
Abstract
Background
Percutaneous coronary intervention (PCI) is the main treatment option for acute coronary syndromes (ACS) often related to the progression and rupture of vulnerable plaques. While drug-eluting stents (DES) are now routinely used in PCI, drug-coated balloons (DCB) are a new strategy to PCI and their practice in the treatment of ACS with vulnerable plaques has not been reported. This study aimed to evaluate the safety and efficacy of DCB in ACS complicated with vulnerable plaque lesions.
Methods
123 patients were retrospectively analyzed and diagnosed with ACS and given PCI in our Cardiology Department from December 2020 to July 2022. Vulnerable plaques were confirmed by intravenous ultrasound (IVUS) in all patients. According to individual treatment plan, patients were entered into either DCB (n = 55) or DES (n = 68) groups. The results of coronary angiography and IVUS before and immediately after percutaneous coronary intervention were analyzed. The occurrence of major adverse cardiovascular events (MACE) and the results of coronary angiography were also evaluated during follow-up.
Results
There were no significant differences in baseline clinical characteristics, preoperative minimal luminal diameter (MLD), and preoperative diameter stenosis (DS) between the two groups. Also, there were no differences in IVUS plaque burden (PB), vessel area, and lumen area in the two groups before and immediately after PCI. The efficacy analysis showed that immediately after PCI, the DCB group had smaller MLD and higher degrees of lumen stenosis than the DES group (P < 0.05). However, during follow-up, no significant differences in MLD and DS were seen in two groups; relatively, late loss in luminal diameter(LLL)in the DCB group was smaller (P<0.05). Safety analysis showed that during follow-up, 9 patients developed restenosis after DCB implantation while restenosis occurred in 10 patients with DES treatment, no statistical difference in the incidence of restenosis in the two groups. Besides, there was no statistical difference in the incidence of major adverse cardiac events(MACE)during hospitalization and follow-up in the DCB group (7.3% (4/55)) and the DES group (8.8% (6/68)).
Conclusion
DCB is safe and effective for ACS complicated with vulnerable plaque and has an advantage over DES in LLL.
Introduction
Acute coronary syndromes (ACS) is a serious coronary heart disease that threatens human health. Coronary plaques in such patients usually have a large plaque burden with lipid-rich necrotic cores, called vulnerable plaques, whose progression and rupture lead to unstable angina, acute non-ST elevation myocardial infarction, and acute ST-elevation myocardial infarction.1–4 Percutaneous coronary intervention is now an effective treatment approach for ACS. PCI can restore normal blood flow through myocardial revascularization and thus greatly improves symptoms and prognosis in ACS patients.5,6
Compared with traditional two-dimensional coronary angiography (CAG), new intraluminal imaging techniques such as IVUS have more efficacy in reducing complications after drug-eluting stents placement, decreasing in-stent restenosis rate, and improving treatment outcome. Equally important, IVUS can better provide intravascular imaging data for coronary vascular lesions with coronary overlapping, anatomical abnormalities, aneurysms, myocardial bridges, and calcifications, especially in the identification of coronary culprit vessels. Because most ACS patients present with plaque ruptures, an accurate identification of the nature, extent and location of plaque ruptures is particularly important for the formulation of diagnosis and treatment planning. In this context, IVUS is superior to CAG in providing relevant imaging information and intraprocedural guidance of PCI and evaluating postoperative results and clinical prognosis.7,8
Currently, DES is the preferred strategy for PCI in patients with ACS. The use of DES has the advantages of inducing intimal hyperplasia, thickening fibrous cap, and normalizing wall stress to reduce plaque rupture. However, subsequent complications of DES may occur, such as in-stent restenosis, in-stent hyperplasia, and stent fracture, and require long-term dual antiplatelet therapy. In severe cases, there may be no reflow phenomenon after stent placement, rapidly resulting in a larger area of myocardium infarction.9–11 DCB are a new revascularization technique that has become the treatment of choice for in-stent restenosis because it meets the new concept of intervention without implantation. Indications of DCB also include small vessel disease and bifurcation disease, among others.12–14 However, there are few reports related to the use of DCB in ACS patients with vulnerable plaques. Therefore, this study used DES as a parallel treatment to examine the safety and efficacy of DCB in ACS complicated with vulnerable plaques lesions under the guidance of IVUS.
