
Abstract
Objective
We propose for the first time that D-dimer to creatinine ratio (DCR) may serve as a new clinical biomarker and explore its association with ST-segment elevation myocardial infarction (STEMI).
Methods
347 STEMI patients with complete D-dimer and creatinine were included in the analysis. According to the median of DCR value, patients were divided into the lower DCR group (DCR < 1.402, n = 173) and the higher DCR group (DCR ≥ 1.402, n = 174), and the differences between the two groups were compared. In addition, patients were divided into four groups according to the quartiles of Gensini score: Group 1(Gensini score ≤ 34, n = 88); Group 2(34 < Gensini score ≤ 65, n = 88); Group 3(65 < Gensini score ≤100, n = 87); Group 4(Gensini score >100, n = 84). Multivariate linear and multivariate logistic regression analyzes were performed to determine independent predictors of the Gensini score.
Results
High DCR group had higher Gensini score compared with the low DCR group (P < .05). DCR was positively correlated with Gensini score (r = 0.493, P < .001). Multiple linear regression analysis showed that Previous MI (r = 11.312, P = .035) and DCR (r = 5.129, P < .001) were independent risk factors associated with the Gensini score. Multivariate logistic regression analysis showed that, compared to Group 1, DCR was an independent risk factor in Group 2, Group 3, Group 4 (P < .001).
Conclusions
As a new and useful clinical biomarker, DCR was positively correlated with coronary Gensini score in STEMI patients.
Introduction
Acute ST-segment elevation myocardial infarction (STEMI) is one of the critical conditions endangering human health worldwide, with rapid onset and high mortality. 1 The most common cause is complete occlusion of the epicardial coronary artery by intracoronary thrombosis. Reperfusion therapy, including thrombolytic therapy, percutaneous coronary intervention (PCI), or coronary artery bypass surgery must be performed as early as possible.2–4 Activation of coagulation and fibrinolysis systems play a crucial role in the pathogenesis and prognosis of STEMI. 5 As a product of fibrinoid degradation, D-dimer increases in thrombosis and/or dissolution in the circulatory system and can be used clinically as a clinical biomarker of thrombosis.6,7 Increased D-dimer levels have also been found to be associated with the severity of coronary artery disease in patients with STEMI. 8 At the same time, serum creatinine level, as one of the indicators reflecting renal function, is associated with systemic atherosclerosis.9,10 In addition, studies have found that creatinine levels are correlated with the occurrence, severity, and prognosis of coronary artery disease.11–13
Previous studies have combined serum creatinine with other clinical indicators to assess risk and prognosis in cardiovascular disease(CVD) patients. For example, the urea to creatinine ratio (UCR) was shown to be one of the predictors of long-term mortality in chronic heart failure with preserved ejection fraction patients. 14 In addition, UCR has also been found to have predictive value for the prognosis of patients with acute myocardial infarction complicated with acute heart failure. 15 The American College of Cardiology/American Heart Association recommends the use of cardiovascular biobiomarkers for rapid diagnosis and prognostic assessment of patients with chest pain. 4 Although much attention has been paid to D-dimer and creatinine studies respectively and it has been found that both may provide additional information for diagnosis and risk assessment in patients with CVD. However, there is no research that combines these two easily available indicators. Therefore, we conducted this study to combine D-dimer and creatinine(DCR) as new clinical biomarker and examine the correlation between the DCR and Gensini score in patients with STEMI.
Materials and Methods
Study Population
The main data used in this study was obtained from Dryad Digital Repository. The data can be accessed in the Dryad Digital Repository (10.5061/dryad.pf56 m). 16 From January 2010 to October 2014, 464 STEMI patients from a single center participated in the study. Finally, 347 patients with complete D-dimer and creatinine results were included in this analysis. This is a prospective observational study, which has previously reported the full details of the study population. Written consent was signed by all enrolled patients. The protocol of the study was approved by the ethics committee of Taizhou First people's Hospital. The diagnostic criteria for STEMI are as follows: (1) chest pain that persisted for more than 30 minutes; (2) prolonged ischemic ST-segment elevation and/or depression that included two or more contiguous leads; (3) significant increases in creatine kinase-myocardial band (CK-MB) and cardiac troponin concentrations in laboratory findings. 17 Exclusion criteria included: (1) cardiogenic shock; (2) severe vascular heart disease; (3) history of ventricular fibrillation; (4) secondary hypertension; (5) untreated third-degree or late atrioventricular block; (6) cerebrovascular disease; (7) life expectancy <12 months; (8) recent severe infection; (9) recent major surgery or trauma (within 6 months); (10) active bleeding; (11) endocrine disorders such as thyroid dysfunction, adrenocortical dysfunction; (12) severe renal insufficiency requiring dialysis; (13) history of chronic hepatitis or cirrhosis; (14) Non-STEMI patients; (15) Incomplete clinical data.
