
Abstract
With advances in modern imaging techniques, portal vein thrombosis (PVT) is being increasingly diagnosed. It has a wide ranging clinical spectrum from being an asymptomatic state to a potentially life-threatening situation. It is not unusual to find it as an incidental finding in the abdominal imagings done for other reasons. It is commonly associated with cirrhosis and abdominal malignancies and also has a strong association with prothrombotic disorders. It is often difficult for the clinicians to decide whether PVT is acute or chronic. This poses great challenges to its management strategies that include anticoagulants, thrombolysis, and surgical options. Timely diagnosis and appropriate management have great bearings on its outcomes of morbidity and mortality. In this clinician-oriented review, we have provided a concise review of clinical aspects of PVT and discussed various management strategies while addressing the common questions that come to a physician’s mind dealing with such a patient.
Introduction
Portal vein thrombosis (PVT), first described in 1868, 1 refers to the partial or complete thrombosis of the portal vein trunk, including its right and left intrahepatic branches. The PVT is an uncommon disease, but it is being diagnosed more frequently because of the increasing use of high-resolution imaging modalities such computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) Doppler. The PVT is clinically important because it may be associated with serious sequelae. It is now well established that acute and chronic PVT are successive stages of the same disease, with similar causative factors, but differ in terms of clinical management. In acute cases, PVT may be complete or partial, may extend to the superior mesenteric and splenic veins, and may also involve the branches of intrahepatic portal vein. Life-threatening bowel ischemia may ensue if the superior mesenteric vein and mesenteric venous arches become thrombosed. 2 Chronic PVT may lead to portal hypertension.
Early diagnosis and appropriate management of PVT have the potential to reduce morbidity and mortality. Although there are several reviews of PVT available, 2 –8 there are many clinical issues regarding its management that need to be addressed further. The objectives of this review are (1) to provide a concise but comprehensive overview of the key features of PVT and (2) to provide a practical approach to managing patients with PVT and address common questions that arise in practice. The Class and Level of Evidence and Strength of recommendations in the article are based on ASSLD(American Society for the Study of Liver Diseases)(Table 6 and 7) and ACCP(American College of Chest Physicians) (Table 8).
Epidemiology
In the general population, the lifetime risk of developing PVT is approximately 1%. 9 The PVT is more common in developing countries, probably due to higher rates of intraabdominal infections, and may account for portal hypertension in 30% of cases in adults and 75% of cases in children. 10 Its prevalence in patients with cirrhosis varies widely, increasing with the severity of cirrhosis, and is between 0.6% and 16%, 3 with the highest prevalence occurring in patients who require liver transplantation. In patients with liver cancer, the incidence of PVT is between 10% and 40%. 11
Etiology and Pathogenesis
In past years, PVT was often considered idiopathic, without an identifiable cause. With the more recent discovery of novel prothrombotic abnormalities, coupled with a better understanding of many predisposing clinical conditions, the etiology of PVT can be ascertained in about 70% of the cases. 3 The PVT is often multifactorial and it is not uncommon to find systemic and local causes occurring concurrently in the same patient. Local factors are present in the majority of patients with PVT. 5 Apart from cirrhosis, cancer (usually hepatic or pancreatic), and liver transplantation, the other important local causes include abdominal inflammation (such as pancreatitis and cholecystitis), abdominal trauma including abdominal surgery, and abdominal sepsis. A study found higher incidence of PVT in patients with bacteremia from bacteroides fragilis of occult source due to transient appearance of anticardiolipin antibodies. 12 Studies indicate that up to 72% of presumed idiopathic cases of PVT may be associated with thrombophilic states. 5,13 Myeloproleferative disorders and the factor V Leiden mutation are among the most common disorders associated with PVT. Prothombin gene mutation has often been reported in patients with cirrhosis with PVT, but its role in development of PVT in general population is not well-defined. Dentali et al reported an odds ratio of 1.9 for PVT in patients with factor V Leiden and 4.48 in patients with prothombin gene muatation. 14 The role of natural anticoagulant proteins (protein C, protein S, and antithrombin) in PVT is less clear as their levels may be altered as a result of hepatic injury in both acute and chronic PVT. 8 However, in some patients there may be multiple prothrombotic disorders simultaneously accounting for the development of PVT. 8,14 The JAK2 mutation (JAK2V617F), in particular, appears to be strongly associated with PVT, with an odds ratio exceeding 50. Indeed, PVT may be the first manifestation of myeloproliferative disease and routine screening for the JAK2 mutation is recommended in patients with otherwise unprovoked PVT (Tables 1 and 2). 15
Causes of Portal Vein Thrombosis (PVT).