Materials and Methods
Patients
This retrospectively study investigated 123 patients who were diagnosed with ACS and underwent PCI in the Department of Cardiology, the First Affiliated Hospital of Zhengzhou University from December 2020 to July 2022, and all patients were confirmed to have vulnerable plaques by IVUS. According to the treatment strategy they received, patients were entered into either the DCB treatment group (n = 55) or the DES treatment group (n = 61). Figure 1 shows the study flowchart.
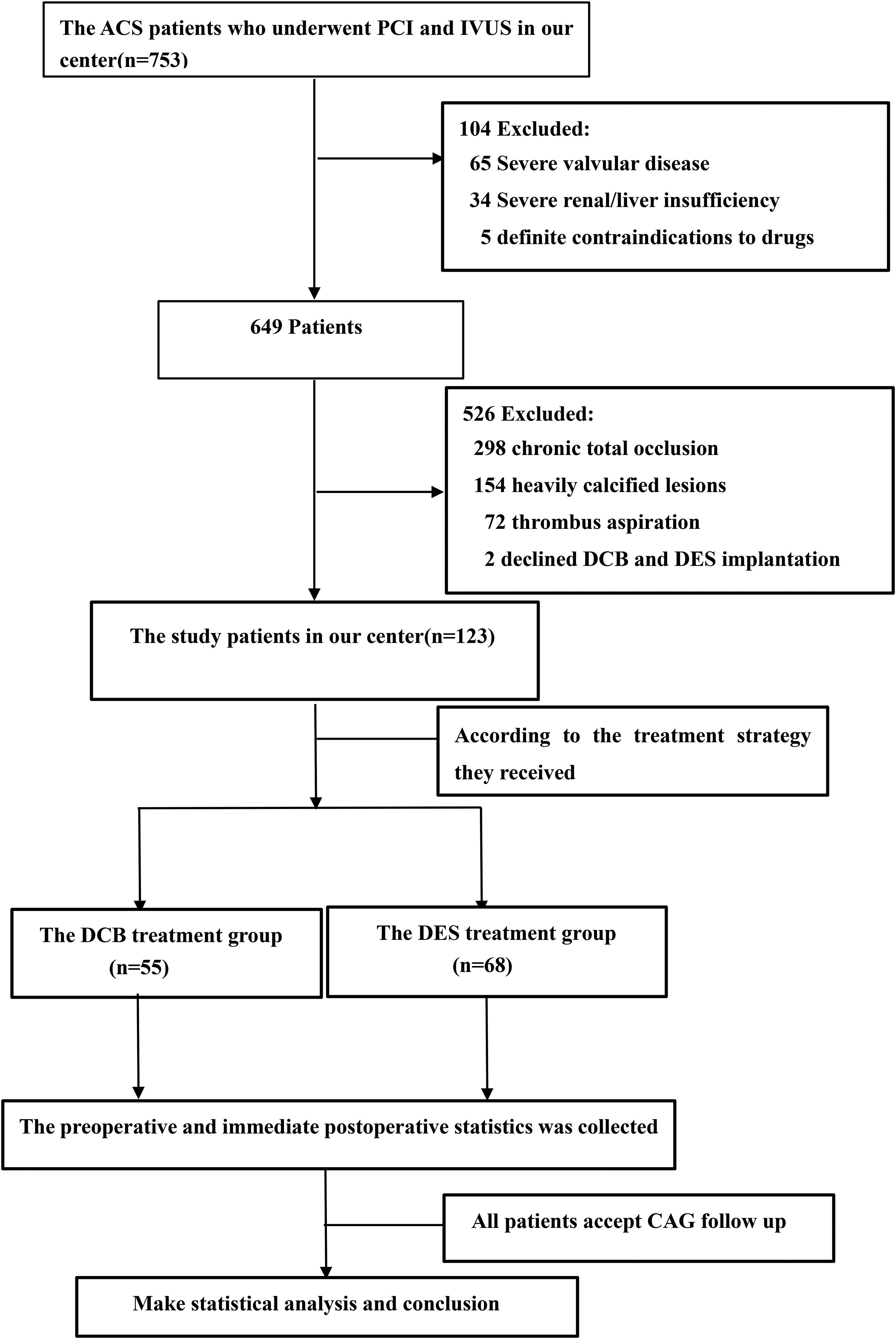
The flowchart of this study.