Clinical and Demographic Characteristics Collection
The following demographic and clinical data of all patients were collected: gender, age, hypertension, diabetes mellitus, and history of myocardial infarction (MI). The following biochemical indicators were tested according to local laboratory standards 16 : fasting blood glucose (FBG), percentage of neutrophils, white blood cell count, hemoglobin, platelets, blood urea nitrogen (BUN), creatinine, uric acid, total cholesterol (TC), triglyceride (TG), High-density lipoprotein (HDL-C), low-density lipoprotein-cholesterol (LDL-C), CK-MB, cardiac troponin I (cTnI), D-dimer. Calculate the DCR based on the D-dimer and creatinine values: DCR = D-dimer*100/creatinine. All patients entered the emergency room within 12 hours of onset, and all received a loading dose of oral aspirin (300 mg), clopidogrel (300 mg), as well as intravenous heparin (initially 10,000 IU, added during surgery). The interventional surgeon determines and records the location of the patient's myocardial infarction based on the angiographic results, and which of the left circumflex coronary artery (LCX), left anterior descending coronary artery (LAD), and right coronary artery (RCA) is the culprit vessel. Two-dimensional echocardiography and Doppler parameters were measured using biplane Simpson's method to obtain left ventricular end-diastolic diameter (LVEDD) and left atrial diameter (LAD).
The Gensini score was calculated by two independent senior cardiologists as previously described: 1 point for ≤ 25% obstruction, 2 points for 26–50% obstruction, 4 points for 51–75% obstruction, 8 points for 76–90% obstruction, 16 points for 91–99% obstruction, and 32 points for total occlusion(100%). Then the score is multiplied by the factor which depends on the functional significance of the area supplied by that segment(5 for the left main coronary artery, 2.5 for the proximal segment of left anterior descending artery or circumflex artery, 1.5 for the middle segment of left anterior descending artery, 1 for the apical segment of left anterior descending artery or the middle or distal segment of circumflex artery or the entire segment of the right coronary artery, and 0.5 for other small branches of the coronary artery).18,19
Statistical Analyzes
Data were analyzed using Statistics v26.0 (SPSS Inc., Chicago, IL, USA), the statistical software packages R (The R Foundation; http://www.r-project.org; version 3.6.2), and MedCalc v19.5.6 (MedCalc Software bvba, Ostend, Belgium). The normal distribution of continuous variables was tested using the Shapiro–Wilk test. Continuous variables with normal distribution were expressed as mean ± standard deviation (Mean ± SD) and were analyzed by Student's t-test. The non-normal distribution data were presented as medians (25th and 75th percentiles) and compared by the Mann-Whitney U test. Categorical variables are shown as counts and percentages and analyzed by Pearson's chi-square test. The Spearman correlation analysis (r) was used to determine whether there was a significant correlation between variables. We employed both multivariate linear regression analysis and multivariate logistic regression analysis, analyzing the Gensini score as a continuous and a categorical variable, respectively. For all statistical analyzes, statistical significance was defined as a two-sided P-value less than or equal to .05.
Results
Comparison of Clinical Characteristics Between Different DCR Level Groups
Of the 464 STEMI patients, 347 with complete records of serum D-dimer and creatinine levels were finally included and analyzed (264 males and 83 females), with an average age of 63.22 ± 12.73 years. All patients were divided into two groups according to the median of DCR value(1.402): the lower DCR group (DCR < 1.402, n = 173) and the higher DCR group (DCR ≥ 1.402, n = 174). There were no significant differences in age, gender, history of diabetes, history of hypertension, previous MI, Killip class I, heart rate, anterior wall MI between the two groups (all P > .05). Compared with the low DCR group, the high DCR group had higher SBP, FBG, D-dimer, LVEDD, and Gensini score (all P < .05). The serum creatinine level was higher in the low DCR group than in the high DCR group (P < .05). In addition, there were no significant differences in neutrophil percentage, white blood cells count, urea nitrogen, uric acid, hemoglobin, platelet, albumin, TC, TG, HDL-C, LDL-C, cTnI, CK-MB, LAD, culprit vessel, pathological Q-wave between the two groups (all P > .05) (Table 1).
Comparison of Clinical Characteristics Between Different DCR level Groups.