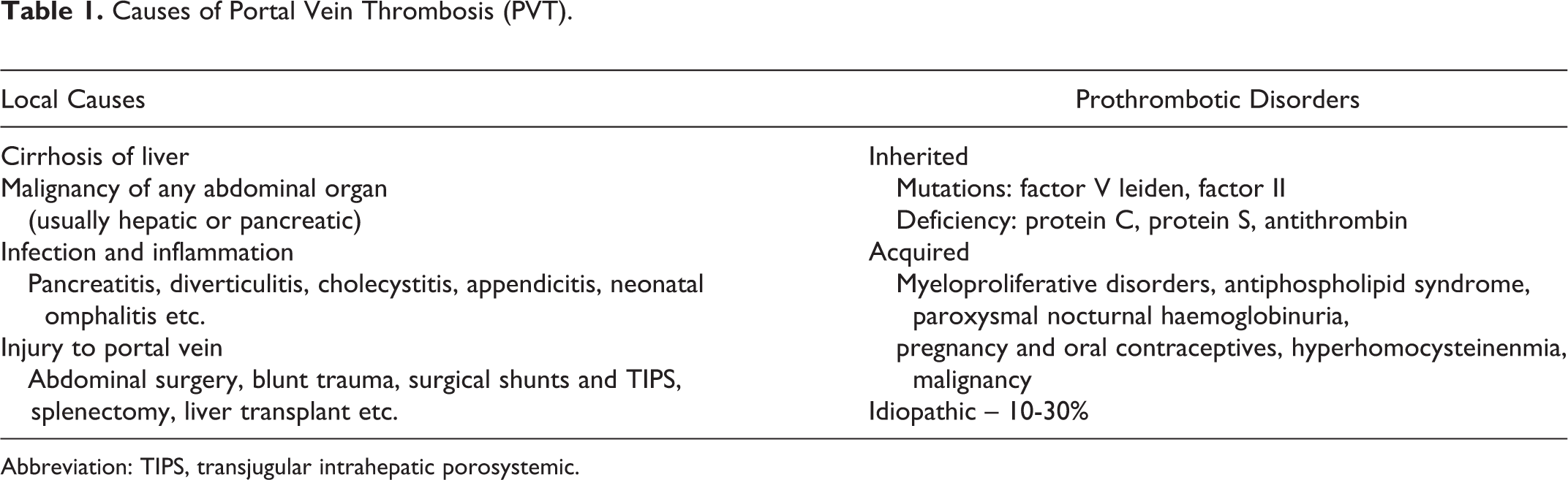
Abbreviation: TIPS, transjugular intrahepatic porosystemic.
Investigating Causes of PVT.a
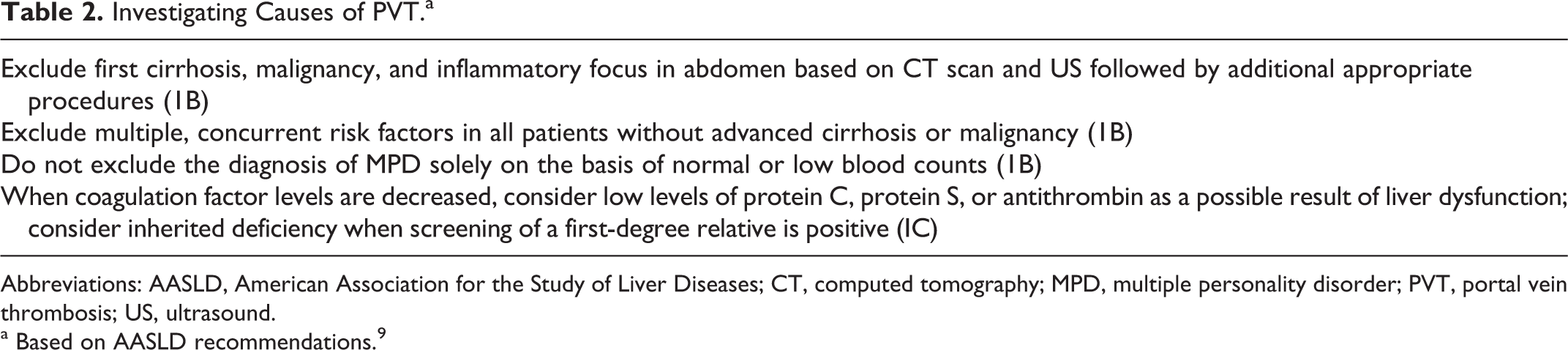
Abbreviations: AASLD, American Association for the Study of Liver Diseases; CT, computed tomography; MPD, multiple personality disorder; PVT, portal vein thrombosis; US, ultrasound.
a Based on AASLD recommendations. 9
The approach to identify the cause of PVT should initially focus on excluding local diseases such as cirrhosis, malignancy, pancreatitis, and sepsis. However, as stated above, since PVT is often multifactorial in etiology, it may be worthwhile excluding thrombophilic conditions even when there is a local cause as it might have therapeutic and prognostic connotations.