Inclusion criteria: (1) 18-85 years of age; (2) meeting the diagnostic criteria of the European Heart Association for ACS 15,16(3) having definite culprit vessel; and (4) gray-scale IVUS showing PB ≥ 70% and minimal luminal area (MLA) ≤ 4.0 mm2. 17 Exclusion criteria: (1) chronic total occlusion; (2) heavily calcified lesions requiring rotational atherectomy; (3) patients with thrombus aspiration; (4) severe valvular insufficiency or valvular stenosis; (5) definite contraindications to antiplatelet drugs or anticoagulants; (6) dissection repair remedial stents after DCB implantation; (7) severe renal insufficiency (GFR< 30 ml/min) or severe liver insufficiency; and (8) patients who declined DCB and DES implantation.

The survival curve of DCB and DES groups
PCI Procedure
Patients received dual antiplatelet therapy.18–22 Scheme 1: preoperative loading dose of aspirin 300 mg + ticagrelor 180 mg, postoperative maintenance dose of aspirin 100 mg + ticagrelor 90 mg, twice a day. Scheme 2: preoperative loading dose of aspirin 300 mg + clopidogrel 300 mg, postoperative maintenance dose of aspirin 100 mg/d + clopidogrel 75 mg/d. For special ACS patients, such as emergency PCI patients, comatose patients, and patients with poor cooperation, preoperative dual antiplatelet drug therapy might not be given and replaced by continuous intravenous anticoagulant drugs.
After routine sterilization and draping, the radial artery or femoral artery was selected for arterial puncture and sheath insertion. CAG was performed according to established protocols. To clearly display the culprit vessels, an appropriate positioning was selected for imaging according to the preoperative electrocardiogram, and multi-position imaging was performed if necessary. Culprit vessel were determined by combining the patient's electrocardiogram, echocardiography, and intraoperative angiography, and graded according to the Thrombolysis in Myocardial Infarction (TIMI) criteria. For TIMI grade < 3 culprit vessels, a compliant balloon was used to pre-dilate the culprit vessel lesions to restore TIMI grade 3 flow. According to the patient's condition, IVUS was performed at the appropriate time. The probe was sent to the relatively normal segment at the distal end of the culprit vessel, and then withdrew to the relatively normal segment at the proximal end at a constant rate of 0.5 mm/s to obtain intravascular imaging including vessel area, lumen area and plaque burden.
Before DCB or DES implant in the culprit vessel, an appropriate compliant balloon, semi-compliant balloon, cutting balloon, or spinous balloon was used to dilate the lesion and reduce culprit stenosis. 23 For DCB implantation, if the degree of vascular stenosis was ≤ 30%, and there was no dissection or only type A or B dissection after dilation, a size-matched DCB was chosen based on IVUS imaging and placed in the lesion sustained release before balloon withdrawal. The length of the DCB catheter exceed the target lesion by at least 5 mm. and the ratio of DCB diameters with reference vessel diameters were 0.8–1.0. The recommended inflation time was at least 40 s at >7 atm. For DES implantation, after pre-dilation, a size-matched DES based on IVUS imaging was placed in the lesion and released. A high-pressure balloon with appropriate dimensions was selected for post-stenting dilation to ensure that the stent was fully expanded and adhered to the vessel wall. IVUS examination was performed after DCB and DES implantation to further evaluate the immediate postoperative efficacy and guide further treatment of stent malapposition and dissection. At the same time, postoperative IVUS imaging results were recorded.
In this study, DCB had a paclitaxel/iohexol matrix coating on the Bingo Drug-Coated Balloon (Bingo™, Yinyi Biotech, Dalian, China). And the IVUS imaging were done with
the computer program (H749A70200,Boston Scientific, Shanghai, China).
