
Abstract
Objective
To evaluate the efficacy and safety of anticoagulant therapy in patients with cirrhotic PVT, and compare differences in efficacy and safety among different anticoagulants.
Methods
We comprehensively searched Pubmed, Cochrane Library, EMBASE, and ClinicalTrials.gov from inception to April 2022 for studies using anticoagulants for cirrhotic PVT. Meta-analysis was performed to calculate odds ratios (ORs) with 95% confidence intervals (CIs).
Results
3 RCTs and 14 cohort studies involving 1270 patients were included. Anticoagulant therapy can increase the recanalization rate compared with non-anticoagulation therapy (OR 4.44, 95% CI 3.11-6.32, I2 = 2.5%) and can decrease the extension rate of cirrhotic PVT (OR 0.33, 95% CI 0.18-0.62, I2 = 41.0%), without increasing the incidence of total bleeding (OR 1.21, 95% CI 0.75-1.97, I2 = 9.8%), major bleeding (OR 0.98, 95% CI 0.49-1.95, I2 = 19.7%), and variceal bleeding (OR 0.35, 95% CI 0.12-1.01, I2 = 39.9%). Subgroup analysis showed that VKA, LMWH, and DOACs could increase the recanalization rate of PVT and were not associated with the risk of bleeding. Studies that compared direct oral anticoagulants (DOACs) with warfarin directly showed that the recanalization rate of PVT in the DOACs group might be higher than that in the warfarin group (OR 30.99, 95% CI 7.39-129.87, I2 = 0.0%), and there was no difference in the rate of total bleeding (OR 0.30, 95% CI 0.01-8.65, I2 = 79.6%).
Conclusions
Anticoagulants are safe and effective in patients with cirrhotic PVT. The rate of PVT recanalization associated with DOACs may be higher than warfarin.
Portal vein thrombosis (PVT) is a common complication of liver cirrhosis, and the incidence is about 5%∼20%.1,2 The pathogenesis of cirrhotic PVT is related to decreased portal blood flow and hypercoagulability. The existence of PVT increases mortality and graft failure after liver transplantation and is life-threatening when extended to the mesenteric vein. 3 Recent studies have shown that recanalization of PVT is associated with better survival. 4 Therefore, it is necessary to treat PVT for patients with liver cirrhosis.
Concerns about anticoagulant therapy of PVT are portal hypertension and esophageal varices are common complications in patients with liver cirrhosis, which can lead to variceal bleeding, 5 and anticoagulant therapy may have the risk of increasing the incidence of bleeding. Besides, since patients with liver cirrhosis are in a state of “rebalance”, the spontaneous recanalization of PVT was observed and the pooled rate was 39.8%. 6 Thus, it is still controversial whether to conduct anticoagulant therapy for patients with cirrhotic PVT because of the unclear bleeding risk and prognosis of anticoagulant therapy. 7 As the safety and efficacy of anticoagulants for cirrhotic PVT are still insufficient, the American College of Gastroenterology (ACG) clinical guideline 8 did not recommend anticoagulant therapy for all cirrhotic PVT patients and suggested weighting the risk of bleeding against benefits. In addition, the guidelines only suggested heparin or low molecular weight heparin (LMWH) for PVT to initiate anticoagulation and did not mention other anticoagulants. The optimal anticoagulant regimen is still uncertain. In this study, we conducted a systematic review and meta-analysis to compare the efficacy and safety of anticoagulants and the differences among different anticoagulants.
Methods
This systematic review and meta-analysis were reported by the PRISMA statement. 9 The protocol was registered in the PROSPERO (Number CRD42021251163).
Literature Search
We performed an extensive search for all available studies in English indexed in PubMed, Cochrane Library, and EMBASE from inception to April 2022. We used MeSH terms and free texts on cirrhotic PVT and anticoagulants to collect RCTs and observational studies that evaluated the efficacy and/or safety of anticoagulants for patients with cirrhotic PVT. The search strategies was shown in Appendix 1. In addition, we performed a manual search for relevant studies through ClinicalTrial.gov and the reference lists of all included studies.
