
Abstract
Objectives:
The underutilization of manual thrombus aspiration (MTA) may have reduced the benefits of ischemic postconditioning (PostCon), as it reduces thrombus embolization. We aimed to assess the benefits of PostCon in patients with ST-segment elevation myocardial infarction (STEMI) after the systematic utilization of MTA.
Methods:
A total of 87 patients were enrolled in a prospective, randomized trial (43 PostCon and 44 controls). After MTA, PostCon was performed on the treatment group by applying 4 cycles of alternate reperfusion and reocclusion (60 seconds each) using the angioplasty balloon. The primary end point was infarct size assessed by the area under the curve (AUC) of troponin T (TnT) activity. The secondary end points were left ventricle ejection fraction (LVEF) and major cardiac events (new myocardial infarction or cardiac death) both at discharge and at follow-up.
Results:
The AUC for TnT was no different with respect to study arms (median [interquartile range]): PostCon = 8.9 (10.6) versus control = 8.2 (10.6), P = .68. Left ventricle ejection fraction improved from in-hospital to follow-up (9 ± 3 months) for the entire cohort (46.3% ± 7.3% vs 52.2% ± 10.7%, P < .001), with no differences between PostCon and controls (51.6% ± 9.5% vs 52.7% ± 11.9%, P = .89); major cardiac events at 14 ± 4 months of follow-up were also no different (PostCon = 1.0 (2.3%) vs control = 0, P = .49).
Conclusion:
In patients with STEMI treated with MTA, PostCon offered no benefits to infarct size, LVEF, or major cardiac events.
Introduction
Timely restoration of coronary blood flow by means of primary percutaneous intervention (PCI) is the recommended strategy to treat ST-segment elevation myocardial infarction (STEMI). 1 Despite significant advances in mechanical reperfusion treatment, high rates of mortality and morbidity are still observed. 2,3 This may partially be ascribed to the reperfusion lesion. The concept that reperfusion itself could lead to myocardial injury captivated the attention of many investigators. 4,5 It is estimated that the reperfusion injury (RI) phenomenon may represent as much as half of the final infarct size. 6 Therefore, extensive research on treatments that could minimize the RI phenomenon has been pursued.
Ischemic postconditioning (PostCon) was first described by Zhao et al. 7 In a dog model, they found that intermittent occlusion of the coronary artery immediately after achieving reperfusion led to the same amount of myocardial salvage when compared to preconditioning. While promising results were achieved in some human trials, 8 –12 most of them failed to confirm the benefits of PostCon when compared to standard PCI. 13 –19 A recent meta-analysis 20 showed that PostCon did not reduce infarct size as assessed by cardiac resonance imaging (CMR). The interpretation of these conclusions should be cautious, given the significant heterogeneity across trials.
In recent trials testing PostCon, thrombus aspiration was limited (none to 30% of cases). 8 –19 Manual thrombus aspiration (MTA) as an adjunct to reperfusion has been shown to reduce microvascular obstruction and infarct size as evaluated by CMR, 21 to preserve microvascular integrity 22 and to improve clinical outcomes, 23,24 and it has been included in the current STEMI guidelines 1 as a class IIa/B recommendation. However, a large recent trial showed that routine thrombus aspiration before PCI failed to reduce 1-year adverse clinical events in comparison with PCI alone, 25 shadowing the putative benefits of this empirical and easy-to-use technique. Its utilization either routinely or selectively in the United States ranges from 20% to 90% of all primary PCIs, 26,27 reflecting procedural variations in the interventional community. In our center, thrombectomy was used in more than 70% of cases over the last 6 years. 28 Nevertheless, coronary microembolization may offset cardioprotective measures, 29 and it is plausible that balloon angioplasty not preceded by thrombectomy may promote distal thrombus embolization and microvascular dysfunction, blunting the effects of PostCon.
Our aim was to study the effect of PostCon on myocardial infarct size in patients with STEMI treated with primary PCI after systematic utilization of MTA. The secondary end points were left ventricle ejection fraction (LVEF), both at discharge and at follow-up, and major adverse cardiac events.