Analysis Parameters
Basic patient information was collected, including sex, age, clinical diagnosis, left ventricular ejection fraction (LVEF), history of hypertension, hyperlipidemia, diabetes, smoking, myocardial infarction, previous PCI, previous coronary artery bypass grafting (CABG), and family history of coronary heart disease.
Quantitative coronary angiography (QCA) software was used to analyze the CAG data of all patients, including (1) preoperative and immediate postoperative reference vessel diameter (RFD), minimal luminal diameter, and diameter stenosis; (2) MLD, DS, LLL, restenosis lesions, and lumen enlargement at follow-up.
The IVUS analysis were also evaluated, including preoperative and immediate postoperative vessel area, plaque burden, and lumen area. Because the PB ≥70% was the strongest independent predictor of subsequent lesion-related events in the first PROSPECT study, and Gregg et al defined vulnerable plaque with this PB threshold.17,24 In this study, the PB criterion was selected to define a vulnerable plaque, and the result of CAG and IVUS were evaluated by two experienced researchers.
All patients passed the outpatient or telephone assessment 1, 3, 6, and 12 months after PCI. Major adverse cardiovascular events during hospitalization and follow-up were target lesion revascularization (TLR), myocardial infarction (MI), and cardiac death.
Statistical Analysis
SPSS version 22.0 (IBM Corporation, Armonk, NY, USA). was used for statistical analysis. Quantitative data that conformed to normal distribution were analyzed by t-test and expressed as mean ± standard deviation (SD); those that did not conform to normal distribution were analyzed by Wilcoxon rank-sum test and expressed as median and quartile range (M (P25, P75)). Qualitative data were compared using the chi-square test. If T ≤ 5, the continuity-corrected chi-square test and Fisher's exact probability test were used and expressed as number of cases (%). A Kaplan-Meier curve was used to describe survival analysis. Two-tailed P < 0.05 indicates a statistically significant difference.
Results
Baseline Demographic and Clinical Characteristics
A total of 123 patients were included in this study, of whom 55 received DCB and 68 received DES. As shown in Table 1, there were no statistically significant differences between the DCB and the DES groups in terms of average age, gender distribution, ejection fraction, and other clinical characteristics (P > 0.05). Coronary heart disease-related risk factors such as hypertension, hyperlipidemia, diabetes, and smoking history were also not significantly different between the two groups (P > 0.05). Similarly, there were no significant differences in clinical diagnosis of ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, and unstable angina pectoris between the two groups (X2 = 0.92,P>0.05).
Baseline Patient Characteristics of the Study Population.

Comparing two data sets using the continuity corrected chi-square test; DCB: drug coated balloon, DES: drug-eluting stent; STEMI :ST-segment elevation myocardial infarction, NSTEMI: non-STEMI; MI :myocardial infarction; PCI :percutaneous coronary intervention; CABG: coronary artery bypass grafting; LVEF: Left Ventricle ejection
Procedural Characteristics of PCI
By combining preoperative ECG and echocardiography and intraoperative CAG results, the culprit vessels in ACS patients were diagnosed and PCI was performed. The target vessel locations included left anterior descending artery, left circumflex artery, right coronary artery, and ramus coronary artery, and there were no statistically significant differences in target vessel locations between the DCB and DES treatment groups(X2 = 2.83,P>0.05). According to intraoperative CAG, coronary artery lesions in the two groups were divided into single vessel disease, double vessel disease, and triple vessel disease, and there were no significant differences in multivessel disease between the two groups (X2 = 0.01,P>0.05). Except for the significant difference in intraoperative balloon usage between the two groups (X2 = 7.69,P<0.05), there were no statistical differences in other PCI procedural characteristics, including implantation diameter and length, number of patients with intraoperative dissection, number of patients with temporary pacemakers, and number of patients using intra-aortic balloon pump(IABP)(P > 0.05). The procedural characteristics of PCI in the two groups are shown in Table 2.
Procedural Characteristics of PCI.

