
Abstract
Acute upper or lower Gastrointestinal bleeding (GIB) is a clinical emergency in which transfusion can be lifesaving. An individualized and restrictive transfusion strategy is recommended. This study aims to analyze and evaluate GIB transfusion practices during one year in a large tertiary hospital in Lisbon, Portugal. All patients with GIB and transfusion support during 2014 were identified and clinical data collected and statistically treated. There were 1005 GIB transfusion episodes, in a total of 494 patients. Upper GIB was more common. The median haemoglobin concentration that triggered RBC transfusion was 7,6 g/dL with a median of 2 RBC per episode. In 21,9% of episodes, RBC were used in combination with other therapies, in 70,8%, only RBC were administered and in 7,3% RBC were not used at all. In the subgroup of patients receiving FC and/or PCC there were higher median of blood products transfused: RBC (3 17 units), FFP (3 units), PC (1 unit). In a large percentage of the transfusion episodes for GIB, only RBC were used whereas only 7,3% of the GIB didn't require RBC transfusion. Patients requiring FC and/or PCC, needed more allogenic components. We observed, in accordance with the latest clinical practice guidelines and the published literature, a restrictive transfusion approach in our clinical practice.
Introduction
Gastrointestinal bleeding (GIB) is a common clinical emergency linked to a significant burden of morbidity and mortality. 1 GIB is a common indication for red blood cell (RBC) transfusion in order to improve oxygen delivery and haemostasis. 2 Even though most cases of GIB do not entail haemodynamic compromise, transfusion can be lifesaving in patients with massive bleeding. 3 Previous randomized controlled trials have shown non-inferiority of restrictive transfusion strategies, even for critically ill GIB patients.4‐8 Furthermore, a recent meta-analysis supports restrictive transfusion policies over liberal transfusion policies for acute GIB. 9 It is therefore currently recommended that a restrictive transfusion strategy should be enforced, using blood components and coagulation factor concentrates (CFC) with selective goal-directed criteria, 1 in combination with a multimodal and multidisciplinary approach.
Patients with active bleeding and hypovolemia may require RBC transfusion despite an apparently initial normal haemoglobin (Hb), particularly if the patient remains haemodynamically unstable despite appropriate fluid resuscitation. Patients without active bleeding who become haemodynamically stable with fluid resuscitation should receive a blood transfusion if the Hb is <8-9 g/dl and <7 g/dl in high and low-risk patients, with and without cardiac diseases respectively. 1 However, it is important to avoid overtransfusion, especially in patients with suspected variceal bleeding, as this may cause volume overload and exacerbate the bleeding. 1
In a recent survey of 815 UK clinicians, most stated they believed a limited use of RBC transfusion to be appropriate, whereas actual observed practice indicated otherwise. 10 Moreover, the study revealed significant disparity in selected Hb transfusion triggers between physicians of distinct medical specialities and their clinical experience. Clinical reasoning and risk assessment for transfusion in GIB is not completely defined yet, hindering the objective definition of appropriate Hb transfusion triggers. The wide variation of Hb transfusion triggers between different clinicians, hospitals and countries ultimately results in a wide variation in GIB transfusion practice.
In order to assess and evaluate GIB transfusion practices, we performed analysis of all GIB-related transfusion episodes that occurred during one year in a large tertiary hospital in Lisbon, Portugal, including demographics, clinical data, therapeutic outcomes and analytical information.
Materials and Methods
This retrospective analysis included all allogeneic transfusions of blood components and CFC in GIB patients (including upper, lower and not specified) from the Department of Transfusion Medicine, North Lisbon University Hospital Center - Santa Maria Hospital (HSM), during 2014. Clinical charts were reviewed for demographic, clinical and laboratory information from each patient and transfusion request. Clinical and analytical information was gathered both before and after each transfusion episode, in order to evaluate transfusion efficacy. Haemodynamic instability was defined as systolic blood pressure <100 mm Hg or heart rate >100 bpm with a shock index ≥1.0, in a patient with haemorrhage.
Basal diagnosis, comorbidities, anticoagulant and anti-platelet therapy were also evaluated. The clinical department requesting the blood transfusion was also recorded.