Pathophysiology
In healthy states, the liver receives two-thirds of its blood supply from the portal vein, with the remaining one-third from the hepatic artery. 16 However, complete occlusion of the portal vein in PVT may not lead to clinical consequences and the patient may remain asymptomatic. This is due to important hemodynamic changes in the systemic and splanchnic circulation brought about by compensatory mechanisms. 17 Initially, there is “arterial rescue” in which vasodilatation of the hepatic artery helps to preserve hepatic function. This is followed by “venous rescue” which results in the rapid development of collaterals to bypass the obstruction within a few days and eventual formation of a cavernoma in 3 to 5 weeks. 18 Notwithstanding these compensatory mechanisms, advanced stages of portal vein occlusion may lead to impairment of synthetic functions of the liver. 19
Clinical Features
It is customary to classify PVT as acute or chronic, but it may be sometimes difficult to apply this formulation in clinical practice. Although not universally accepted, some authors suggest that PVT may be considered acute if symptoms develop within 60 days prior to diagnosis. 5,20 –22 Another way to distinguish between acute and chronic PVT is the presence or absence of signs of portal hypertension (splenomegaly and esophageal varices) and collateral vessels on imaging. 3
Acute PVT is often asymptomatic or it may present with nonspecific abdominal pain. It is also often identified as an incidental finding on abdominal imaging studies that are done for other reasons. However, involvement of the superior mesenteric vein and the mesenteric arches may result in bowel congestion and ischemia leading to abdominal pain, vomiting, diarrhea, hematochezia, and features of sepsis complicated with shock and death from multiorgan failure. 3,5,9 Acute septic PVT, also called acute pylephlebitis, is characterized by the presence of infected thrombus in the portal vein. 9 It usually has a septic focus in the abdomen and presents with fever with chills, right upper quadrant pain, and, occasionally, hemodynamic instability.
Chronic PVT may also be asymptomatic or identified incidentally during abdominal imaging. It involves formation of periportal collaterals around the thrombosed portal vein (portal cavernoma). Such patients may present with sequelae of portal hypertension such as esophageal varices, splenomegaly, anemia, and thrombocytopenia. 3 Upper gastrointestinal bleeding may be the first manifestation in 20% to 40% of the patients with chronic PVT. 12 Rarely, some patients may develop portal cholangiopathy due to common bile duct obstruction by enlarged collateral veins. Such patients may be asymptomatic or present with jaundice, abdominal pain, or cholangitis. 22,23 On the other hand, ascites and encephalopathy are uncommon in the absence of concomitant liver disease.
In the absence of bowel ischemia, acute PVT may have good prognosis. However, mortality rates can be as high as 20% to 50% in patients with intestinal ischemia and multiorgan failure. 5,24 In chronic PVT, the prognosis largely depends on the presence of underlying cirrhosis or malignancy. Patients with chronic PVT tolerate gastrointestinal bleeding better than other forms of portal hypertension as such patients tend to be younger and have no significant liver disease. In noncirrhotic and nonmalignant cases, chronic PVT has a good prognosis with an estimated long-term mortality of <10%. 5,25 The clinical importance of incidental PVT is unknown and it is often difficult to ascertain whether thrombosis is acute or chronic. Similarly, it is not known whether treatment is required given the competing interests of increased risk of hemorrhage, for example, due to varices against an unknown risk of local or systemic complications in the absence of treatment.
Diagnosis
Diagnostic imaging: Imaging techniques used to diagnose PVT include US, CT, and MRI. Ultrasound is inexpensive, readily available, and widely used to diagnose PVT but has variable accuracy, with sensitivity and specificity varying from 66% to 100%.
3
Ultrasound demonstrates the presence of solid material in the portal vein lumen, collateral vessels (a cavernoma), and, when combined with pulsed Doppler, absent flow within the portal veins. The US with color Doppler imaging has negative predictive value of 98% for diagnosis of PVT and has become imaging modality of choice.
20,22
Endoscopic US has greater sensitivity and specificity for the diagnosis of PVT.
26
However, US has limited utility for the evaluation of mesenteric circulation. Both CT and MRI can better visualize the mesenteric vasculature and can also identify bowel ischemia and pathology in adjacent organs. Finally, positron emission tomography-CT might differentiate if PVT is associated with benign or malignant disease (Table 3).