Comparing two data sets using the continuity corrected chi-square test #Comparing two data sets using the Fisher's exact probability test; DCB: drug coated balloon, DES: drug-eluting stent; IABP: intra-aortic balloon pump
QCA and IVUS Analysis
The preoperative, postoperative and follow-up results of PCI are shown in Table 3. There were no significant differences in preoperative RFD, MLD and DS between the two groups (P > 0.05). However, CAG immediately after DCB or DES implantation showed significantly smaller MLD and greater degree of stenosis in the DCB group than in the DES group (P < 0.05). Further follow-up CAG after PCI revealed that there were no statistically significant differences in MLD, stenosis degree, and coronary restenosis between the two groups (P > 0.05), except that compared to the DES group, the DCB group had less LLL in lumen diameter and a greater number of lumen enlargements (P < 0.05).
Comparison of Coronary QCA and IVUS Results Between DCB and DES Groups.
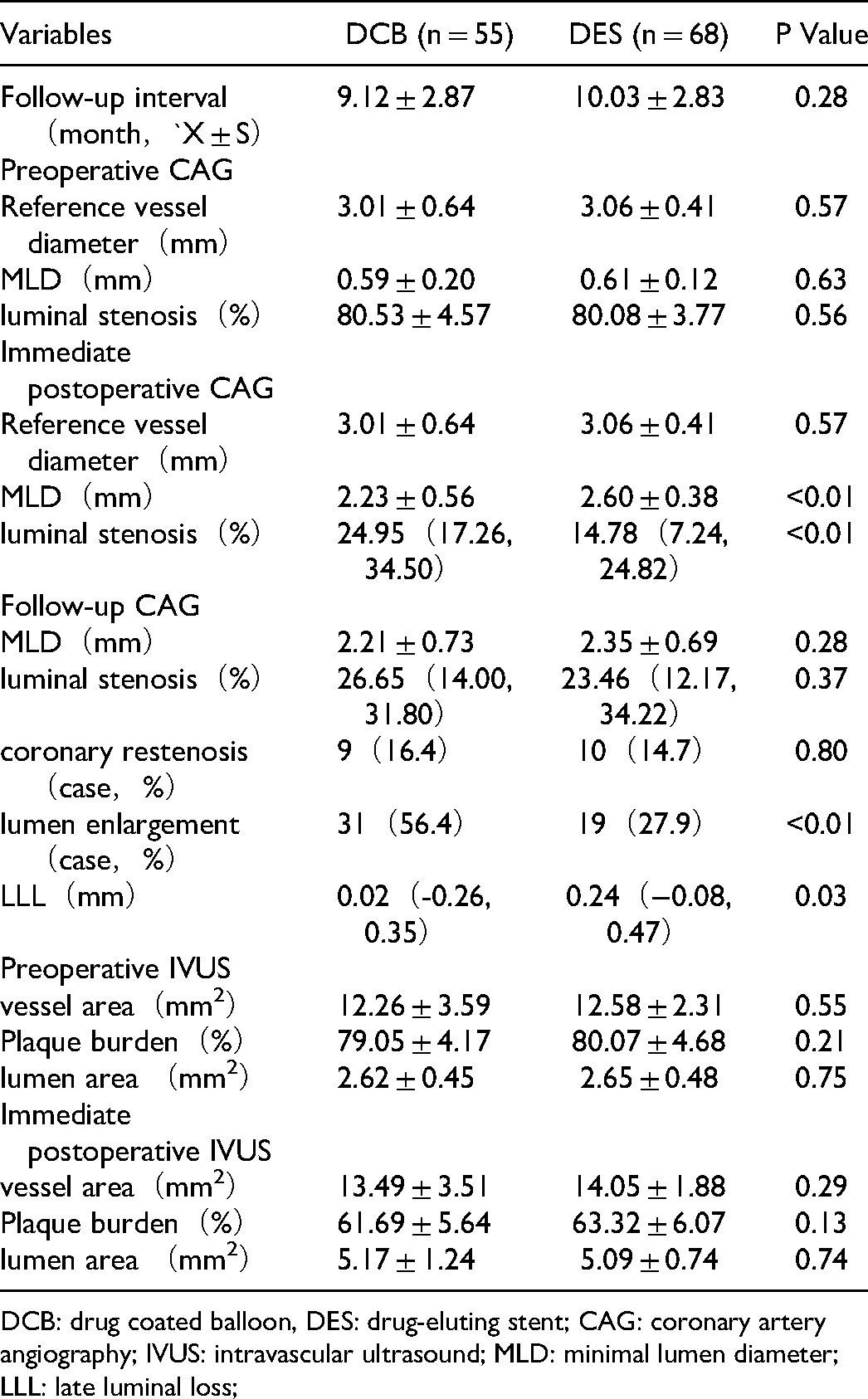
DCB: drug coated balloon, DES: drug-eluting stent; CAG: coronary artery angiography; IVUS: intravascular ultrasound; MLD: minimal lumen diameter; LLL: late luminal loss;
Both groups underwent IVUS before and after PCI. The results showed that there were no significant differences in vessel area and lumen area between the two groups (P > 0.05). In addition, no statistically significant differences were seen in preoperative plaque burden (79.05 ± 4.17 VS 80.07 ± 4.68)and postprocedural plaque burden (61.69 ± 5.64 VS 63.32 ± 6.07)between the two groups (P > 0.05).
Follow-up MACE
During the follow-up period, there were no significant differences in target lesion revascularization, myocardial infarction, and cardiac death between the two groups (P > 0.05). And survival analysis shows that there were no significant differences in the survival rate of the two groups (Log-rank,X2 = 0.01,P > 0.05). The detailed data are shown in Table 4 and Figure 2.
Comparison of MACE Between DCB and DES Groups.

