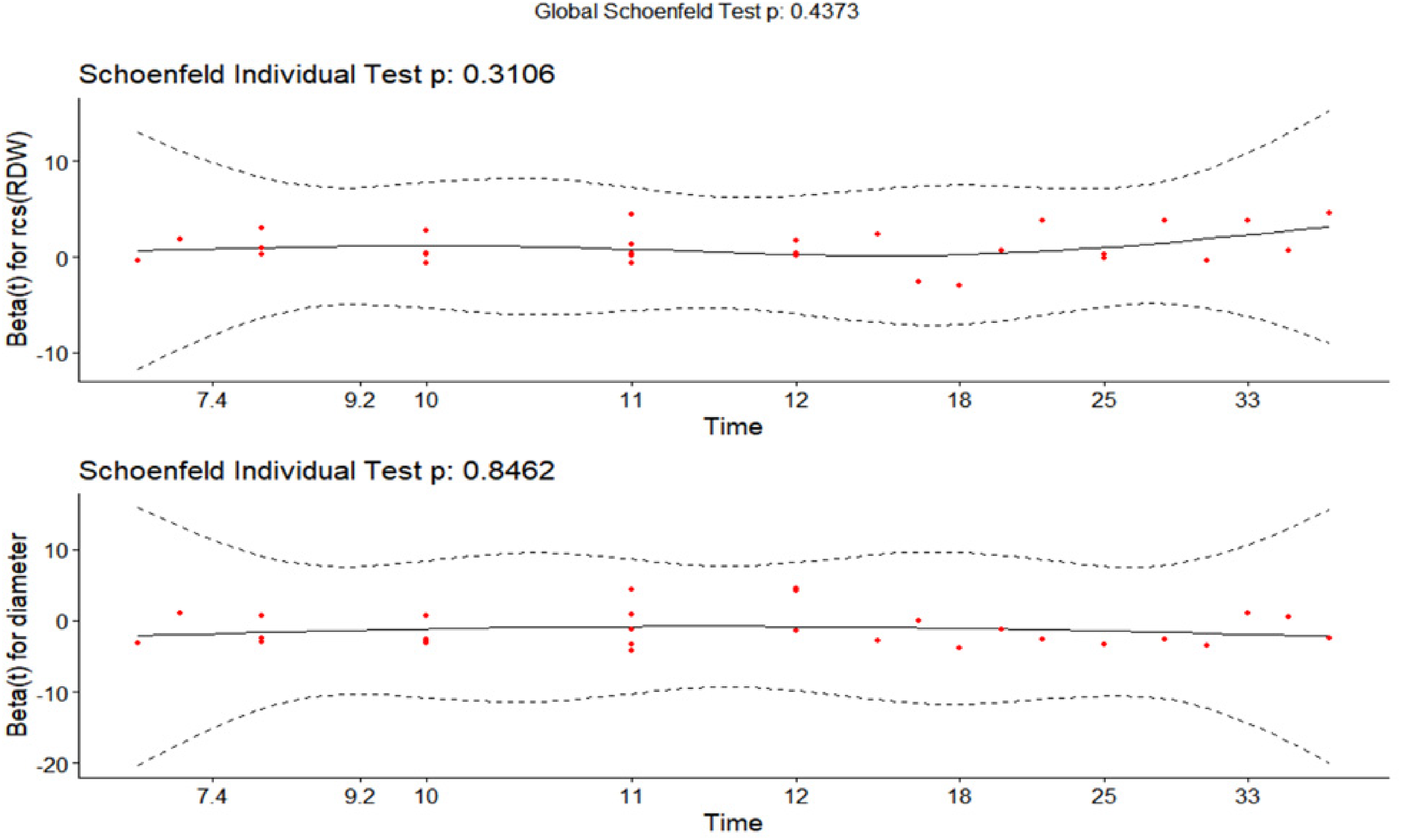
Schoenfeld Residuals Test
Of 215 patients, 30 suffered from ISR during 3 years follow-up. The Kaplan-Meier estimate for ISR showed statistical significance in the higher RDW combined lower minimum stent diameter group (p = 0.004; HR = 3.33; 95%CI:1.48-7.04) [ Figure 5]

Kaplan-Meier curves for survival probability
Discussion
This was the first study to systematically assess the impact of RDW combined minimum stent diameter on risk of ISR events in older ACS patients after DES implantation. Overall, the RDW was significantly higher and minimum stent diameter was significantly lower in older patients with ISR compared to non-ISR group.
