
Abstract
One of the major concerns remaining in the treatment with stenting is the occurrence of stent thrombosis (ST). We reviewed 1960 consecutive patients (mean age 56 ± 11.6 years, 84.6% males) treated with primary coronary stenting for ST elevation myocardial infarction between 2003 and 2008. All clinical, angiographic, and follow-up data were retrospectively collected. The data when the patient had angina pectoris was obtained from medical record. Early ST was observed in 89 (4.5%) patients. We identified 86 patients with early ST and known date and time of symptom onset. In these patients (mean age 59.2 ± 13.9, 83.7% males), symptoms occurred mostly at night time (00.00-6.00
Introduction
Coronary stenting has made a dramatic impact on reducing the incidence of acute vessel closure and has been shown to be a relatively safe and highly effective treatment to relieve angina. 1 Although it is a rare complication (0.5%-1.9%), 2,3 stent thrombosis (ST) is usually associated with a poor prognosis compared to de novo thrombosis. 4 Despite dual antiplatelet therapy, ST results in mortality and myocardial infarction (MI) rates of 26% and 63%, respectively. 5
There appears to be a circadian rhythm in certain cardiac and cerebrovascular events, including stroke, pulmonary thromboembolism, MI, and sudden cardiac death (SCD). 6 –9 The renin–angiotensin–aldosterone system (RAAS) is characterized by a circadian rhythm, which is more active during the night than in the morning. 10 Furthermore, it has also been stated that the parameters that increase cardiac work by altering the heart rate and blood pressure tend to the highest in those hours. 11
Multiple studies have shown that acute MI and SCD are likely to occur on Mondays and in the winter season. 12 –15 It has been accepted that this temporal variation has arisen from mental/physical stress and hemodynamic and hemostatic alterations. 16 –18 Although it is known that acute MI demonstrates daily and seasonal variation, there is no sufficient data regarding the circadian rhythm of ST. Previous studies investigating the effect of circadian rhythm had enrolled patients who needed angioplasty for any reason; we investigated patients who had undergone primary coronary angioplasty.
Methods
Patient Populations
Between October 2003 and March 2008, primary coronary stenting was performed in 2349 patients admitted with the diagnosis of acute MI within 12 hours from the onset of chest pain. The diagnosis of acute MI required the presence of at least 2 of the following 3 criteria: (1) ST-segment elevation or new onset of complete left bundle branch block on an electrocardiogram (ECG) consistent with acute MI; (2) symptoms of myocardial ischemia lasting for 20 minutes, and (3) transient increase in cardiac enzymes to more than 2-fold the normal laboratory value. A total of 389 patients were excluded from the study because of unsuccessful procedures (postprocedural thrombolysis in MI [TIMI] flow <3; n = 274), death during acute intervention due to the development of acute ventricular fibrillation (n = 12), use of drug-eluting stent (DES; n = 64), and cardiogenic shock (n = 39). The population consisted of 1960 patients who were evaluated retrospectively. Early ST was noted in 89 (4.5%) patients. We excluded 3 patients with an unknown date and time of symptom onset. Therefore, the final 86 patients with early ST were investigated. The study protocol was approved by the hospital’s ethics committee. No extramural funding was used to support this study. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the article, and its final contents.
Analysis of Patient Data
A clinical history of risk factors such as age, gender, diabetes mellitus (DM), hypertension, hypercholesterolemia, cigarette smoking, family history for coronary artery disease, MI history, primary coronary intervention, or bypass history was determined from the medical records. A 12-lead ECG was recorded in each patient just after the hospital admission, and the MI type was also recorded from the ECGs.