Methods
This was a prospective, single-center, randomized, controlled, open clinical trial. It was performed in accordance with the Declaration of Helsinki and the European Guidelines for Good Clinical Practice and was approved by the Ethics Committee of Porto Hospital Centre (223/11-139-DEFI/209-CES). All patients gave written informed consent.
Study Population and Definitions
Patients with STEMI older than 18 years of age and within 12 hours from onset of symptoms, admitted to our center for primary PCI, were eligible for enrollment provided they fulfilled the following inclusion criteria: ST-segment elevation ≥0.1 mV (≥0.2 mV at V1 and V3) in 2 contiguous electrocardiogram (ECG) leads or new left bundle branch block and a thrombolysis in myocardial infarction (TIMI) 0 flow in the infarct-related artery without significant collaterals (Rentrop grade 0 or 1). Patients with bypass grafts, severe renal impairment (creatinine clearance by Cockcroft-Gault formula <30 mL/min/1.73 m2), previous myocardial infarction on culprit vessel, Killip-Kimball class on presentation ≥3, life expectancy <12 months, culprit vessel diameter <2.5 mm, lesion deemed not suitable for MTA or stent implantation, infarction due to left main coronary artery occlusion, and refusal or impossibility to give informed consent were excluded. Total ischemic time, door-to-balloon, and ECG-to-balloon times were determined as the periods elapsed from the onset of chest pain, hospital admittance, and diagnostic ECG, respectively, to the passage of the coronary occlusion with the first device (aspiration catheter or angioplasty balloon/stent). For each patient, the TIMI risk score for STEMI 30 and the SYNTAX 31 score were calculated. The SYNTAX score version 2.11 was calculated by scoring all coronary lesions with a diameter stenosis >50% in vessels >1.5 mm by 2 senior interventional cardiologists. The infarct-related artery with TIMI 0 flow was scored as an occlusion <3 months duration.
Study Design and Protocol
Patients were loaded with 300 mg aspirin and 600 mg clopidogrel before PCI. The 6F catheterization was performed by radial or femoral approach. Following angiogram acquisition, unfractionated heparin 70 IU/kg was administered on a peripheral vein and 3 mg nitroglycerin was given intracoronarily. Patients were then randomized 1:1 to either the PostCon protocol or the standard (control) PCI after opening a sealed opaque envelope. The block randomization sequence was computer generated by an investigator not involved in patient care (RM). The sealed envelopes were transferred to the catheterization laboratory and were consecutively numbered. Manual thrombus aspiration was exclusively performed by a 6F Export device (Medtronic, Minneapolis, Minnesota). If reflow (TIMI ≥ 2) was restored after guidewire passage or the aspiration device was unable to reach the lesion, the patient was excluded. After MTA, patients allocated to the PostCon arm underwent 4 cycles of 60 seconds reperfusion followed by 60 seconds reocclusion at low pressure (6 atm), with either the angioplasty balloon (in case the lesion was predilated) or the balloon stent (in case of direct stenting), whichever came first. Aspiration was considered effective if TIMI 2 to 3 flow was achieved on the target vessel provided the occlusion was crossed by the device. The PostCon sequence had to commence within 5 minutes after reflow if the aspiration was effective. Where MTA was ineffective, the PostCon sequence started with the angioplasty balloon. The type of stent, adjunct medication, or devices were left to the operator’s discretion. After PCI, patients were admitted to the cardiac care unit where evidence-based medications were administered accordingly. Blood samples were collected on hospital admittance and at 6, 12, 24, 48, and 72 hours after PCI. On discharge from the hospital, patients were instructed to take aspirin indefinitely and clopidogrel for at least 1 year.
Area at Risk, Infarct Size, and Left Ventricle Function
The area at risk (AAR) was estimated by angiography using the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease Score (APPROACH score). In brief, this score estimates the percentage of the myocardium that is perfused by each segment of the 3 major epicardial vessels, in accordance to the anatomical dominance and size of side branches. It is well correlated with the AAR as estimated by CMR. 32,33 The infarct size was estimated by the area under the curve (AUC, arbitrary units) for troponin T (TnT) activity in plasma. Troponin T was measured on a third-generation Elecsys Modular Analytics e170 (Roche Diagnostics, Mannheim, Germany). Left ventricle ejection fraction was determined by 2-dimensional echocardiography (Phillips iE33, Eindhoven, the Netherlands), using the biplane Simpson method on all patients prior to hospital discharge and on scheduled follow-up visits. The LVEF was calculated, by consensus, by 2 senior echocardiographers blinded to the study arm.