Comparing two data sets using the continuity corrected chi-square test; #Comparing two data sets using the Fisher's exact probability test; DCB: drug coated balloon, DES: drug-eluting stent; MACE: major adverse cardiovascular event; TLR: target lesion revascularization; MI: myocardial infarction.
Discussion
DES is the preferred strategy for reperfusion in patients with ACS. However, delayed healing and vascular remodeling of the vascular endothelium often occur after DES implantation due to the vulnerability of the plaque and the hypercoagulable state and persistent inflammation caused by residual metals, leading to a greatly increased risk of late in-stent thrombosis.10,25 As a new strategy for the treatment of coronary artery disease, DCB has achieved reliable efficacy in various types of coronary artery disease such as in-stent stenosis due to its unique drug release behavior and no residual metal substances. Similarly, DCB has also been used in ACS lesions, but little is known about the effect of plaque vulnerability on the efficacy of DCB in ACS patients.
At present, there are many ways to identify vulnerable plaques, and each imaging method, whether invasive or non-invasive, has different diagnostic criteria. Gregg et al noted that PB ≥ 70% or MLA ≤ 4.0 mm2 on IVUS are the strongest independent predictors of subsequent MACE after PCI.17,26–30 Therefore, this study similarly adopted this criterion to define vulnerable plaque. We also analyzed IVUS in the DCB and DES groups before and immediately after PCI. We found no significant differences in vessel area, PB, and lumen area between the two groups, indicating that DCB has comparable effects on vulnerable plaques and luminal structure immediately after implantation in ACS patients compared to DES. Nevertheless, the long-term efficacy of DCB is unclear, as patients in both groups did not undergo IVUS during follow-up for economic or other reasons. It has been reported that during IVUS follow-up of DCB in the treatment of native vessel lesions, DCB was found to stabilize plaques by reducing PB and altering plaque composition, thereby reducing subsequent adverse events caused by plaque rupture. 31,32 Whether this effect of DCB appears in the treatment of ACS complicated with vulnerable plaques warrants further IVUS follow-up analysis.