Statistical analysis of continuous variables was conducted using Shapiro-Wilk test to evaluate departure from normality. Descriptive data were presented as median and interquartile range for continuous and count plus frequency for categorical variables. Data analysis was performed using SPSS 17.0.
Results
This analysis studied 1005 GIB transfusion episodes (65,6% of which were males) in a total 494 patients (of which 59,7% males), with a median age of 75 years (age range :1 month-96 years old; interquartile range, IQR, 61-83 years).
Descriptive data of the patients’ demographic and clinical characteristics are presented in table 1. In this tertiary care single-centre (HSM), patients with upper GIB (UGIB) constituted 60,2% (n = 605) of all transfusion episodes, patients with lower GIB (LGIB) comprised 25,7% (n = 258) of all transfusion episodes and the anatomical location of GIB (above or under Treitz ligament) of the remaining 14,1% (n = 142) could not be specified.
Descriptive data of participants and blood transfusion episodes.

IQR, interquartile range; GIB, gastrointestinal bleeding.
It was observed that 18,6% of all patients (12,2% of transfusion episodes) presented with unstable haemodynamic status, while 7,1% were in hypovolemic shock (4,8% of transfusion episodes) at the time of request of the blood transfusion (Table 1). 127 out of the 494 (25,7%) patients exhibited haemodynamic compromise, the majority of which were men (70%). Of these, 66,1% had UGIB (n = 84), 24,4% had LGIB (n = 31) and GIB location could not be specified in the remaining 9,4% of patients.
The gastrointestinal diagnosis (27,7% of all patients) underlying GIB included, among others, gastrointestinal ulcers (31.4%), angiodysplasia (10,2%) and liver disease (34.3%) of which 95,7% presented with oesophageal variceal bleeding. 12.6% of the patients included in the study had solid tumors, 79% of which were located in the gastrointestinal tract (42,8% of which were located in the stomach). Haematological pathologies, mostly of oncohaematological nature, were present in 6,3% of patients, whereas hypocoagulation accounted for another 6,3%. Sepsis and kidney failure with haemodialysis accounted for 1,4% and 2,0% of patients, respectively. The main comorbidities observed in the global population of this study (n = 494) were cardiac (n = 58), haematological (n = 31), renal (n = 31) and gastroenterological (n = 21) diseases. Five medical departments were the top transfusion prescribers, comprising 83,1% of transfusion episodes in patients with GIB (Table 1).
When considering all transfusion episodes, the median haemoglobin (Hb) trigger value for transfusion was 7,6 (6,8-8,3) g/L. For UGIB the Hb trigger was 7.5 (6.8-8.2) g/L, whereas for LGIB it was 7,7 (6.9-8,5) g/L. The comparison of laboratorial haematologic parameters at the time of pre-transfusion between UGIB and LGIB showed a significantly lower haemoglobin (Hb) cut-off value for UGIB (p = 0.004).
The allogeneic blood components included in the majority of cases RBC concentrates (n = 932, 92,7%). In 70,8% (n = 712) transfusion episodes were undertaken using exclusively RBC, 21,9% (n = 220) using RBC combined with other transfusion therapy, and 7,3% (n = 73) transfusion episodes without RBC. These last percentages were similar among UGIB and LGIB patients. Furthermore, the amount of consumed blood components and CFC was similar between patients with GIB in distinct anatomical locations (Table 2). Spearman correlation coefficient analysis demonstrated a positive association between the pre-transfusion Hb level and the amount of RBC units (r = 0.438, p < 0.0001).
Descriptive pre-transfusion analytical status and transfused blood components in UGIB versus LGIB.