Study Selection
Two authors (Zhang Z, Zhao Y) independently reviewed the titles and abstracts according to the following inclusion criteria: (1) studies using anticoagulants including LMWHs, vitamin K antagonists (VKA), direct oral anticoagulants (DOACs), for patients with cirrhotic PVT; and (2) patient's age ≥ 18. Then three authors (Zhang Z, Zhao Y, Han B) screened the full texts for the final inclusion. We resolved discrepancies through discussion or consultation with another reviewer (Dr Cui X). The exclusion criteria included: (1) studies using anticoagulants for preventing PVT; (2) non-drug anticoagulation of cirrhotic PVT such as transjugular intrahepatic portosystemic shunt (TIPs); (3) malignant PVT; (4) splanchnic vein thrombosis without portal vein involvement; and (5) studies with duplicate data, abstracts only or non-English studies.
Data Extraction
Three authors (Zhang Z, Zhao Y, Han B) extracted data into predesigned tables. The following information was collected: (1) Characteristics of the studies, including the name of the first author, year of the publication, type of study; (2) baseline characteristics of included patients. Such as age, gender, INR, creatinine, platelet count, and hemoglobin; (3) Anticoagulants used in the studies, including dosage, duration of treatment and follow-up; and (4) Outcomes of the anticoagulants, including the recanalization and extension of PVT, and bleeding events. The recanalization of PVT included partial and complete recanalization of the thrombus in the main portal vein and its branches. The partial recanalization was defined as at least a 30% reduction in the long diameter and/or 50% reduction in the cross-sectional area of the main thrombus, without evidence of thrombus extension. Bleeding events included variceal bleeding and major bleeding. The major bleeding events were determined according to the International Society on Thrombosis and Haemostasis criteria or as reported.
Risk of Bias Assessment
We used Cochrane risk-of-bias tool to assess the risk of bias in RCTs. The Newcastle-Ottava Scale (NOS) 10 was used for the risk of bias in observational studies, and the quality was high when studies got more than 7 stars.
Statistical Analysis
We performed a meta-analysis to compare PVT recanalization and bleeding events between the anticoagulant group and the non-anticoagulant group, and among the different anticoagulant groups. We pooled and compared the data by random-effect model and used the inverse-variance method to calculate the odds ratios (OR) with 95% confidence intervals (CIs). The I2 statistic was used to assess the heterogeneity, with substantial heterogeneity defined when I2 is greater than 50%. 11
We performed subgroup analysis and meta-regression to evaluate the safety and efficacy of different anticoagulants and explore the source of heterogeneity. We performed sensitivity analysis on the results, and funnel plot to assess the presence of publication bias. The publication bias was solved by the "trim and fill" test. A P-value of <0.05 suggests a statistical significance. All analyses were performed with the software Stata (version 15.1, USA).
Results
We retrieved 579 studies by our search strategies. Among these, 149 were removed because of the duplication, and then 430 studies were identified. After abstracts and full texts screening, 17 studies involving 1270 patients were included, which included 3 RCTs and 14 cohort studies (Appendix 2). These studies were published from 2005 to 2022 with sample sizes ranging from 11 to 214. Baseline characteristics of included patients was shown in Table 1. Most patients were male, average age ranged from 41.3 to 69. The quality of the included study is shown in Appendix 3, 4.
Baseline Characteristics of the Studies included in this Meta-Analysis.

*The units of platelet count are converted into 10^9/L; time units are converted into months, 30 days = 1 month, 12 month = 1 year. Data are mean ± SD.
Abbreviations: M, male; F, female; INR, international normalized ratio; m, months; U, units; IQR, interquartile range; NA, not available; NR, no report.