27
Laboratory testing: Liver functions tests, including albumin, bilirubin, international normalized ratio (INR), and activated partial thromboplastin time, are usually normal unless there is concomitant cirrhosis. Common but nonspecific laboratory findings include moderately decreased coagulation factors levels and an increase in
Diagnosis of PVT.a
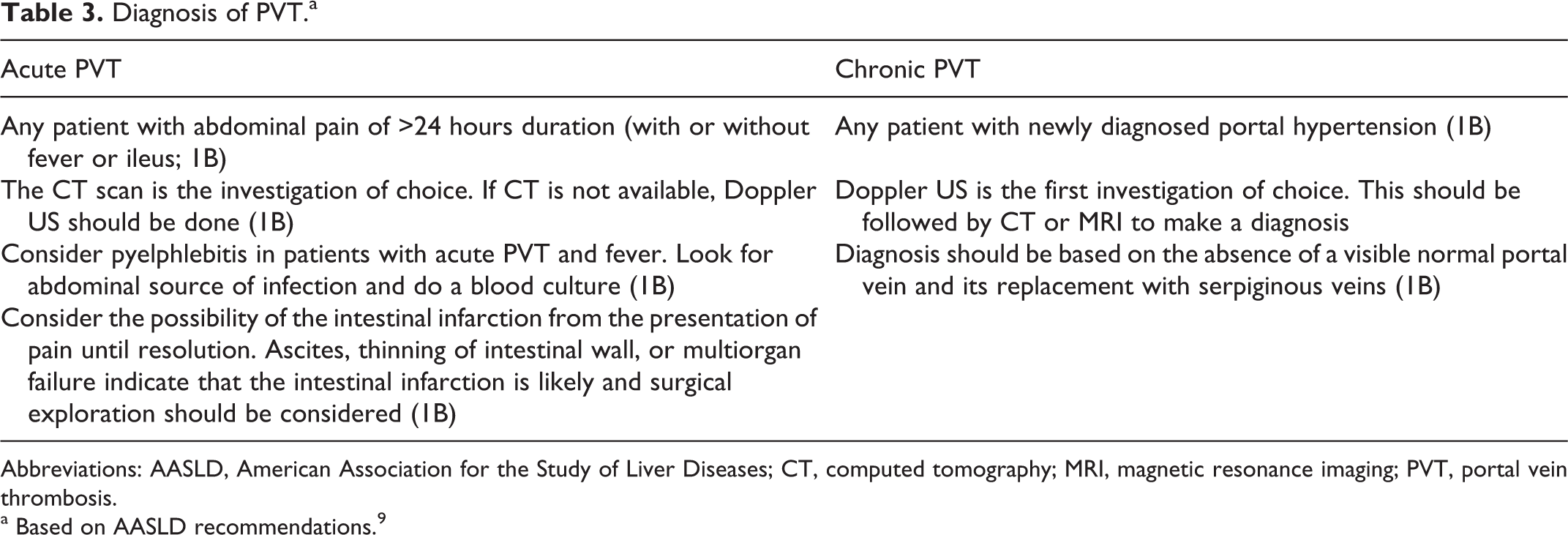
Abbreviations: AASLD, American Association for the Study of Liver Diseases; CT, computed tomography; MRI, magnetic resonance imaging; PVT, portal vein thrombosis.
a Based on AASLD recommendations. 9
Treatment
The management goals of PVT are to identify and treat underlying causes, to prevent thrombus extension, and to achieve portal vein recanalization. Although there is general agreement that anticoagulant therapy is required for most symptomatic cases of PVT, there is no consensus on the optimal type and duration of such treatment. 5 In addition to anticoagulation, thrombolysis and thrombectomy are adjunctive treatment options although thrombolysis is used infrequently and thrombectomy is used all the more rarely. Comparative clinical trials of these treatment modalities are lacking. Finally, the need for treatment (or no treatment) should also consider whether PVT is acute or chronic, the extent of thrombosis, the presence of other comorbidities such as cirrhosis and malignancy, and the presence of thrombophilia. 5 It is also noteworthy that there are sporadic case reports of recanalization of pylephlebitis with antibiotics alone (Tables 4 and 5). 8
Treatment of PVT (Based on AASLD Guidelines).9
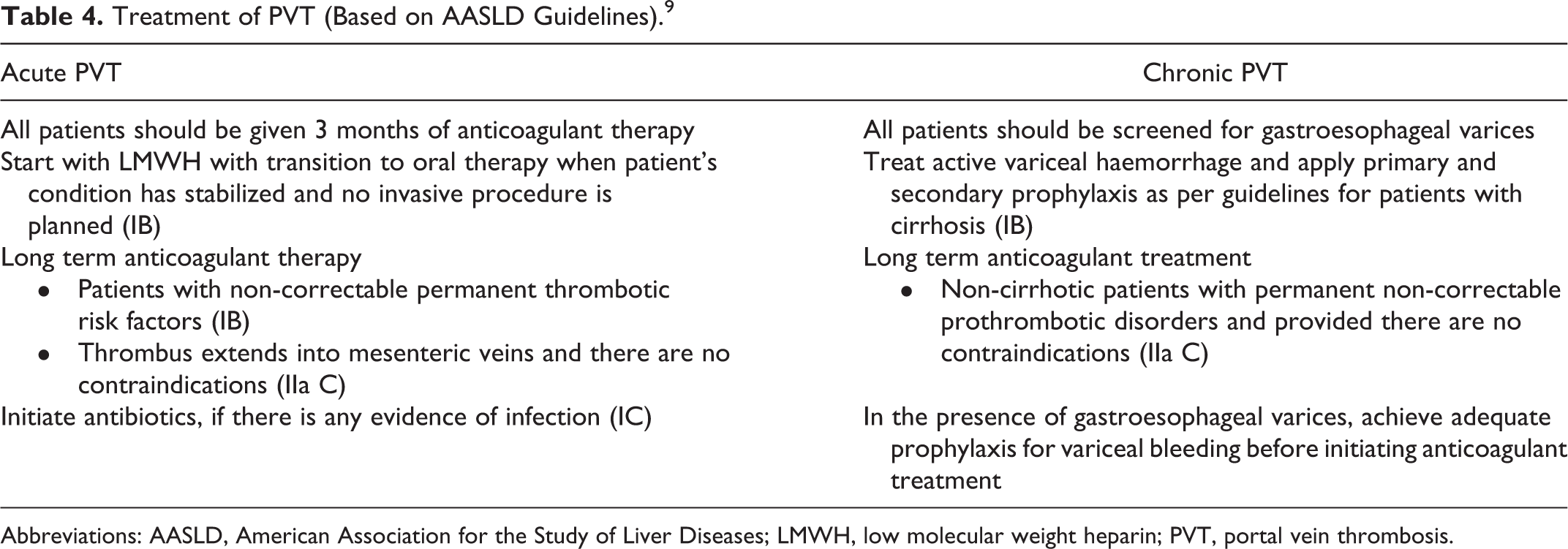
Abbreviations: AASLD, American Association for the Study of Liver Diseases; LMWH, low molecular weight heparin; PVT, portal vein thrombosis.