Major Cardiac Events and Follow-Up
All participating patients were monitored in the outpatient clinic. Major cardiac events were considered to be death from cardiac causes or recurrent myocardial infarction (MI). By default, death was presumed to be of cardiac origin unless another cause was identified. MI was defined as a new (with or without Q-wave) infarction as described elsewhere. 34
Statistical Analyses
Based on previous trials and in basic research, 6,20,35 a 20% reduction in infarct size in patients submitted to PostCon was anticipated. A sample comprising 66 patients was considered necessary (power = 80%, α = .05 in a 2-tailed test). To compensate for missing samples and patient dropout, we decided to enroll 90 patients. Continuous normally distributed data are expressed by mean ± standard deviation (SD) and compared using Student’s t test, while nonnormally distributed data are expressed by medians and interquartile range (IQR) and compared using Mann-Whitney U test. Categorical variables are expressed by percentages and compared using chi-square or Fisher exact tests. The AUC for TnT was calculated by the trapezoidal rule and was Log(10) transformed to enable parametric tests. Linear regression was generated to compare the AUC for both study groups in accordance with the AAR. Left ventricle ejection fraction was compared between study groups both in-hospital and at follow-up by repeated measures analysis of variance. All tests were 2-sided, and P < .05 was considered significant. Analysis was performed using the perprotocol principle and all data were analyzed using SPSS v.20 (SPSS, Chicago, Illinois).
Results
Patient enrollment occurred between March 2012 and April 2014. During this period, 321 patients with STEMI were admitted to primary PCI (Figure 1). One hundred patients met the inclusion criteria and entered randomization. The MTA was not performed in 11 cases and the patients were excluded after randomization: 3 of these (2 PostCon and 1 control) were due to excessive coronary tortuosity not amenable for the aspiration catheter to cross the lesion, and in the remaining cases, reflow was achieved after crossing the occlusion with the coronary guidewire. One patient in the PostCon group was excluded due to technical difficulties in performing the PostCon sequence within the 5-minute frame, and 1 patient was excluded from the control group due to the absence of a significant coronary lesion after MTA. Therefore, 43 patients in the PostCon group and 44 in the control group entered final analysis. Both groups were well balanced on clinical (Table 1) and procedural (Table 2) characteristics, except for the radial approach which was used less often in the PostCon group, and a trend toward more postdilation in the control group. Overall, most of the patients were reperfused within 4 hours from symptoms onset. The majority had single-vessel disease, and the culprit vessel in almost half of the patients in both groups was the left anterior descending artery. The MTA was considered effective in 41 (95.3%) patients in the PostCon group and in 39 (88.6%) in the control group (P = .43). The time elapsed from removing the aspiration device to first inflation of the balloon/stent was 1.5 ± 0.5 minutes for PostCon and 1.6 ± 0.6 minutes for controls (P = .52).