Efficacy and Safety of Anticoagulant Group Versus non-Anticoagulant Group
13 studies had compared the anticoagulant group with the non-anticoagulant group, 12 of them were observational studies and one was a single-blind RCT study. In terms of efficacy, the meta-analysis showed the recanalization rate of PVT in the anticoagulant group was higher than that in the non-anticoagulant group (OR 4.44, 95% CI 3.11-6.32, I2 = 2.5%) (Figure 1). Anticoagulants can increase both the rate of complete recanalization (OR 3.49, 95% CI 2.40-5.06, I2 = 0.0%) and partial recanalization (OR 2.69, 95% CI 1.27-5.57, I2 = 26.3%). In addition, the anticoagulant group was associated with a lower rate of PVT extension (OR 0.33, 95% CI 0.18-0.62, I2 = 41.0%). Subgroup analysis showed that VKA, LMWH, and DOACs could increase the recanalization rate of PVT. Meta-regression analysis showed that gender, age, INR, hemoglobin, creatinine, platelet count, follow-up time, and anticoagulation duration were not the sources of heterogeneity in recanalization and extension rate of the anticoagulants (Appendix 5).
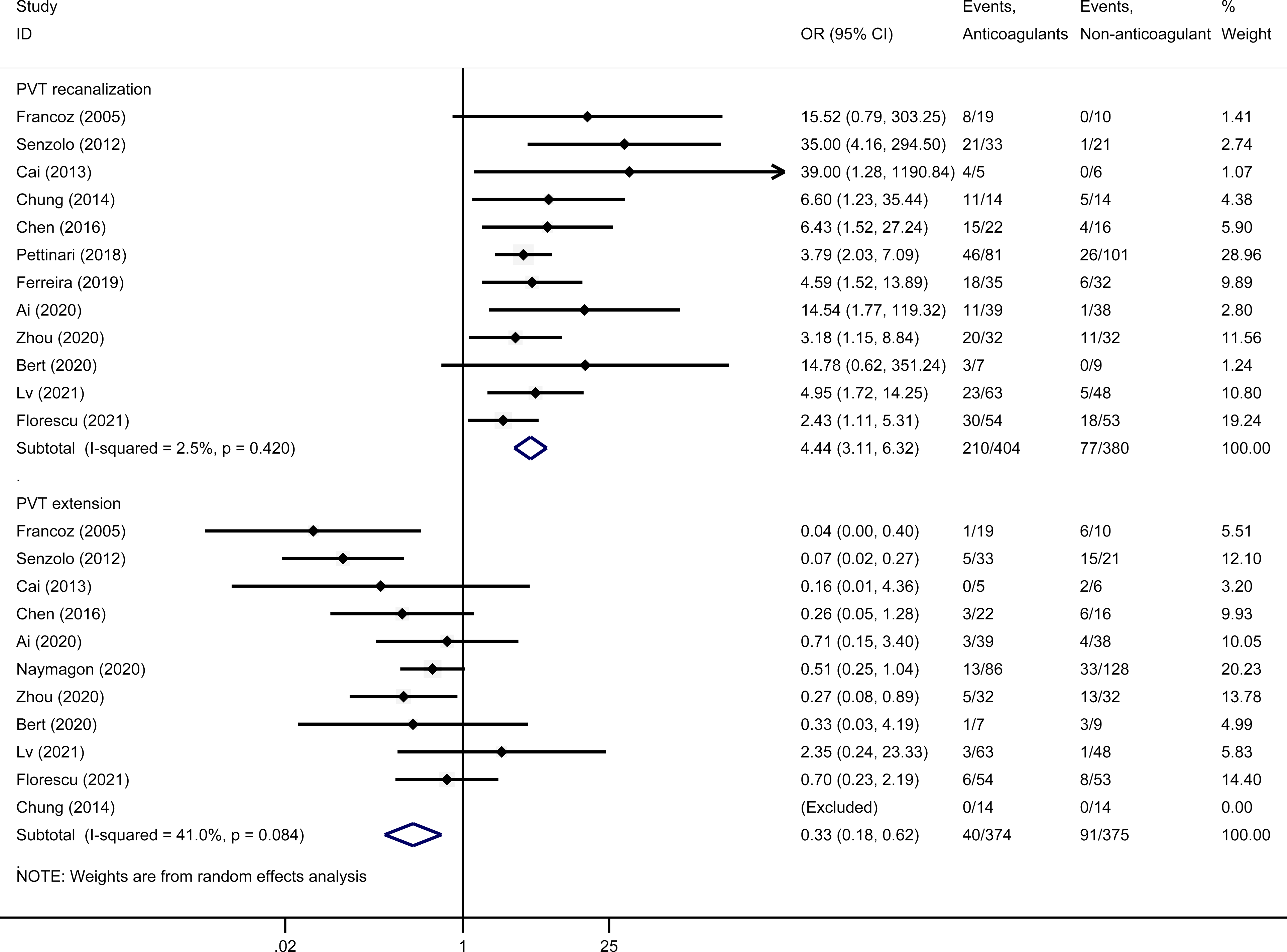
PVT recanalization and extension of anticoagulants versus non-anticoagulant group.