Onset of early ST was defined as the beginning of typical chest discomfort. Patients who had early ST were grouped by 6-hour intervals depending on the starting time (06.00-12.00/12.00-18.00/18.00-00.00/00.00-06.00) of chest pain. The winter season is described as the period of time from December of the previous year to the last day of March of the following year. After primary coronary stenting, the global left ventricular ejection fraction (LVEF) was measured by transthoracic echocardiography using a system V (GE Vingmed Ultrasound, Horton, Norway), with a 2.5-MHz phased-array transducer. The LVEF was measured using the modified Simpson’s rule. 19
Coronary Angiography and Stenting
All patients received chewable acetyl salicylic acid (300 mg, unless contraindicated) and clopidogrel (300 mg loading dose) prior to the coronary angiography. Emergency coronary angiography and stenting were performed through the percutaneous femoral approach. After visualizing the left and right coronary arteries, 2.5 mg of isosorbide dinitrate was selectively injected into the infarct-related artery (IRA) to rule out the possible coronary spasm. Angiographic assessments were made at the treating hospital by visual assessment. The IRA was graded according to the TIMI classification. 20 Primary coronary stenting was performed only for IRA. Stents were deployed according to the standard techniques. All the patients received unfractionated heparin intravenously during the procedure (70 U/kg bolus), and heparin infusion (to maintain the activated partial prothrombin time between 80 and 150 seconds), or subcutaneous low-molecular-weight heparin (1 mg/kg twice a day) was restarted immediately after application of pressure bandage. The use of glycoprotein IIb/IIIa inhibitors was left to the discretion of the operator. After the stenting, all the patients were prescribed a lifelong acetyl salicylic acid (100 mg daily) regimen, and clopidogrel (75 mg daily) was prescribed for at least 1 month. Concomitant medical treatment with β-blockers, angiotensin-converting enzyme inhibitors, and statins followed according to the guidelines of the American College of Cardiology/American Heart Association (ACC/AHA).
Definition
Stent thrombosis was defined as the occurrence of any of the following events: angiographic proof of stent occlusion, postprocedural MI after successful stent implantation not clearly attributable to another coronary lesion, or unexplained deaths ≤30 days after the procedure. Early ST was defined as thrombosis that occurred in the first 30 days following primary coronary stenting. Early ST was also classified into acute (0-1 days) and subacute (1-30 days). Three-vessel disease was defined as the presence of more than 50% stenosis in 3 major epicardial coronary arteries. Time to reperfusion was measured as the time from the onset of symptoms to the coronary reperfusion acquired with balloon inflation. Door-to-balloon time was defined as the time between hospital admission and balloon inflation. Cardiogenic shock was defined as prolonged hypotension (systolic blood pressure <85 mm Hg), with evidence of decreased organ perfusion caused by severe left ventricular dysfunction, right ventricular infarction, or mechanical complications of infarction. Patients were also evaluated according to the Killip clinical examination classification. 21 Renal failure was defined as a serum creatinine level ≥1.5 mg/dL and/or use of dialysis. Patients with DM were defined as those with documented DM using either oral hypoglycemic agents or insulin treatment on admission. Hypercholesterolemia was defined as total cholesterol of ≥200 mg/dL or use of cholesterol-lowering agents. All deaths and MIs were reviewed independently by 2 interventional cardiologists for ST.
Statistical Analysis
Quantitative variables were expressed as mean value ± standard deviation (SD), and qualitative variables were expressed as percentage. Continuous variables were compared using the independent Student t test and the Mann-Whitney U test, whereas categorical variables were compared by the likelihood ratio χ2 test or the Fisher exact test. A P value of <.05 was considered statistically significant. All statistical studies were carried out using the SPSS program (version 15.0; SPSS, Chicago, Illinois).
Results
The overall incidence of early ST was 4.5% (n = 89), of which 0.9% (n = 19) were acute ST and 3.5% (n = 70) were subacute ST in our 1960 study patients (mean age 56 ± 11.6, years, 1657 males). The median time to development of ST was day 5 following the stent implantation. The baseline angiographic and procedural characteristics in the 2 groups have been summarized in Table 1 . Patients developing ST were significantly older, current smokers, and more commonly had history of percutaneous coronary intervention (PCI) and MI, and were of advanced Killip class. The mean LVEF after primary coronary stenting and use of tirofiban were found to be similar in both groups. When patients with early ST were compared to the group without ST, total stent length was longer (21.56 ± 8.27 vs 18.96 ± 6.29, respectively, P < .001) and smaller (2.98 ± 0.29 vs 3.12 ± 0.34, respectively, P < .001) in patients with early ST. Patients with ST had a lower rate of postprocedural TIMI flow grade 3, and premature clopidogrel discontinuation was significantly higher in these patients.