Treatment for PVT (Based on ACCP Guidelines). 30
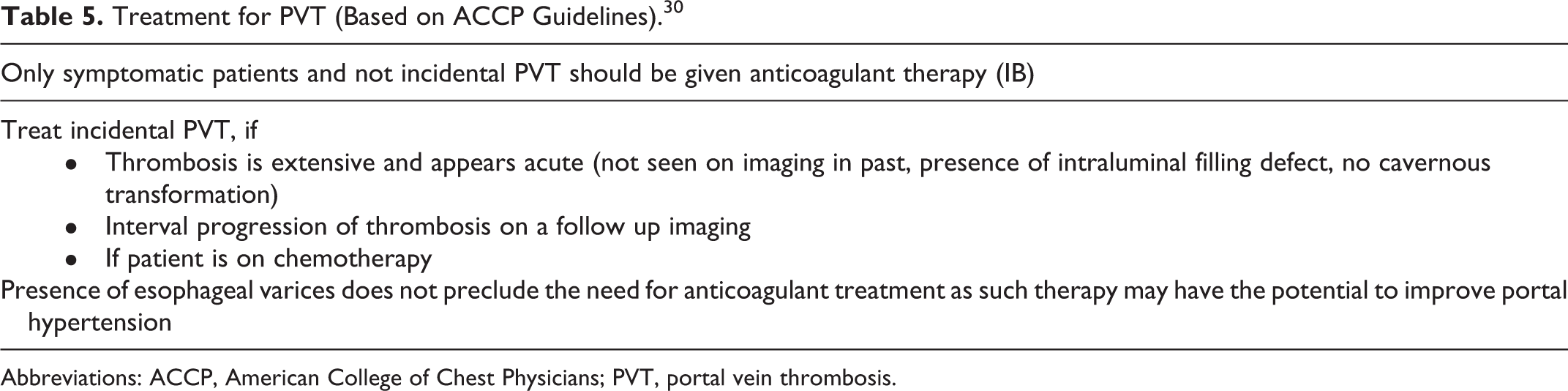
Abbreviations: ACCP, American College of Chest Physicians; PVT, portal vein thrombosis.
The AASLD Grading System for Recommendations.
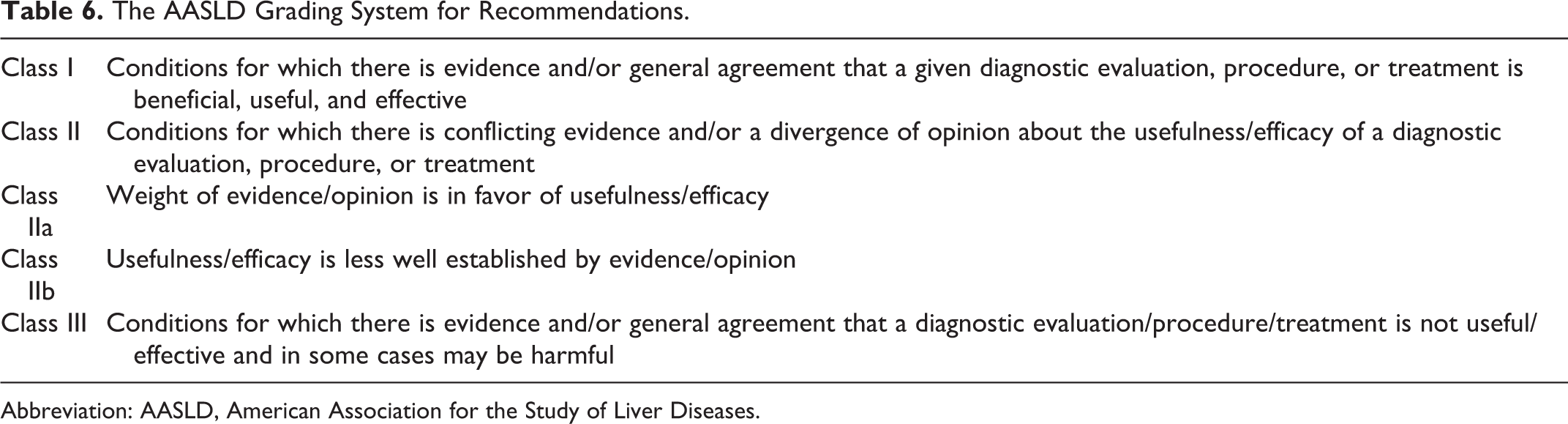
Abbreviation: AASLD, American Association for the Study of Liver Diseases.
The AASLD Level of Evidence Description.

Abbreviation: AASLD, American Association for the Study of Liver Diseases.