Despite the widespread use of the new generation of DES and new oral antiplatelet aggregation drugs, ISR remains concern after PCI, which increased risk of adverse clinical outcomes including recurrent angina or even myocardial infarction in the real world. 12 After stent implantation, mechanical-induced vascular injury caused local and systemic inflammatory processes, subsequently leading to migration and proliferation of smooth muscle cells, particularly in patients with systemic inflammatory reactions, ultimately leading to ISR. 13 Based on the key role of inflammation in this process, some biomarkers associated with inflammatory responses have been shown to effectively predict the incidence of ISR.14–17
However, there was no significant correlation between biomarkers of lipid and ISR in older patients, we consider that as the older patients, was a special group, because a larger number of older patients were complicated with CHD, hypertension, diabetes, dyslipidemia, and these older patients may have long term take drugs including antiplatelet aggregation drugs, statin, angiotensin-converting enzyme inhibitors/angiotensin receptor blocker (ACEi/ARB) preprocedure, therefore, the significance of lipid biomarkers before PCI decreased significantly compared with that of ordinary patients. The RDW and minimum stent diameter were found to be statistically significant for predict ISR in our study. We know that RDW is an indicator to measure of the heterogeneity of the erythrocytes. Both the destruction of red blood cells and the reduced production rate can increase the value of RDW. The increase in value of RDW was recently found in some researchers as an independent predictor of the incidence of ISR after PCI in patients and the mortality in patients with heart failure.18–23 In a series of clinical studies, a significant positive correlation between RDW and various inflammatory markers, inflammation can promote increased RDW by impairing iron metabolism, by inhibiting erythropoietin production or response, or by shortening the survival time of red blood cells. 24 In our study, higher preprocedural RDW in ISR patients than those without ISR (Table 1) suggested that ISR patients may be at a higher level of inflammation with a greater inflammatory response to PCI.
A previous study have shown that the incidence of ISR in DES was significantly lower than in bare-metal stent (BMS), only in vessels <3.0 mm. 25 But, another study showed a greater diameter of left circumflex artery (LCX) increase the incidence of left anterior descending coronary artery (LAD) stent restenosis. 26 To date, there have been no numerous studies demonstrating the relationship between stent diameter and ISR in older patients with ACS. From our results, we concluded that the minimum stent diameter was negatively associated with the occurrence of ISR after PCI in older ACS patients, however, there were many other factors affecting ISR, which also have different influence values in different groups, because the pathogenesis of ISR is multifactorial. 27
As a prediction tool, nomogram has advantages over the conventional analysis using ORs. 28 In the current study, we incorporated the independent risk factors RDW and minimum stent diameter to develop a nomogram for predicting ISR in older patients with ACS after DES implantation. This model nomogram presented more accurate predictive efficacy, as the DCA and CIC illustrated well adoption of the nomogram into clinical use in terms of threshold probability. 29 The nomogram-assisted medical decision-making may meet the needs of aging ACS patients after DES implantation for risk stratification and conducting risk-oriented therapy to improve outcomes during and after discharge.
Our study focused on older patients with ACS undergone DES implantation, and results showed that the model consisted of higher plasma RDW and lower minimum stent diameter have good predictive value for ISR within 3 years in older ACS patients after DES implantation in Kaplan-Meier curves, but there was no statistical significance when RDW and minimum stent diameter predict 3 years prognosis as factors alone.
The strengths of our study were that, RDW and diameter of minimum stent are objective clinical parameters that can be easily measured or collected, and this model nomogram showed improved prediction accuracy.
But, there were some limitations in our study: our study was retrospective research with not enough larger samples, and was lack of the external validation to further test the applicability of the nomogram, although the internal validation showed the good discriminative value of nomogram; and all patients underwent coronary artery angiography without intravascular imaging or functional intervention techniques, may affected accuracy of results.
Conclusion
Higher levels of RDW and lower minimum stent diameter were associated with incidence of ISR within 3 years in older ACS patients after DES implantation. The model of present nomogram involving RDW and minimum stent diameter was sufficient to provide an individualized prediction of ISR was a promising prognostic value to optimize the strategies for risk stratification, treatment, and prevention of ISR in older ACS patients who have undergone DES implantation.
Footnotes
Author Contributions
DC: Conceptualization, Investigation, Formal analysis, Methodology, Supervision, Writing-original draft, Writing-review & editing; JZ: Conceptualization, Investigation, Writing-review & editing; YD: Conceptualization, Investigation, Methodology, Supervision, Writing-review & editing; AW: Investigation, Methodology, Writing-review & editing; TY: Formal analysis, Methodology, Writing-review & editing; SL: Formal analysis, Methodology, Writing-review & editing; All authors have read and agreed to the published version of the manuscript.
Data Availability
Restrictions apply to the availability of some or all data generated or analyzed during this study to preserve patient confidentiality or because they were used under license. The corresponding author (CDY) will request details of the restrictions and any conditions under which access to some data may be provided.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was carried out in accordance with the Declaration of Helsinki and the use of its data have been approved by the Taicang first peoples Hospital Ethics Committee (IRB: TCYY-KY-2021-153). The study is retrospective in design, the need for informed consent was waived.
Funding
This work was supported by a project grant from Science and Technology Program of Taicang City, China (No.TC2018JCYL25).