Data are expressed as mean ± SD or median (25th, 75th percentile) for continuous variables and n (%) for categorical variables.
Abbreviations: BUN, blood urea nitrogen; CK-MB, creatine kinase-MB; cTnI, cardiac troponin I; DCR, D-Dimer to creatinine ratio; FBG, fasting blood glucose; HDL-C, high-density lipoprotein; LAD, left atrial diameter; LCX, left circumflex coronary artery; LDL-C, low-density lipoprotein-cholesterol; ECG, endocardiogram; LVEDD, left ventricular and diastolic diameter; MI, myocardial infarction; RCA, right coronary artery; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride; WBC, white blood cells.
P-value <.05 was considered statistically significant
Correlation Analysis
Spearman correlation analysis showed that DCR was positively correlated with Gensini score (r = 0.493, P < .001) (Figure 1). Then, according to the quartile method, we divided the patients' scores into four groups based on the Gensini score: Gensini score ≤ 34 (Group 1, n = 88); 34 < Gensini score ≤ 65 (Group 2, n = 88); 65 < Gensini score ≤ 100 (Group 3, n = 87); Gensini score > 100 (Group 4, n = 84). In the Group 2, the Spearman correlation coefficient of DCR and Gensini score was the highest (r = 0.381, P < .001).

Scatter diagram of DCR and Gensini score
Multivariate Regression Analysis
A multiple linear regression model was used to examine the relationship between Gensini score and DCR or other possible cardiovascular risk factors. Variables of gender, age, history of diabetes, history of hypertension, previous MI, FBG, urea nitrogen, percentage of neutrophils, white blood cells count, uric acid, hemoglobin, platelet, albumin, DCR, TC, TG, HDL-C, LDL-C, cTnI, CK-MB were included in the model (D-dimer and creatinine were not included in the model due to the presence of collinearity).The results showed that Previous MI (r = 11.312, P = .035) and DCR (r = 5.129, P < .001) were independent risk factors associated with Gensini score (Table 2).
Multivariate linear Regression Analysis for Gensini Score as a Continuous Variable.

Abbreviations: BUN, blood urea nitrogen; DCR, D-Dimer to creatinine ratio; FBG, fasting blood glucose; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein-cholesterol; MI, myocardial infarction; TC, total cholesterol; TG, triglyceride; WBC, white blood cells.
P-value <.05 was considered statistically significant.
In the multivariate logistic regression analysis, we used the Group 1(Gensini score ≤ 34) as references. Hypertension (OR: 2.148, 95%CI: 1.071-4.307, P = .031) and DCR (OR: 2.819, 95%CI: 1.989-3.994, P < .001) were independent risk factors for the Gensini score in Group 2 (34 < Gensini score ≤ 65). DCR (OR: 2.977, 95%CI: 2.102-4.215, P < .001) was an independent risk factor for the Gensini score in Group 3 (65 < Gensini score ≤ 100). In addition, Previous MI (OR: 3.581, 95%CI: 1.123-11.417, P = .031), DCR (OR: 3.078, 95%CI: 2.172-4.361, P < .001) and FBG (OR: 1.167, 95%CI: 1.011-1.347, P = .035) were independent risk factors for the Gensini score in Group 4 (Gensini score > 100)(Table 3).
Multivariate logistic Regression Analysis for the Gensini Score as a Hierarchical Variable.

Abbreviations: DCR, D-Dimer to creatinine ratio; FBG, fasting blood glucose; MI, myocardial infarction.
P-value <.05 was considered statistically significant.
ROC Analysis
A receiver operating characteristic (ROC) curve analysis was performed and showed that DCR predicted a higher Gensini score (Gensini score>34)with a sensitivity of 69.11% and a specificity of 85.23% (area under ROC curve = 0.821, P < –.001), a cut-off value of 1.11, and a Youden index of 0.543(Figure 2).