Baseline Angiographic and Procedural Characteristics of Study Patients.a
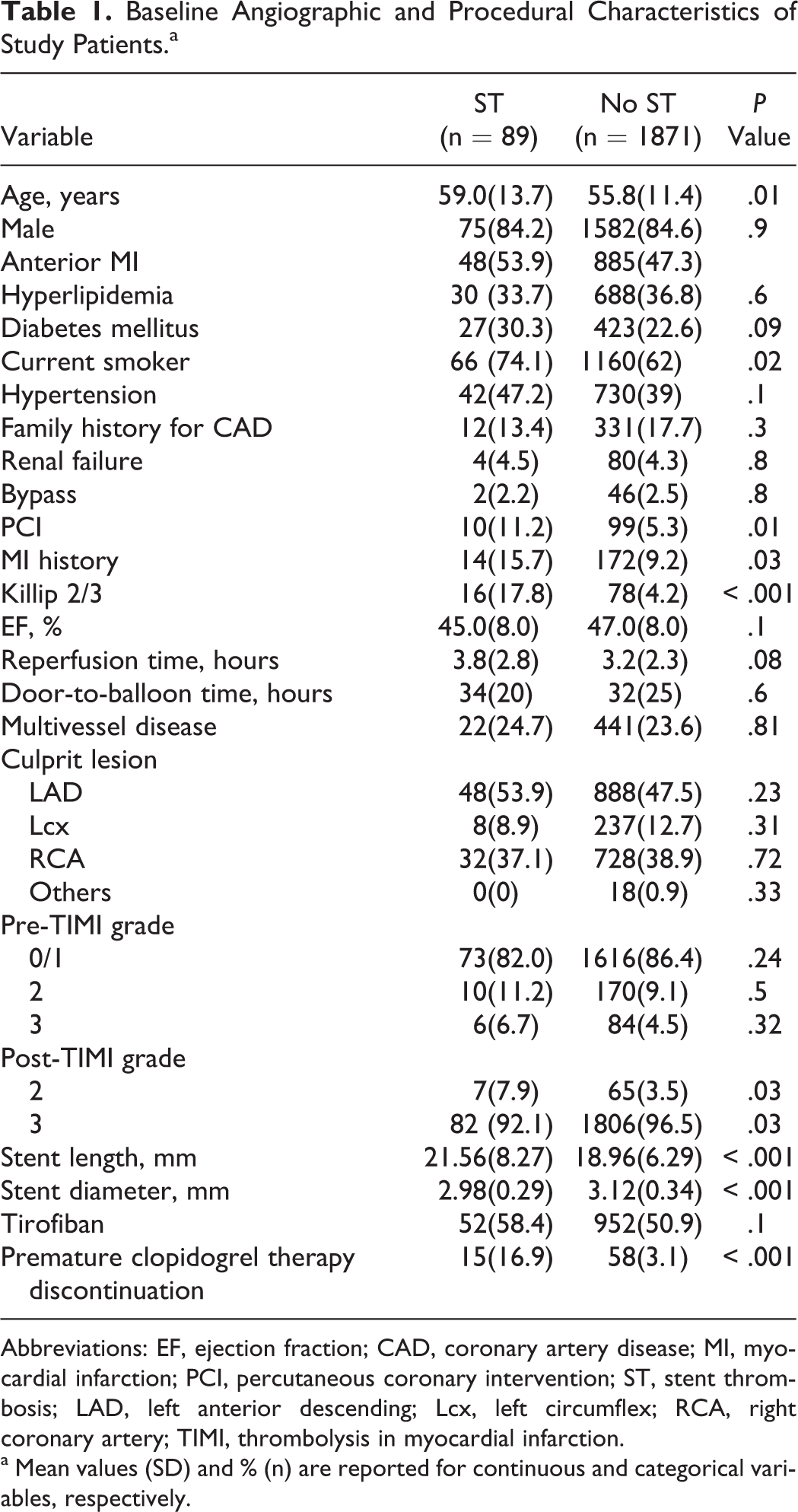
Abbreviations: EF, ejection fraction; CAD, coronary artery disease; MI, myocardial infarction; PCI, percutaneous coronary intervention; ST, stent thrombosis; LAD, left anterior descending; Lcx, left circumflex; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
a Mean values (SD) and % (n) are reported for continuous and categorical variables, respectively.