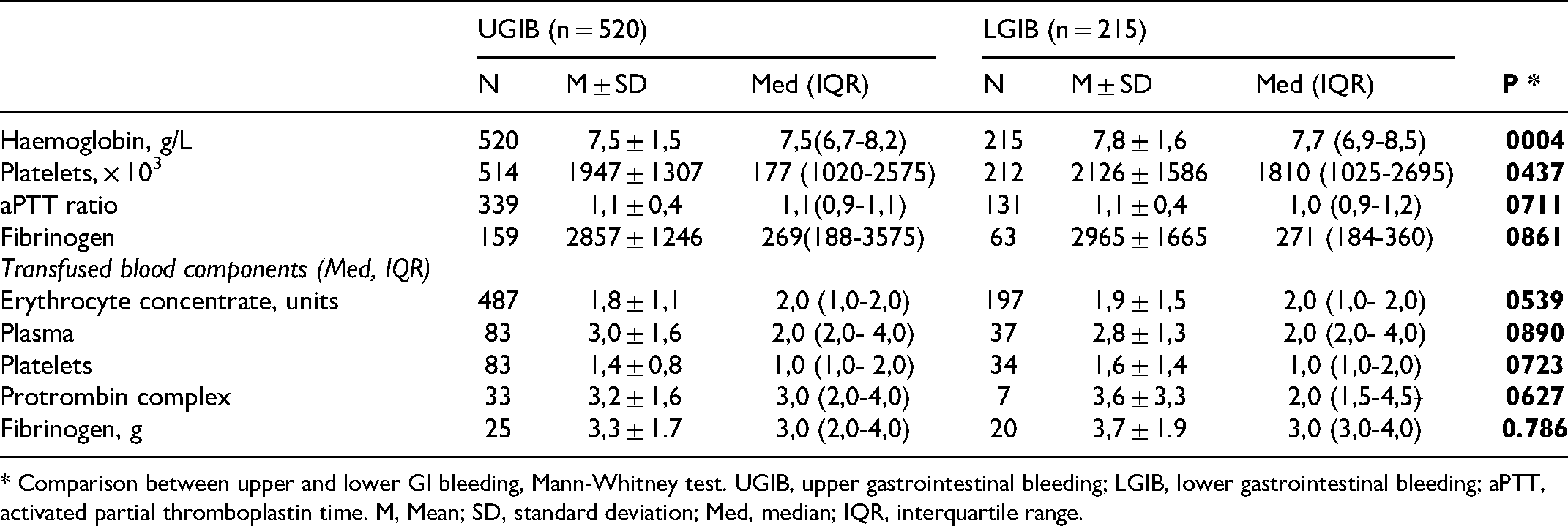
* Comparison between upper and lower GI bleeding, Mann-Whitney test. UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; aPTT, activated partial thromboplastin time. M, Mean; SD, standard deviation; Med, median; IQR, interquartile range.
Transfusion efficiency was evaluated through the comparison of pre-transfusion and post-transfusion Hb values. We found that there was a significant increment of 8-to-31.2% in Hb values, in any pre-transfusion Hb group below 9 g/L(Table 3). Moreover, the magnitude of transfusion efficacy was calculated to assess the impact of different blood component transfusion strategies, by anatomical location of GIB and pre and post-transfusion Hb level values. It was found that the type of blood component transfused does impact Hb increase, with RBC transfusion eliciting the best treatment responses, probably due to lower bleeding severity (Figure 1).

Impact of blood component transfusion strategies, by anatomical location of GIB and pre-transfusion haemoglobin in the variation of haemoglobin level (magnitude of effect), median and interquartile range UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; Hb, haemoglobin; * Kruskal-Wallis test was used to compare differences in magnitude of effect between strategies of components transfusion; EC, erytocyte concentrate; ** Mann Whitney test, no EC versus only EC, P < 0.0001, no EC versus with EC, P < 0.0001 and only EC versus with EC, P = 0.006; a Kruskal-Wallis test followed by Mann Whitney test: no EC versus only EC, P = 0.067, no EC versus with EC, P = 0.145 and only EC versus with EC, P = 0.084; b Kruskal-Wallis test followed by Mann Whitney test: no EC versus only EC, P = 0.196, no EC versus with EC, P = 0.388 and only EC versus with EC, P = 0.036; c Kruskal-Wallis test followed by Mann Whitney test: no EC versus only EC, P = 0.028, no EC versus with EC, P = 0.089 and only EC versus with EC, P = 0.54036.
Magnitude of effect and variation of median haemoglobin level with blood transfusion by pre-transfusion haemoglobin groups.

Median (interquartile range); * Mann Whitney test.
It was observed 15% (n = 151) transfusion episodes where no Hb values were registered pre and/or post-transfusion.