In terms of safety, there was no significant difference in the rate of total bleeding (OR 1.21, 95% CI 0.75-1.97, I2 = 9.8%), major bleeding (OR 0.98, 95% CI 0.49-1.95, I2 = 19.7%), and variceal bleeding (OR 0.35, 95% CI 0.12-1.01, I2 = 39.9%) between the anticoagulant group and non-anticoagulant group (Figure 2). And different anticoagulants were not the source of heterogeneity in bleeding rate (Appendix 5).

Bleeding events of anticoagulant group versus non-anticoagulant group.
Efficacy and Safety of DOACs Versus Warfarin
According to the studies that compared DOACs with warfarin directly, the recanalization rate of PVT in the DOACs group might be higher than that in the warfarin group (OR 30.99, 95% CI 7.39-129.87, I2 = 0.0%). The extension rate of PVT in the DOACs group might be lower than that in the warfarin group (OR 0.08, 95% CI 0.01-0.45, I2 = 0.0%). There was no difference in the rate of total bleeding (OR 0.30, 95% CI 0.01-8.65, I2 = 79.6%), major bleeding (OR 0.16, 95% CI 0.02-1.39, I2 = 0.0%), and variceal bleeding (OR 0.12, 95% CI 0.00-6.06, I2 = 77.1%) between the DOACs group and warfarin group (Figure 3).
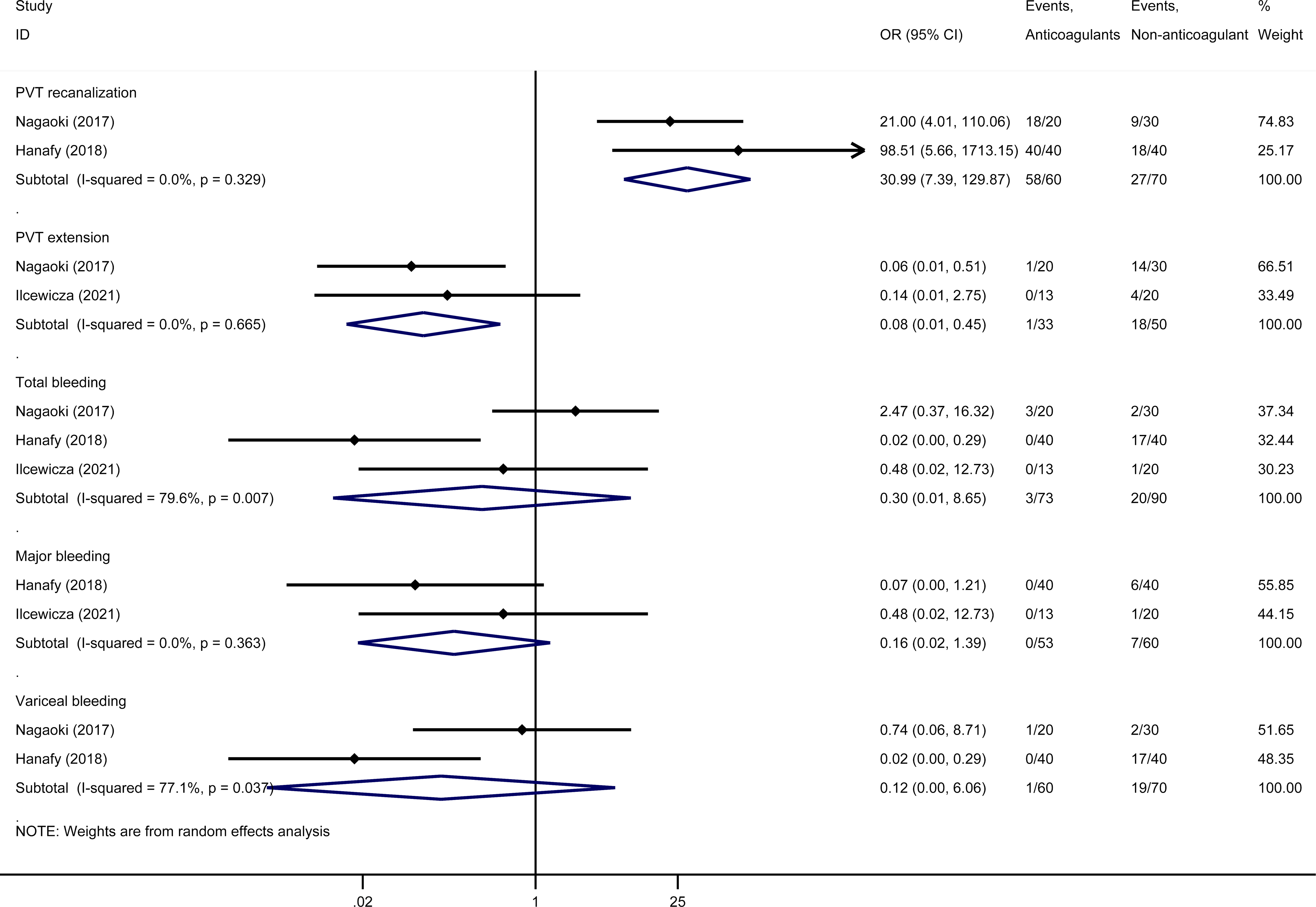
Efficacy and safety of DOACs versus Warfarin.
Sensitivity Analysis and Publication Bias
We excluded one study at a time, and when Florescu's study was excluded, the anticoagulant group had a lower rate of variceal bleeding than the non-anticoagulant group (OR 0.21, 95% CI 0.09-0.51, I2 = 0.0%). None of the studies had a significant impact on other results. The figure of sensitivity analysis can be seen in Appendix 6. There was visible gross asymmetry observed in the funnel blot, suggesting publication bias (Appendix 7. Supplementary Figure 6). We used the "trim and fill" test to adjust the funnel chart without significantly changing the results.
Discussion
In this meta-analysis, we found that anticoagulants were associated with an increased rate of PVT recanalization and a reduced rate of PVT extension. Anticoagulants did not increase the rate of total bleeding, major bleeding, and variceal bleeding. Besides, the meta-analysis of different anticoagulants showed the PVT recanalization rate of DOACs might be higher than VKA.
Consistent with previous meta-analyses,29,30 we found the efficacy of anticoagulation treatment for cirrhotic PVT can promote the PVT recanalization without increased risk of bleeding. American Gastroenterological Association (AGA) 31 Clinical Practice pointed out that the use of warfarin or heparin-derived medications was associated with increased rates of recanalization. This was confirmed in our study along with the fact that DOACs may have a similar effect.