The mean age of the patients with early ST and known time of symptom onset (86 patients, 83.7% males) was 59.2 ± 13.9 years. In this group, 22 patients (25.6%) with early ST had 3-vessel disease, 46 patients (53.5%) had anterior MI, 27 patients (31.4%) had hyperlipidemia, 59 patients (68.6%) were smokers, 41 patients (47.7%) had hypertension, and 27 patients (31.4%) had diabetes during index procedure. Fourteen patients (16.3%) discontinued antiplatelet therapy prematurely in this group. The baseline angiographic and procedural characteristics during the index procedures of patients with early ST and known time of symptom onset have been summarized in Table 2 .
Baseline Angiographic and Procedural Characteristics During Index Procedure.a
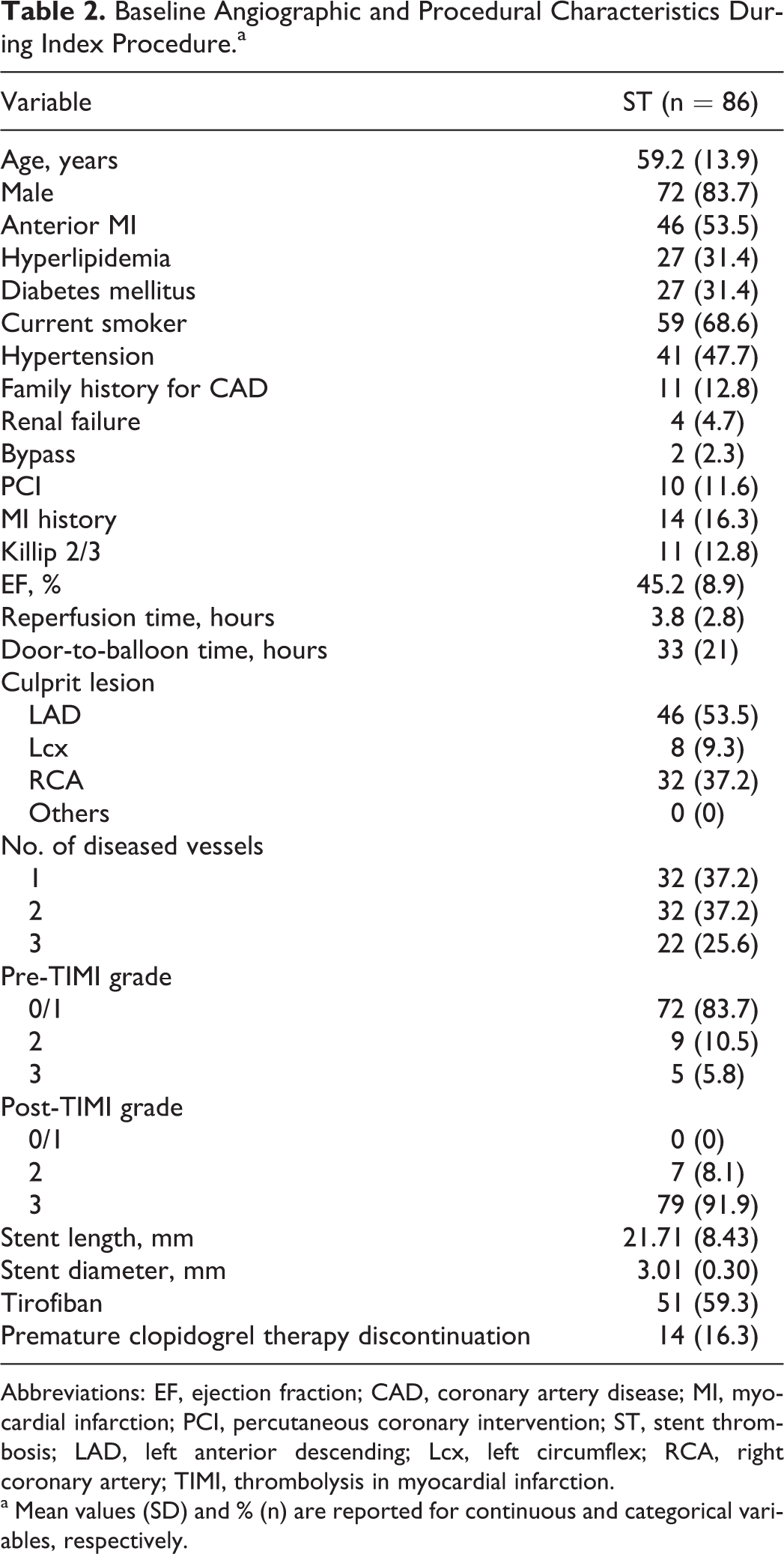
Abbreviations: EF, ejection fraction; CAD, coronary artery disease; MI, myocardial infarction; PCI, percutaneous coronary intervention; ST, stent thrombosis; LAD, left anterior descending; Lcx, left circumflex; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
a Mean values (SD) and % (n) are reported for continuous and categorical variables, respectively.
In patients with early ST and known time of symptom onset, 62 (72%) had ST-segment elevation MI (STEMI), 20 (23%) had unstable angina pectoris, and 4 (5%) had non-STEMI. The time period of onset of angina pectoris in 33 patients (38%) was during the night (00.00
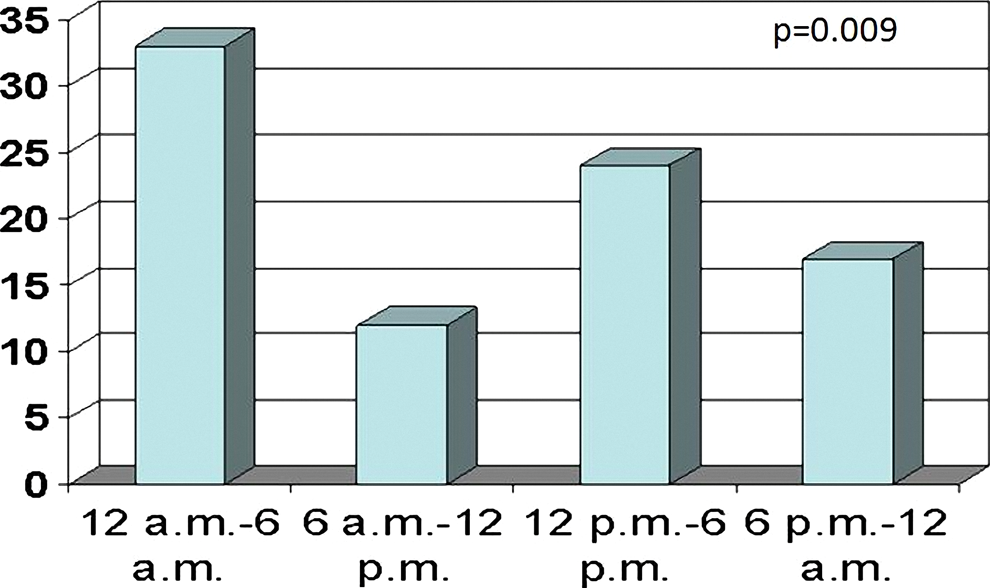
Circadian variation in early stent thrombosis.