Analyzing the consumes associated to the subgroup where fibrogen concentrates (3 g, IQR 2-4) and/or prothrombinic complexes concentrate (1000 UI, IQR 1000-2000) it could be observed higher median consumption per transfusional episode (3U CE (IQR 2-4), 3U PFC (IQR 2-4) and 1CP (IQR 1-2). For this subgroup the main diagnose is gastrintestinal and part of the patients was under oral anti-coagulants, specially those to whom prothrombinic complexes concentrate was administered.
Discussion
The need for blood transfusion in GIB seems to vary according to anatomical site.11,12 Bleeding location in relation to the Treitz ligament determines whether it is considered a UGIB or LGIB. In this study, GIB-associated blood transfusions were mostly due to UGIB (60,2%), in comparison with LGIB (25,7%).
Transfusion practices must be individualized, taking into consideration patient comorbidities and risk factors and according to specific targets in a goal-directed approach, taking advantage of point-of-care/viscoelastic tests,13‐21 A large study in the UK revealed that 38% of patients presented with haemodynamic instability at the time of blood transfusion due to UGIB. 10 In our overall population, 25,7% (n = 127) patients presented with haemodynamic instability, 66% (n = 84/127) of which were due to UGIB.
Criteria for the use of RBC transfusion in GIB remains non-consensual in clinical guidelines.
Frequently, RBC are transfused triggered by low Hb values, below a threshold where is believed the benefits of transfusion outweigh the risks of anaemia. 4 Nevertheless, in clinical practice the decision to transfuse is made through the subjective perception of clinical assessment and the appropriate Hb trigger. Transfusion Hb triggers vary between different clinicians and different hospitals, resulting in wide variations in RBC transfusion practice;22‐24 Overall, in the current study, the median Hb trigger value for transfusion was 7,6 (IQR 6.8-8.3) g/L. However, the Hb trigger for UGIB [7,5 (6,8-8,2)] g/L was significantly lower than for LGIB [7,7 (6,9-8,5)] g/L. According to the most recent guidelines for GIB management, a restrictive transfusion strategy is recommended (Grade 1A),4,25,26 with a Hb threshold value of 8 g/dl18,27 and 7 g/dl in patients with and without heart disease, respectively.13,25 Moreover, it is currently recommended that patients with and without heart disease maintain a Hb target range of 8-10 g/dl and 7-9 g/dl after transfusion, respectively (Grade 1A),18,25,27,28 even during active bleeding episodes (Grade 1C). 13
In this analysis is observed a post-transfusion global median Hb value 8,8 (IQR 7,9-9,6), according to the literature.
The subgroups where fibrogen concentrates (3 g, IQR 2-4) and/or prothrombinic complexes (1000 UI, IQR 1000-2000) administered presents an higher percentage of patients with hemodynamic changes and/or hypovolemic shock. In this subgroup the median pre transfusion value of haemoglobin was lower and coagulopathies were documented by clinically relevant changes in TP and/or aPTT as well as lower pre transfusion levels of fibrogen.
The main purposes of blood transfusion are to correct global or regional oxygen delivery and/or to improve haemostasis28,29 However, evidence does not support increasing oxygen delivery with RBC transfusion when Hb is over 7 g/dl, unless the patient has cardiac disease, or chronic pulmonary disease. 18 About the effects of blood transfusion on haemostasis, it is known that the haematocrit (Htc) has influence on it, as a low Htc can be partially responsible for increased bleeding.28,29 The optimal Htc to sustain haemostasis in a bleeding patient is still unknown. This threshold Htc could be around 30%, but no study, at this moment, has validated this suggestion. 28 Some authors in chronic kidney disease recommends to correct the anaemia, targeting a Htc to 30% to lower bleeding (Grade 1C). 16 In this study, we demonstrate that patients transfused with RBC improved significantly Hb levels, despite this effect was verified to be more pronounced in those with lower Hb values before transfusion.
After analyzing our hospital experience, that reflects our context and reality, we can conclude that we favor a restrictive transfusion approach, in accordance with the latest clinical practice guidelines and the published literature.
Further clinical studies could evaluate other relevant clinical outcomes in the assessment of transfusion role, particularly short-term hospital mortality.
Footnotes
Author Contributions
All authors contributed towards the concept of the paper, data collection and analysis and writing of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
For this retrospective analysis, it was waived of informed consent. The analysis looked retrospectively at outcomes for a large cohort of patients treated. All data analysed were collected as part of routine diagnosis and treatment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.