The ACCP: Strength of Recommendations Grading System.
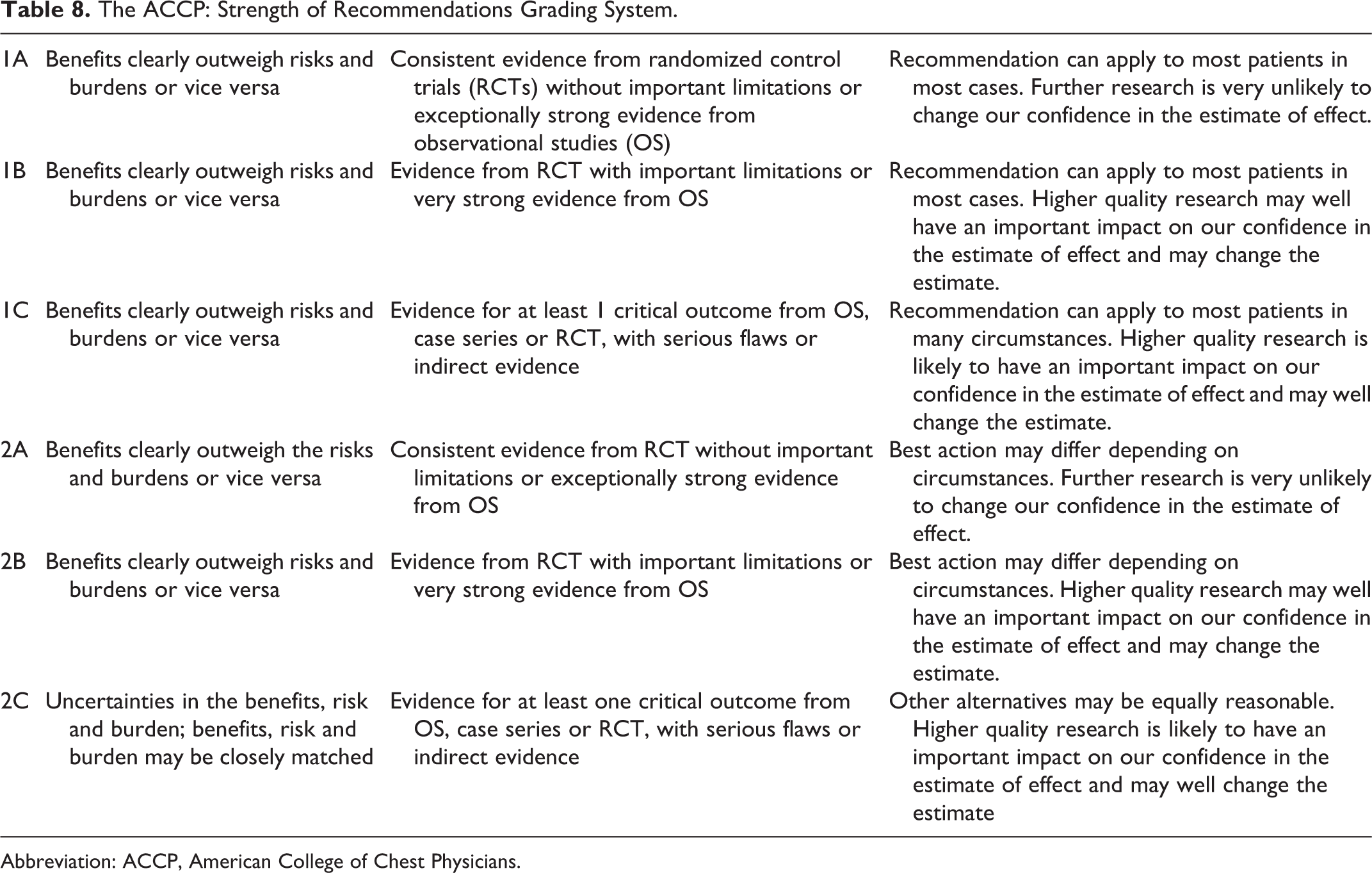
Abbreviation: ACCP, American College of Chest Physicians.
Should All Patients With PVT Receive Anticoagulant Therapy?
The uncertain natural history of PVT precludes definitive conclusions about the need for anticoagulation in all patients. Randomized trials comparing anticoagulation and nonanticoagulation approaches for PVT are lacking and, consequently, management strategies are typically individualized. Based on the findings from observational studies, spontaneous resolution of PVT without antithrombotic therapy appears to be uncommon. 29,31 –33 Thus, a systematic review of studies conducted in patients without cirrhosis or cancer reported spontaneous thrombus resolution in only 16.7% of the patients. 2
Factors favoring spontaneous thrombus resolution in PVT include self-limiting underlying diseases, less extensive thrombosis, no concomitant hepatic parenchymal disease, and no thrombophilia. 32,33 Patients with minimal or no vessel recanalization appear to have a higher rate of complications related to portal hypertension and it is prudent, therefore, to ensure early recanalization of the portal vein to decrease the subsequent risk of bleeding from esophageal varices. 34
What is Appropriate Anticoagulant Management?