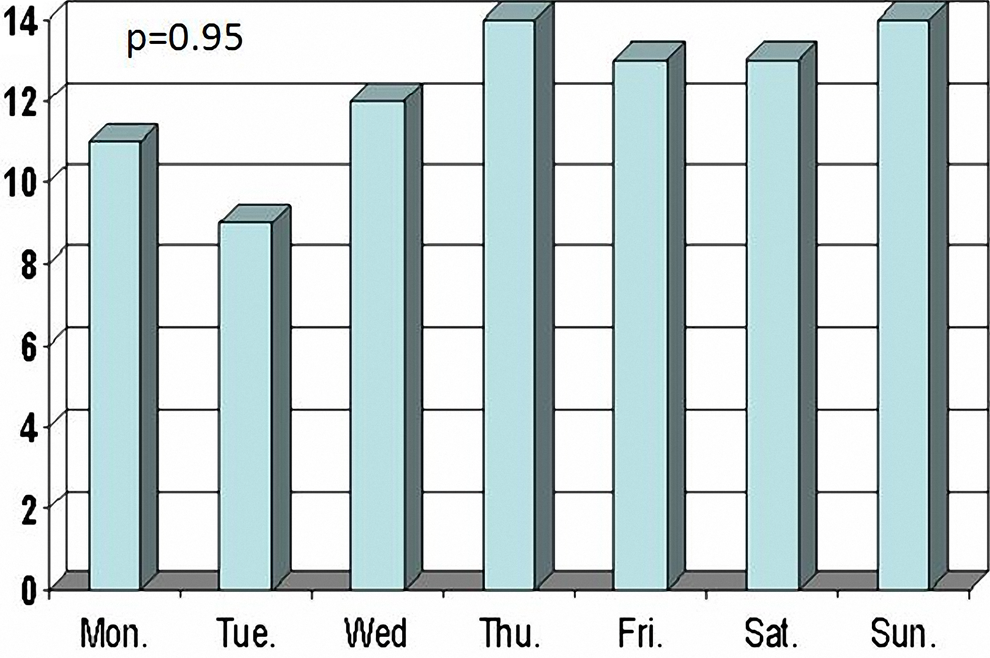
Weekly variation in early stent thrombosis.
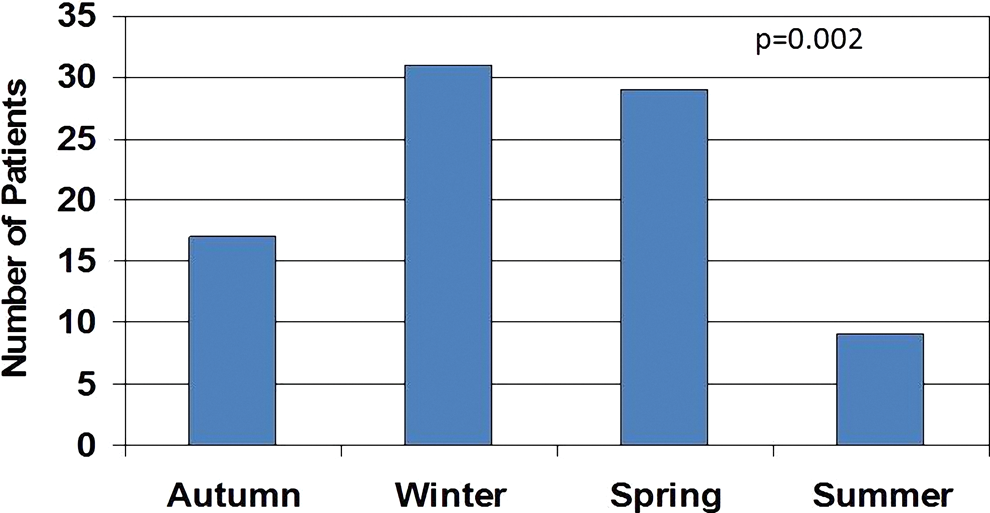
Seasonal variation in early stent thrombosis.