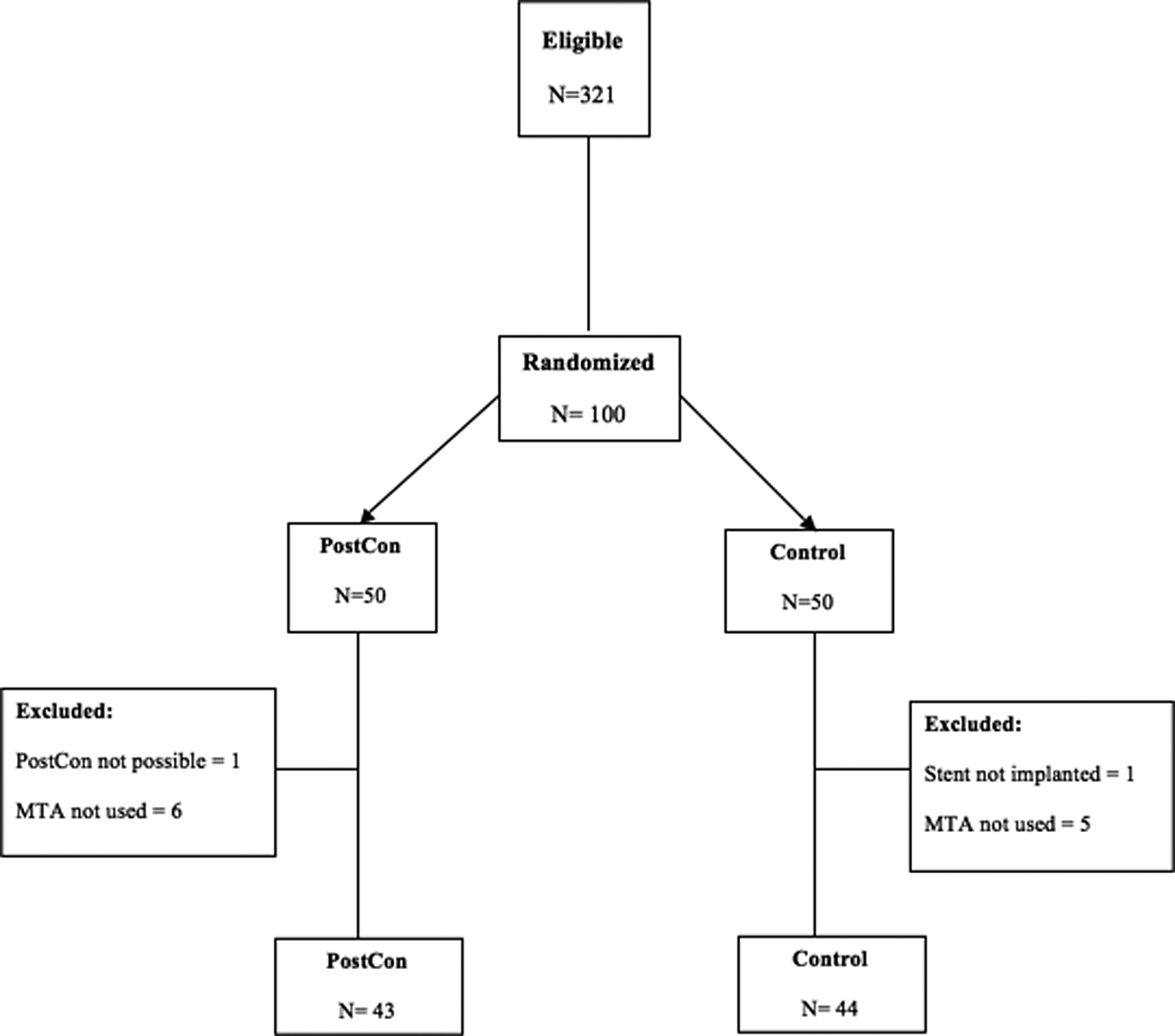
Patient flowchart. PostCon indicates postconditioning; MTA, manual thrombus aspiration.
Baseline Features of Studied Patients.

Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; SD, standard deviation; IQR, interquartile range; TIMI, thrombolysis in myocardial infarction; PostCon, postconditioning.
Procedural and Angiographic Characteristics.

Abbreviations: ECG, electrocardiogram; IQR, interquartile range; PostCon, postconditioning.
Infarct Size
For the entire cohort, 6 (1.1%) blood samples were lost. Because all missing samples were from the descending arm of the curve, missing values were calculated as the average of the 2 flanking samples. The AUC for TnT was not significantly different between study groups (median AUC = 8.9 [IQR = 10.6] for PostCon vs 8.2 [IQR = 10.6] for the control group, P = .68; Figure 2). Additionally, the regression line to fit the infarct size with respect to the AAR failed to show differences between study arms (P for interaction = .35; Figure 3).

Mean troponin-T (TnT) activity and 95% confidence intervals from before (TnT0h) to 72 hours after intervention. PostCon indicates postconditioning.

Infarct size measured by the area under curve of troponin-T (AUC TnT) activity vs area at risk (AAR) assessed by the angiographic APPROACH score. The regression lines for both groups don’t differ significantly (P = .35).