Acute PVT: There is evidence from observational studies to justify the use of anticoagulants in patients with acute symptomatic PVT but randomized trials are lacking.
5,8,22
Nonetheless, anticoagulant therapy has become the de facto standard of care for the treatment of PVT and the prevention of portal hypertension.
5,22
Anticoagulant options include unfractionated heparin, low-molecular-weight heparin (LMWH), and vitamin K antagonists (VKAs). To date, there are no clinical reports on the use of the new oral anticoagulants (factor IIa or factor Xa inhibitors) for PVT. The LMWHs are often the initial choice of treatment because of their established efficacy and safety profile in other thrombotic conditions, predictable dose–response effect and ease of use, and are subsequently transitioned to VKA in most cases. Based on extrapolation of data on venous thromboembolism, a target INR of 2 to 3 is considered optimal. There is evidence that early initiation of anticoagulation is associated with more favorable outcomes. Depending upon whether anticoagulation is started within the first or second week after diagnosis, the rate of recanalization may drop from 69% to 25%.
5,11,21,29
To achieve optimal recanalization, it appears that anticoagulation should be initiated within 30 days of symptom onset.
3
However, in situations where acute PVT occurs in the immediate postoperative period or is associated with bleeding (such as hemorrhagic pancreatitis), the risk of further bleeding may preclude initiating anticoagulant therapy and repeat reassessments of the benefits and risks of anticoagulation are warranted. Anticoagulant therapy appears to result in full patency of the portal vein in 50% of the patients and partial patency in 40% of the patients.
8,31,35
–39
However, even with prompt initiation of anticoagulant therapy, up to 10% of the cases of PVT will be resistant to even partial recanalization.
31,35
–39
Further support for early initiation anticoagulation is the observation that anticoagulants improve the survival rates in cases of intestinal ischemia when started before any surgical intervention.
40
–42
Both the American Association for the Study of Liver Diseases (AASLD) guidelines and American College of Chest Physicians practice guidelines (Grade 1B) recommend that acute PVT should be treated with anticoagulants. 8,30 Based on these overall considerations, early initiation of anticoagulant therapy should be the goal for all cases of acute PVT in the absence of contraindications.
2. Chronic PVT: The need for anticoagulation for patients with chronic PVT is often uncertain, mainly because such patients are considered to have higher risk of bleeding due to frequent presence of cirrhosis or cancer, associated esophageal varices, thrombocytopenia, and coagulopathy. Furthermore, it is oftentimes difficult or impossible to determine how long the PVT has been present. It is estimated that only 30% of the patients with chronic PVT receive anticoagulant therapy. 6 Despite these concerns, observational studies involving selected patients with chronic PVT who received anticoagulation have suggested a reduction in recurrent thrombosis and no clinically important increase in bleeding 9,43 and improved survival. 8,22,43 –45 The AASLD guidelines recommend that patients with chronic PVT who do not have cirrhosis and have a permanent thrombosis risk factor may be considered for long-term anticoagulation if there are no contraindications and appropriate treatment for esophageal varices has been undertaken. Reflecting the poor quality evidence supporting this recommendation, it is given a grade of recommendation of Grade IIa-C. 8 Overall, the potential benefits and harms of anticoagulation for chronic PVT should be based on an individual assessment of bleeding and thrombosis risks as well as the potential clinical consequence of bleeding and thrombosis.
How Safe Is Anticoagulation in Patients With Cirrhosis?
The development of PVT in patients with cirrhosis is important to recognize because of the associated development of portal hypertension and increased bleeding risk from esophageal varices. 46 –49 Early and effective treatment of PVT, therefore, may decrease the risk of variceal bleeding. 50 In patients with cirrhosis, the risk of bleeding is matched by risk of thrombosis and since the later is often silent, thrombosis is often missed and not treated. There is an increased tendency to bleed because of low platelet count and decreased production of most coagulation factors such as fibrinogen II, V, VII, IX, and X. 51 Paradoxically, there is also the possibility of a hypercoagulable state due to decreased levels of the anticoagulant proteins such as antithrombin, protein C, protein S, and heparin cofactor II and elevated levels of factor VIII and von Willebrand factor. 51,52 If anticoagulation is considered, it may be difficult to monitor VKA therapy in patients with advanced liver disease as the baseline INR is frequently prolonged. 53,54 Some recent studies have indicated that for acute PVT in patients with cirrhosis, anticoagulation with LMWH is largely safe and effective 55 –57 with recanalization rates of more than 35%, delay in the occurrence of hepatic decompensation, and improved survival. 58 However, there is frequent recurrence of thrombosis even after 12 months of therapy. 57,59 Although the current guidelines include anticoagulation for acute PVT in patients without cirrhosis, 8 there is no such recommendation for PVT in patients with cirrhosis. 59 Consequently, there may be reluctance to initiate anticoagulant therapy in such patients because of concerns that the risk of bleeding exceeds that of thrombus extension. Indeed, some authors have indicated that until the safety and efficacy of anticoagulation is established, such treatment should be avoided in patients with PVT and cirrhosis. 60 In general, patients with thrombophilia or intestinal ischemia should be considered for anticoagulation only after the risk of bleeding complications has been minimized such as with treatment of esophageal varices. 8,47
What Is the Role of Anticoagulation in Liver Transplant Associated PVT?