Discussion
We found that early ST was more likely to occur at night in patients who underwent primary coronary intervention due to STEMI. ST occurrences throughout the week were equally distributed, but early ST was more likely to occur in the winter months.
Several physiological mechanisms may trigger early ST during the night. Andreotti et al
22
showed that the activity of plasminogen activator inhibitor (PAI) decreased throughout the day, reaching trace activity at 6
It has been demonstrated in previous studies that acute vascular conditions such as stroke 26 and MI 12,13 are more likely to occur in winter. It is commonly estimated that mortality from coronary heart disease will increase by approximately 1% per 1°C fall in temperature. 27 The reasons underlying the higher occurrence of cardiovascular diseases in winter have remained controversial, but investigators have mostly pointed to cold conditions 28 and respiratory infections, which may trigger attacks of cardiovascular events, as they affect the blood coagulation factors, 29 causing damage to vessel walls. 30 Possible mechanisms include consequences resulting from increased arterial blood pressure and the subsequent increase in myocardial oxygen demand with a simultaneous decrease in coronary blood flow, and hematological changes following cold-induced vasoconstriction and consequent loss of plasma fluid, which predispose the participant to arterial thrombosis. 31,32
We did not find a significant relationship between the onset of ST and the day of the week. In spite of the fact that some studies have demonstrated the most common time for a heart attack to be Monday mornings due to mental stress, 13 our study suggests that mental stress-induced hemodynamic alterations may not play a role in the development of early ST.
The incidence of ST following PCI varies between 0.5% and 6.3%. 33,34 The corresponding rate in the current trial was 4.5%. Incidence rates were found to be lower in patients who underwent PCI due to stable coronary artery disease, and higher in cases who underwent PCI due to acute coronary syndrome (ACS). For example, the rate of post-PCI ST in patients presenting with acute MI was determined as 6.3% in a trial conducted by La Vecchia et al, 34 while in the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial conducted on ACS patients with no ST elevation, 33 the corresponding rate was reported as 1.4%. Higher ST rates in the present study compared to the rates in ACUITY may be due to methodological differences such as enrollment of STEMI cases only, conduction of the trial in a single center, and adoption of a real-world design, instead of a randomized control trial.
We found circadian variation in coronary ST, consistent with other studies (like Tamura and Mahmoud). Tamura et al demonstrated that subacute ST occurred more frequently during the morning. 35 Mahmoud et al demonstrated that early ST followed a circadian rhythm and occurred more often in the early morning hours. This pattern was not significant in late and very late ST. They found no weekly pattern in ST onset as in our study. In contrast to our study, they found that ST was more likely to occur in the summer months. They found that 14% of patients with bare metal stent and early ST had discontinued clopidogrel or ticlopidine before the onset of ST as in our study (this rate was 16.3% in our study). 36 However, there are some differences; in our study, the rate of patients with TIMI-0/1 flow at baseline was 83.7%, and all patients had STEMI. Their study population mostly comprised patients who had undergone elective coronary stenting, and the preprocedural TIMI-0/1 flow was only 19.7%. Moreover, 71.2% of the patients who presented with early ST had ST segment elevation in our study, and this rate was 47% in their study.
Limitations
Several limitations need to be kept in mind when interpreting the results of this study. This study has a retrospective design which per se is a well-known limitation. Since we have not yet encountered patients developing thrombosis after DES implantation, the present study did not include such patients. We enrolled patients with definite and probable ST. Finally, we did not take into account some mechanisms that may have triggered ST, such as stress, infection, or surgery.
Conclusion
Early ST follows a circadian rhythm with a peak at night. Occurrences throughout the week were equally distributed, but early ST was more likely to occur in the winter months.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.