Left Ventricular Ejection Fraction and Cardiac Events
In-hospital echocardiography was performed on all patients after PCI (4 ± 3 days), LVEF was no different for PostCon versus control (47.1% ± 7.7% vs 45.9% ± 7.1%, P = .46). Seventy-three (84%) patients underwent follow-up echocardiographic evaluation (9 ± 3 months). Left ventricle ejection fraction had significantly improved at follow-up for the entire cohort (46.3% ± 7.3% vs 52.2% ± 10.7%, P < .001), with no differences between PostCon and control groups (51.6% ± 9.5 vs 52.7% ± 11.9, respectively, P = .89; Figure 4).

Mean ejection fraction (EF%) and 95% confidence interval for both groups in-hospital and at follow-up.
No cardiac-related deaths occurred, either in hospital or at follow-up (14 ± 4.3 months). Only 1 (1.1%) cardiac event occurred: 1 patient in the PostCon group had subacute stent thrombosis (MI) and repeated PCI successfully. Two patients died from noncardiovascular causes, one due to purulent mediastinitis and the other had multiorgan failure after complicated pneumonia. At follow-up, there were no differences in the ongoing medications between PostCon and controls groups; all patients were on a statin and the majority was on beta-blockers (35 [83%] vs 41 [92%], P = .19) and angiotensin-converting enzyme inhibitors (26 [62%] vs 26 [59%], P = .79).
Discussion
The present study demonstrates that PostCon failed to reduce infarct size when compared to standard PCI after the routine utilization of MTA. Additionally, no differences were found in major cardiac events or in LVEF both in-hospital and at follow-up.
The translation of PostCon experimental results into the clinical practice may be hampered by several factors. 36 –38 In contrast to animal experiments, patients may have large plaque and thrombus burden and are likely to have diffuse distal coronary disease, which could lead to microvascular occlusion and therefore blunt the effects of local PostCon. 29 Our study explored this important issue by requiring routine utilization of MTA in enrolled patients. We hypothesized that MTA would reduce thrombus burden, which would prevent distal embolization and therefore enhance the putative benefits of PostCon. Furthermore, a time window of no longer than 5 minutes after MTA to initiate PostCon protocol was mandatory, to limit RI dependent on abrupt reflow. Although initial animal studies showed that cardioprotection is lost if the PostCon maneuver was applied several minutes after resumption of flow, 7,39 others had questioned that by providing evidence that cardioprotection exists even if PostCon was performed after a prolonged period of reperfusion (delayed conditioning). 40 Unfortunately, this was not confirmed in a clinical study that showed no impact of PostCon in patients already with TIMI 2 to 3 flow on admission. 41 Therefore, a “second window” of opportunity could not be anticipated and thus PostCon had to be performed as soon as possible after reflow was achieved. The time elapsed from the retrieval of the thrombectomy device, and the first inflation of the balloon/stent was short, averaging 1.6 minutes in the PostCon group which is the time needed to open the package with the balloon or stent and to assemble it on the guidewire. Nevertheless, it might be long enough for the mitochondrial permeability transition pore to open and trigger cell death, as the effective window for the first reperfusion period in humans is unknown.
Common risk factors as well as ongoing and periprocedural medication may condition the heart to a level at which PostCon becomes redundant. 38,42 One elegant study from Yang et al 43 found that clopidogrel (and cangrelor) may act as conditioning mimetics acting in the same signaling pathways as PostCon. The benefits of these agents during reperfusion may well be larger than that provided by their antiplatelet properties. One may speculate that in later PostCon trials, all patients who were loaded with clopidogrel may have already been conditioned to a level rendering PostCon futile. 44 However, clopidogrel is slow to be converted into the active drug, and conditioning is related to its capability to block platelet aggregation. Therefore, the time from the loading dose to PCI may impact the effects of cardioprotective maneuvers that take place at reperfusion. Our patients were loaded either upon hospital admission or in the ambulance, never in the catheterization laboratory. It is therefore conceivable that some degree of conditioning may have been provided by clopidogrel.
Nitroglycerine administration is routinely used in many catheterization laboratories during PCI. Nitric oxide donors like exogenous nitroglycerine induced early and late preconditioning in rabbits. 45 In our study, patients on nitrates were infrequent and balanced between groups; therefore, the presumed preconditioning effect of these drugs was neither a confounding factor nor a competitor to PostCon in the conditioning action.