Complete or partial PVT is not uncommonly seen in patients waiting for liver transplant. Anticoagulation is considered in such patients to achieve recanalization and prevent extension of thrombus. However, very limited data are available on the outcome of such treatment. 8 There is no evidence that pretransplant PVT is an indication for long-term posttransplant thrombosis if adequate portal flow has been achieved by anastomosis and there is no prothrombotic disorder. 61
What is the duration of anticoagulant therapy for PVT?
The duration of anticoagulant therapy for PVT largely depends upon whether PVT is provoked, for example in association with surgery or intraabdominal sepsis, or unprovoked (idiopathic) and whether the provoking factor is correctable or not. Patients with provoked PVT should receive 3 months of anticoagulant therapy. 8,30 Some authors suggest that in case of partial recanalization after 3 months of treatment, anticoagulation should be continued until complete portal vein patency is attained. 62 On the other hand, if PVT appears unprovoked or is associated with a permanent risk factor such as a myeloproliferative disease and the risk of bleeding is estimated to be low, long-term anticoagulation may be justified. 30
What Is the Role of Thrombolysis and Thrombectomy?
The role of thrombolysis in the management of PVT is unclear. Several studies have assessed various thrombolytic agents (recombinant tissue plasminogen activator, urokinase, and streptokinase) and different routes of administration (intravenous, superior mesenteric artery catheterization, or the portal vein either transhepatic or transjugular) and have shown benefits in terms of thrombus resolution but with uncertain effects on clinical outcomes. 7,63 –66 The most common indication for such therapy in these studies was refractory symptoms or extensive disease with thrombus extension despite adequate anticoagulant treatment. 67 However, the studies may have selection bias as thrombolytic therapy was administered to patients only after anticoagulant treatment had failed. 2 This delay in initiating thrombolysis may also allow thrombus to become organized, thereby decreasing the potential for therapeutic benefit. Thrombolysis also confers high rates of bleeding (up to 60%) and may increase the mortality. 21,67 Given the low mortality of acute PVT, it is difficult to justify thrombolysis for the initial management of PVT and such treatment should be considered only when conventional anticoagulation has failed to improve symptoms or thrombus progression with worsening clinical signs and symptoms is present. 67
Thrombectomy, alone or in combination with thrombolysis, has the potential to achieve high rates of portal vein recanalization. However, this therapy (surgical or percutaneous transhepatic mechanical) is also associated with a high rate of complications, including morbidity, mortality, and recurrence of thrombosis. 4
Overall, use of thrombolytic therapy and thrombectomy is complicated by a high rate of serious complications; the net benefit:risk ratio does not favor their frequent use in the management of PVT. Further randomized-control studies are required to define their indications, efficacy, and safety.
What Is the Role of Shunt Procedures?
Shunt placement, either transjugular intrahepatic portosystemic (TIPS) or through conventional surgery, has a limited role in the management of PVT. The TIPS may be considered as an alternative to thrombolysis when anticoagulant therapy is ineffective to achieve the desired outcome or in the situations where PVT is associated with liver transplant. 68
The TIPS is an option in patients with PVT without cavernous transformation but if there is obstruction further down in the portal system, it may not have satisfactory outcome.
Conventional shunt surgery remains a last resort treatment option for PVT but appears to be effective only in the absence of superior mesenteric or splenic vein thrombosis. 69
What Is the Clinical Course of PVT and How Will This Affect the Patient Follow-Up?
The clinical course of treated PVT is variable and largely determined by the factors that include the extent of thrombosis, associated underlying diseases, and timeliness of anticoagulant therapy. 2,21,29,31,34,36,43 There are no good data on recurrence rate of PVT in patients with or without thrombophilic states. Patients with incomplete or no recanalization have a higher rate of complications, largely related to portal hypertension. After acute PVT, varices may develop in, as early as, 1 month. It is recommended that all such patients should be followed up closely as therapy for varices may reduce the risk of hemorrhage. 34 It is not known what percentage of patients with acute PVT will progress to chronic form. 2 All these potential outcomes should be considered during the follow-up of patients.
Summary
The PVT, once considered a rare disease, is being diagnosed with increasing frequency. The PVT is frequently found on abdominal imaging studies performed for other reasons. It is commonly associated with cirrhosis of liver, abdominal malignancy, local abdominal inflammation, or infections. It appears particularly frequent in patients with prothrombotic states, particularly the JAK2 mutation. Although coexistence of local and prothrombotic factor is not unusual, one should consider a hypercoagulable evaluation particularly in patients with idiopathic PVT. Acute PVT may be associated with immediate life-threatening complications of bowel ischemia leading to multiple organ failure and long-term complications of portal hypertension. Spontaneous resolution of PVT is uncommon. Conventional anticoagulants are the mainstay of treatment for acute PVT but their use in chronic PVT remains unclear. Thrombolysis and thrombectomy have a limited role and their use is associated with complications. Close follow-up of patient is important to identify the possible resolution of PVT, to determine the need for ongoing anticoagulation, and to monitor for possible disease and treatment-related complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.