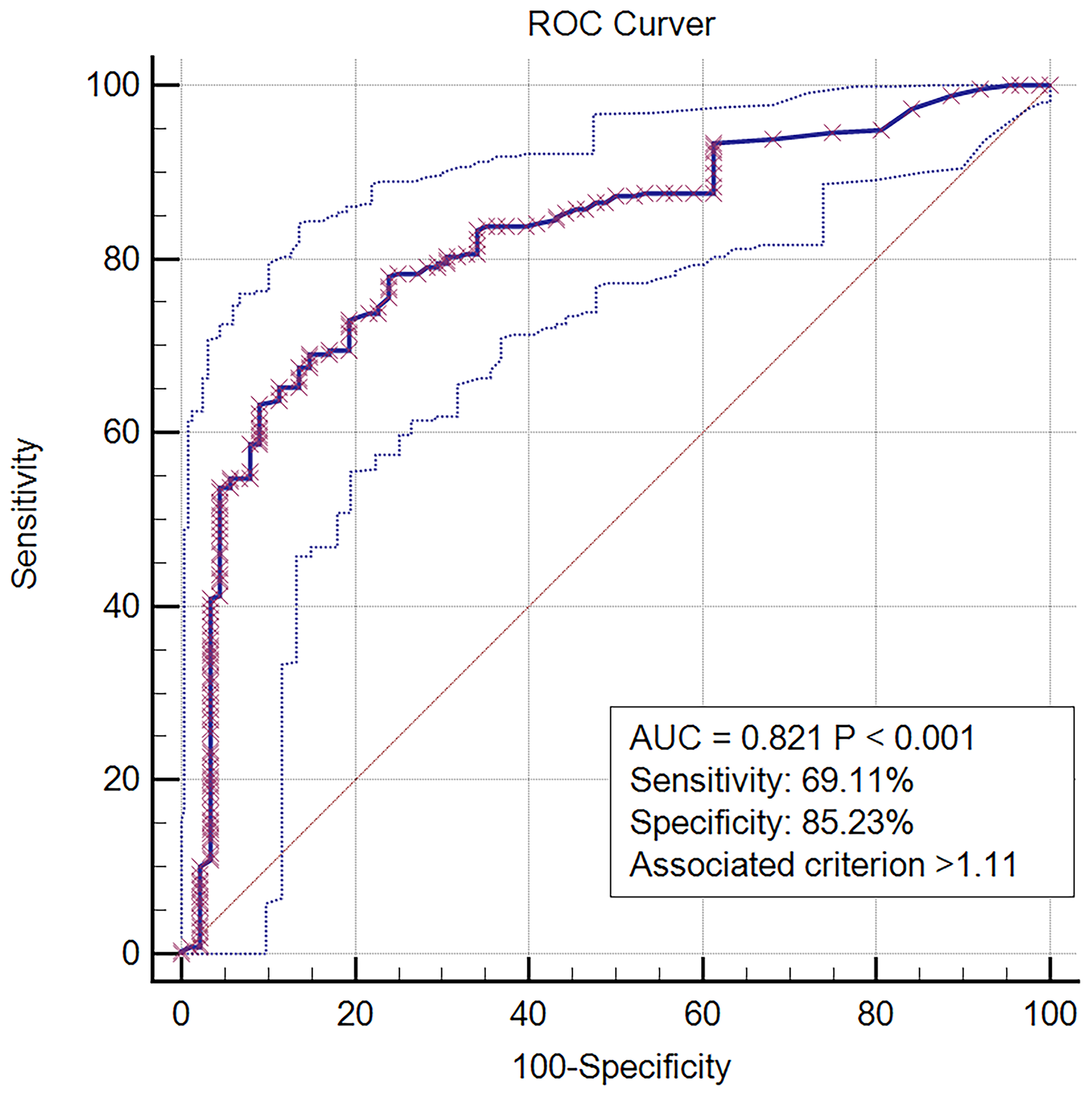
Receiver operating characteristic curve of DCR for predicting a higher Gensini score.
Discussion
In this study, we first proposed DCR as a new clinical biomarker. And to our knowledge, this is the first time that DCR has been identified as a new useful biomarker. Our results suggest that DCR is correlated with coronary Gensini score in STEMI patients, and DCR can be an independent predictor of a higher Gensini score. The Gensini score has been widely used as an indicator of severity of coronary artery stenosis, 20 so an elevated DCR predicts a more severe coronary artery stenosis. In addition, measuring and calculating DCR in STEMI patients may has reference value for rapid assessment of patients presenting at the initial referral hospital, guiding recommended treatment, and transfer to STEMI receiving hospital.