In this study, CAG was performed before both DCB and DES implantation, and there were no significant differences in preoperative MLD and DS between the two groups. For the immediate postoperative CAG results showing that the DCB group had a smaller MLD and greater degree of stenosis than the DES group, one possible reason is that DCB, as a transport tool for antiproliferative drugs, lacks the effective support of metal nets like DES. Secondly, in the DES group, to ensure the full contact between the stent and the blood vessel, a high-pressure balloon of suitable size was used for post-dilation, which can allow the DES to dilate diseased vessels more effectively, reduce the elastic recoil of vessels, and ultimately prevent lumen stenosis. 33 For DCB-PCI, in addition to adequate pretreatment prior to implantation to avoid the occurrence of dissection, the lumen size and lesions had been evaluated by IVUS to minimize the difference in vasodilation with DES.
Follow-up CAG results showed that there were no significant differences in MLD and DS between the two groups, but the DCB group had smaller LLL and greater lumen enlargement. There are multiple reasons for these results. First, unlike patients in previous studies, patients in this study had a higher PB and a higher proportion of patients in the DCB group used cutting balloons or spinous balloons than in the DES group, which may allow for a more complete and uniform dispersion of the internal and medial plaques. Second, compared to DES, DCB has a larger contact area with the diseased arterial segment, enabling the antiproliferative drugs to diffuse uniformly and rapidly to the diseased vessel. Further, the residual metal stent material and long-term sustained release of anti-proliferative drugs in the DES group could lead to delayed endothelialization and inflammatory response, while in the DCB group, the arterial vasomotor and dilatation functions were relatively stable because there was no metal residual problem, which may be the reason for the late lumen enlargement. All these factors together resulted in better vascular remodeling and then less lumen loss diameter and greater lumen enlargement in the DCB group.34–36 On the other hand, there were no significant differences in the incidence of target lesion revascularization, myocardial infarction, and cardiac death between the two groups during follow-up, also suggesting that DCB is non-inferior to DES in long-term outcomes.
Limitations
This study has certain limitations. As a retrospective, single-center, and small-sample study, there may be patient selection bias. Second, although CAG was performed during follow-up in both groups, we had to assess MLD using QCA immediately after PCI due to the lack of IVUS imaging during follow-up. These limitations may have affected the results to some extent. Therefore, to further validate our conclusions, multiple interventional methods such as optical coherence tomography(OCT), virtual histology IVUS (VH-IVUS), and near-infrared spectroscopy (NIRS) can be used to comprehensively detect and identify vulnerable plaques to achieve accurate diagnosis of lesions. In addition, multicenter, large sample, and longer follow-up studies are needed.
Conclusion
In summary, DCB is safe and effective in the treatment of ACS complicated with vulnerable plaque, and DCB has the advantage over DES in LLL. Our work provides practical experience in the interventional treatment of vulnerable plaques in ACS.
Footnotes
Acknowledgments
The study was supported by the National Natural Science Foundation of China Youth Fund (no. 82000454), the Joint project of Medical Science and Technology Research of Henan (no. LHGJ20190092)
Author Contributions
(I)Conception and design of the research: Yu-Bin Zhang, Heng-Dao Liu, Jun-Hui Xing,and Hailong Tao; (II)Provision of study materials or patients:All authors. (III)acquisition of data: Yu-Bin Zhang, Bo-Wen Chen, Yan-Yan Zhao; analysis and interpretation of data: Hengdao Liu, Heping Gu, Shilong Zhou, Yanyan Zhao,Yang Lu; (IV)statistical analysis:, Yu-Bin Zhang, Heng-Dao Liu, Jun-Hui Xing; (V)drafting the manuscript: Yu-Bin Zhang, Heng-Dao Liu, Jun-Hui Xing,and Hai-Long Tao;(VI) revision of manuscript for important intellectual content: Yu-Bin Zhang, Heng-Dao Liu, Jun-Hui Xing, Hailong Tao and Heping Gu. All authors read and approved the final manuscript.
Consent for Publication
Written informed consent for publication was obtained from each author, and there are no other individuals who satisfy the criteria for authorship but who are not listed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the National Natural Science Foundation of China Youth Fund, the Joint project of Medical Science and Technology Research of Henan, (grant number no. 82000454, no. LHGJ20190092)
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethical Approval
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Zhengzhou University.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because this study was designed retrospectively, and the need to obtain informed consent from eligible patients was waived by the ethics committee.