Another drug used in PCI that can interfere with the reperfusion lesion are opioids. One small trial involving a remifentanil infusion given to patients undergoing bypass surgery reduced troponin I release, 12 hours postoperatively. 46 The potential for short-acting opioids such as remifentanil to exert PostCon during reperfusion was also studied. In the animal model, remifentanil appeared to have properties similar to PostCon by acting on both κ and δ receptors, which are thought to trigger PostCon. 47 Another study showed that the protective effect provided by remote ischemic periconditioning is enhanced by morphine if given to patients before reperfusion. 48 In our series, the opioids that were used to manage pain were fentanyl and morphine. In summary, patients enrolled in trials testing PostCon during reperfusion may have been exposed to pharmacological agents that may have already activated cardioprotective pathways. This factor is obviously not accounted for in the experimental settings.
One could always argue many trials published so far were relatively small because the estimated reduction in infarct size of around 20% in the PostCon groups was too optimistic. However, one medium-size 18 trial with infarct size evaluated by CMR and clinical end points and one large 17 trial that evaluated ST-segment resolution and clinical end points failed to disclose the benefits of PostCon. Another explanation comes from the kind of patients enrolled. Similar to previous trials, we only included low-risk patients with STEMI. We speculate that in STEMI’s involving large areas at risk 13 or in patients with hemodynamic instability, the anticipated benefits of PostCon could be higher.
Only 1 cardiovascular event occurred. The causes that promote stent thrombosis are multiple, so it is hard to relate this single event to the PostCon protocol itself. The improvement in LVEF at follow-up reflects the myocardial stunning that occurs shortly after reperfusion. Therefore, LVEF at follow-up may better reflect final left ventricle dysfunction, and it should be taken in consideration in future trials that aim to study the impact of novel methods of cardioprotection.
Preconditioning and PostCon seem to share common signaling pathways, 49 and it appears that both generate similar stimulus to the cell surface, which are then transduced to the intracellular targets of cardioprotection. One of its goals is the inhibition of the opening of the mitochondrial permeability transition pore, which is a key player in the process that underlies RI. However, contrary to the negative results achieved by PostCon, preconditioning, manifested as preinfarction angina, has been regularly related to lesser infarct size. 28,50 Also, apparently in the opposite direction from PostCon, remote ischemic conditioning (in which short cycles of transient nonlethal ischemia in an organ or tissue confers resistance to a subsequent lethal ischemia RI in a remote organ or tissue 51 ) has gathered exciting results in patients with STEMI, 48,52 even if the mechanism behind it is still largely unknown. Why PostCon fails to replicate the effects of other methods in promoting cardioprotection despite sharing similar underlying mechanisms remains unknown.
Limitations
The major limitation of our trial is that CMR was not used to quantify the extent of the infarct. Instead, we used troponin and the angiographic AAR as surrogates for infarct size and AAR, respectively. Their limited accuracy should be considered when interpreting the results of our trial. We may also have overestimated the presumed benefits of MTA; given the absence of a group without MTA to address its effectiveness, the significance of the negative findings of PostCon beyond MTA may be questionable. The small sample size limits the power to detect differences in primary and secondary end points, increasing the chance of a type II error. Our small sample size also increases the vulnerability of our study design to confounding; however, this limitation was significantly mitigated by the use of concealed allocation and randomization.
Conclusion
After routine utilization of MTA, PostCon failed to reduce infarct size and to improve LVEF and major clinical events. Our results are consistent with previous studies and together question the presence of a meaningful clinical benefit of PostCon in patients with STEMI treated with current mechanical and pharmacological therapeutic modalities. Given the importance of reperfusion damage, development of further treatments acting on its mechanisms should be pursued.
Footnotes
Author Contribution
André Luz contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Mário Santos contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Rui Magalhães contributed to design, contributed to analysis and interpretation, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. João Silveira contributed to conception, contributed to acquisition and analysis, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Vasco Dias contributed to conception, contributed to analysis, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Sofia Cabral contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Filomena Oliveira contributed to conception, contributed to analysis drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Sousa Pereira contributed to conception contributed to analysis drafted manuscript critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Adelino Leite-Moreira contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Severo Torres contributed to design, contributed to analysis, drafted manuscript, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.