Acute myocardial infarction is the most important cause of cardiovascular death. Thrombosis and coronary occlusion following the rule of a plaque is the main pathological basis of STEMI. 21 Rupture or erosion of the lipid-rich necrotic core activates unstable platelet aggregation, which is accelerated by the formation of fibrin, with red blood cells and inflammatory cells massively clustering in the fibrous reticular structure to form the thrombus. Ultimately, one or more branches of the coronary artery are interrupted and distal embolization occurs. 22 D-dimer can be used as a biomarker of fibrinolysis, which is the most important laboratory indicator reflecting thrombosis and thrombolytic activity.23,24 In the final stage of coagulation, fibrinogen is excised into A and B peptides under the action of thrombin and transformed into fibrin monomers. With the increase of the concentration of fibrin monomers, these monomers polymerize with each other to form polymers. Soluble fibrin polymer acts as a cofactor, acting together with thrombin to activate coagulation factor XIII. Activated factor XIII promotes cross-linking between the r chains of adjacent fibrin molecules to form stable fibrin aggregates. There is a mechanism of fibrinolysis with coagulation. At the same time of thrombosis, some anti-fibrinolytic substances will be produced, which will degrade the fibrin polymer to form the end products including E fragment and D fragment. D-dimer is a polymer of D-D fragments of fibrin molecules crosslinked together formed by fibrin polymers under the action of plasmin enzymatic hydrolysis.25–27 Study have found that D-dimer is associated with in-hospital adverse outcomes, ischemic and hemorrhagic events after acute myocardial infarction.28,29 It has also been suggested that D-dimer may be an independent predictor of 2-year mortality after percutaneous coronary intervention in patients with coronary artery disease. 30 D-dimer has also been shown to correlate with coronary SYNTAX II score and Gensini score in patients with coronary heart disease.8,31 Creatinine is a metabolite of creatine, which is released during dephosphorylation to form creatinine and is excreted in the form of urine. Most of it is filtered from the glomerulus and is not reabsorbed by the renal tubules, with little excretion.32,33 In different calculation methods of glomerular filtration rate, creatinine has always been one of the important inclusion indicators. Results based on a prospective community-based atherosclerosis risk in communities study showed that people with high serum creatinine levels had an increased risk of coronary heart disease. 34 Serum creatinine levels have been shown to be an independent predictor of the severity and short-term outcome in patients with coronary artery disease.31,35,36
Given the above previous findings, both D-dimer and creatinine are associated with the occurrence of coronary heart disease, especially the severity of coronary artery disease. We explored for the first time the relationship between DCR and the severity of coronary artery lesions in STEMI patients. Our results indicate that there is a positive correlation between DCR and Gensini score of coronary artery in STEMI patients, and DCR is one of the independent predictors of Gensini score and can also be used as an independent predictor of Gensini high score. This result is reasonable and the possible mechanisms are listed as follows: (1) high D-dimer levels reflect a systemic pre-thrombotic state and focal vessel wall-associated fibrinogenesis with unstable atherosclerotic plaque activity; 37 (2) thrombotic activity and thrombus burden are important factors in the magnitude of the increase in D-dimer levels, which are positively correlated with the burden of “fresh” thrombus; 38 (3) Creatinine levels can reflect renal function and be used to calculate estimated glomerular filtration rate (eGFR), and reduced eGFR leads to hypertensive state, oxidative stress, abnormal calcium, and phosphorus metabolism, anemia and other factors, further aggravating vascular endothelial damage, thus accelerating the formation and progression of coronary atherosclerotic plaques.39,40
There are still some limitations in this study. Firstly, as a single-center study, we could not determine the causal relationship between DCR and Gensini score because laboratory findings were measured only once in the design of the study. Secondly, only patients with STEMI were enrolled in this study. Therefore, the results may not apply to the general population. In the future, prospective multicenter studies with larger sample sizes that include different types of coronary artery disease are needed to further evaluate the correlation between DCR and Gensini score. Thirdly, the original data we obtained were not detailed, such as the medication information of patients was not provided. Thus although adjustments have been made, unknown confounding factors may affect the results. Therefore, the interpretation of the results should be careful. Finally, we did not further evaluate the relationship between DCR and the prognosis of STEMI patients, and relevant studies can be designed in the future to explore whether it has potential value.
Conclusions
Our study is the first time to propose DCR as a new clinical biomarker and demonstrate its correlation with coronary Gensini score in STEMI patients. This new biomarker is useful for early evaluation of in patients with STEMI, especially in medical institutions that do not have the ability to perform emergency coronary angiography. DCR can also guide further treatment strategy choices, including relevant medical devices and physician preparation.
Footnotes
Acknowledgements
The authors thank Lingchang Yang, Ting Zheng, Haopeng Wu, Wenwei Xin, Xiongneng Mou, Hui Lin, Yide Chen, Xiaoyu Wu, and the research investigators for sharing their data.
Author Contributions
YiZ: conceptualization and writing-original draught. YL, YiZ, JY and ZBL: data curation.YiZ,YL,and JMT: supervision.YinZ and YL: validation.YL and JY: writing-review and editing.All authors contributed to the articleand approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.