For a long time, there is insufficient information on the efficacy of DOACs for cirrhosis. Current guidelines 8 do not recommend the use of DOACs to treat PVT in patients with cirrhosis. In this study, we found that DOACs was non-inferior to warfarin in safety and efficacy. Warfarin is the most commonly used oral anticoagulant, but the food-drug interaction and INR monitoring increase the misgiving of doctors prescribing anticoagulants and hinder patient compliance. Besides, the baseline prothrombin time was prolonged and baseline INR was increased in patients with cirrhosis and PVT, which may make warfarin based on the regular prothrombin time-INR underdosed in cirrhosis. 32 But in terms of DOACs, they are not needed to adjust the dosage based on INR. This may be the reason why DOACs have a higher rate of recanalization and a lower rate of PVT extension than warfarin. DOACs have the advantage of not requiring dose adjustment by laboratory testing which brings better compliance and cost-effectiveness. Therefore, DOACs have the potential to become one of the alternatives for anticoagulant therapy for cirrhotic PVT. But more studies comparing different anticoagulants are still needed to confirm our conclusions.
The risk of bleeding was the concern for the clinical application of anticoagulants in the treatment of cirrhotic PVT. Neither our study nor previous meta-analysis found using anticoagulants can increases the risk of bleeding. Our study also found that anticoagulants did not increase the rate of major bleeding. These findings supported using anticoagulants in patients with cirrhotic PVT. During the clinical practice, patients should be closely monitored for signs of bleeding, and reversal agents 33 should be used to terminate the anticoagulant effect in time when major bleeding occurred.
The ACG clinical guideline 8 suggested that anticoagulation is not associated with an increased risk of variceal bleeding in patients with cirrhotic PVT and the presence of gastroesophageal varices is not a contraindication to anticoagulation. A previous meta-analysis concluded that anticoagulants could reduce the incidence of variceal bleeding (0.1% vs 18.5%; RR 0.15, 95%CI 0.04-0.55; P = 0.004). 29 Recanalization of PVT has been reported to reduce esophageal variceal pressure, 34 which may lead to the reduction of variceal bleeding. Our study suggested that there was no significant difference in variceal bleeding between the anticoagulant group and non-anticoagulant group after including more studies. However, the results had changed after Florescu's study was excluded in the sensitivity analysis. The weight of Florescu's study accounts for 27.34% of the results, so we should be paid attention to its result. This suggests that more studies on the effect of anticoagulants on the variceal bleeding rate are needed to confirm this conclusion.
Several meta-analyses29,30,35 have been published recently on anticoagulant therapy for portal PVT in cirrhosis. We included more studies and patients than Ghazaleh's study. Compared with the study conducted by Chen and Koh et al, we had stricter inclusion criteria as the population of our study was strictly defined as patients with cirrhosis and portal vein thrombosis. And we excluded the abstract-only studies because the populations and outcomes of those studies were difficult to define. Besides, we not only compared both the anticoagulant group versus the non-anticoagulant group and also different anticoagulants.
Our study has several limitations. First of all, most of the studies we included were observational studies, which may decrease the level of evidence. However, RCTs present a higher level of evidence, but the strict inclusion and exclusion criteria make the research populations different from the clinical practice. Secondly, the baseline characteristics of included studies varied greatly. We collected the baseline characteristic that was risk factors of PVT and conducted a meta-regression analysis including gender, age, INR, hemoglobin, creatinine, platelet count, follow-up time, and anticoagulation duration. But no modification effects were found. The heterogeneity of the outcomes of our meta-analysis was acceptable (I2<50%). Of course, there were also risk factors that were not included in the meta-regression. For example, one study tested 20 the JAK2V617F gene, while others did not. However, only one of the 214 patients was positive, suggesting the low incidence of JAK2V617F, which may have little effect on the overall results. Furtherly, some studies excluded patients with underlying thrombogenic hematologic, pregnancy, or other situations that might affect the outcomes, while others did not mention. Further studies with strict exclusion criteria to eliminate risk factors of PVT were needed for cirrhosis patients.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221104797 - Supplemental material for The Efficacy and Safety of Anticoagulants in the Treatment of Cirrhotic Portal Vein Thrombosis: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296221104797 for The Efficacy and Safety of Anticoagulants in the Treatment of Cirrhotic Portal Vein Thrombosis: A Systematic Review and Meta-Analysis by Zhiqi Zhang, Ying Zhao, Baofeng Han, Zhijun Zhu, Liying Sun and Xiangli Cui in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.