
Abstract
Whether the use of acid suppressants can reduce non-vitamin K oral anticoagulants (NOACs)-related gastrointestinal bleeding (GIB) remains unclear. To systemically evaluate the effect of acid suppressants on the risk of GIB in patients treated with NOACs. All related studies were searched in four databases (Cochrane, Embase, PubMed, and Web of Science) from their establishment to August 10, 2021. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used to identify studies and Stata 16.0 software was used for meta-analysis, including sensitivity and subgroup analysis. Six retrospective cohort studies were included in this study. The use of acid suppressants significantly reduced the GIB risk in patients taking NOACs, with an overall relative risk (RR) of 0.70 (95% confidence interval [CI]: 0.61-0.82; P < 0.001; I2 = 56.3%). This trend of reduced risk for GIB in NOACs was more significant in upper GIB (UGIB; RR: 0.45; 95%CI: 0.22-0.90; P = 0.025; I2 = 71.1%). The reduction was stronger for dabigatran than for rivaroxaban and apixaban. The least reduction in the risk of GIB with acid suppressant co-therapy was rivaroxaban (dabigatran: RR: 0.53; 95% CI: 0.45-0.62; P = <0.001; I2 = 39.8%; apixaban: RR: 0.67; 95% CI: 0.54-0.84; P = <0.001; I2 = 0; rivaroxaban: RR: 0.73; 95% CI: 0.66-0.81; P = <0.001; I2 = 37.6%). The included studies revealed the protective effect of acid suppressants against NOACs-related GIB, especially in the upper gastrointestinal tract. The protective effect was even stronger in patients using dabigatran than in those using Xa inhibitors (rivaroxaban and apixaban).
Keywords
Introduction
Non-vitamin K oral anticoagulants (NOACs), including direct factor Xa inhibitors (rivaroxaban, apixaban, and edoxaban) and direct thrombin inhibitors (dabigatran), are currently widely used in clinical practice. Compared to warfarin, they have advantages in preventing non-valvular atrial fibrillation-related stroke and arterial thrombosis, with faster onset and offset of action, fewer drug interactions, and no need for routine international normalized ratio (INR) monitoring and dose adjustment.1–3 However, it has been found in phase III clinical trials after the drug is marketed or in real-world observational studies that compared with warfarin, NOACs have a higher risk of gastrointestinal bleeding.4–6 A meta-analysis of four large phase III RCTs after NOACs is marketed presented that compared with warfarin, NOACs increase the overall risk of gastrointestinal bleeding by 25% (risk ratio [RR]: 1.25; 95% confidence interval [CI]: 1.01-1.55; P = 0.04). 6 In a recent meta-analysis involving 43 RCTs and 41 real-world studies, rivaroxaban was associated with an increased risk for major GIB (RR from RCTs: 1.39; 95% CI: 1.17-1.65; hazard ratio [HR] from real-world studies: 1.14; 95% CI: 1.04-1.23; P = 0.06). 4 Another real-world study showed that dabigatran was associated with a higher risk of GIB than warfarin (HR: 1.85; 95% CI: 1.64-2.07; P < 0.001). 5
Although some previous observational studies suggested that acid suppressants should be considered in patients receiving NOACs to prevent GIB, the effect of acid suppressants, including proton pump inhibitors (PPIs) and histamine 2 receptor antagonists (H2RAs), in the prevention of GIB, remains undefined. A previous meta-analysis aimed to evaluate the protective effect of acid suppressants on oral anticoagulant-related GIB showed that the protective effect was only valid for warfarin (RR: 0.56; 95% CI: 0.38-0.83; P = 0.004;I2 = 0), but not for dabigatran (HR: 0.78; 95% CI: 0.44-0.1.37; P = 0.386; I2 = 81.7%). 7 However, a retrospective cohort study from Hong Kong suggested that PPI was more effective for high-risk patients with GIB (previous history of GIB or peptic ulcers). 8 At present, there is no special focus on the prevention of direct factor Xa inhibitor-related GIB.
In this article, we systematically reviewed and evaluated the current evidence regarding the effect of acid suppressants on NOACs-induced GIB. Six retrospective cohort studies were included in this study. The use of acid suppressants significantly reduced the risk of GIB in patients taking NOACs (RR: 0.70; 95% CI: 0.61-0.82; P < 0.001; I2 = 56.3%). This trend of reduced risk for GIB in NOACs was more significant in upper GIB (UGIB; RR: 0.45; 95% CI: 0.22-0.90; P = 0.025; I2 = 71.1%). The reduction was stronger for dabigatran than for rivaroxaban and apixaban. The least reduction in the risk of GIB with acid suppressant co-therapy was rivaroxaban (dabigatran: RR: 0.53; 95% CI: 0.45-0.62; P = <0.001; I2 = 39.8%; apixaban: RR: 0.67; 95% CI: 0.54-0.84; P = <0.001; I2 = 0; rivaroxaban: RR: 0.73; 95% CI: 0.66-0.81; P = <0.001; I2 = 37.6%). These results revealed the protective effect of acid suppressants against NOACs-related GIB, especially UGIB, which was even stronger in patients using dabigatran than those with Xa inhibitors (rivaroxaban and apixaban).
Methods
This systematic and meta-analysis strictly adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 9
Search Strategy
We performed a systematic and comprehensive search in four databases (Cochrane, Embase, PubMed, and Web of Science). The date ranged from inception to August 10, 2021. A detailed search strategy is presented in Supplemental Material 1. Two reviewers (Yongqi Dong and Xue Li) independently reviewed the titles and abstracts manually. The full text of the study that met the inclusion criteria was reviewed, and the references were searched to retrieve related studies. Discrepancies between reviewers were resolved by consensus or adjudicated by a third reviewer (ZhiHang Zhou).
Selection Criteria
Inclusion criteria for the studies were as follows: patients aged ≥18 years who were newly prescribed with apixaban, dabigatran, rivaroxaban, or edoxaban; those who were concomitantly prescribed with PPIs or H2RAs with NOACs; those who were not receiving PPIs or H2RAs co-therapy; with an outcome of GIB after NOACs were prescribed; the study should give the relative risks (RRs), hazard ratios (HRs), or incidence ratios (IRs), odds ratios (ORs), and corresponding 95% CIs, or the specific event number to calculate them; and the full text was available and published in English.
Studies that met at least one of the following exclusion criteria were excluded: guidelines, expert position, or consensus; brief reports, case reports, letters, comments, or protocol studies; review and meta-analysis articles; and animal or cell studies and studies with incomplete data.
Data Extraction
Two reviewers (Yongqi Dong and Xue Li) independently extracted the data. All disagreements were resolved by consensus with a third reviewer. The extracted data included PMID, the first author’s name, country, year of publication, type of study design, study period, adjusted RRs, HRs, or ORs, or incidence rate ratios (IRRs), and the corresponding 95% CIs. We also extracted the number of patients who received NOACs alone, with acid suppressant co-therapy, and those who developed GIB.
Methodological Quality
The Newcastle–Ottawa Scale (NOS) (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) was used to assess the quality of each included study independently by the same two reviewers. All disagreements were resolved by consensus with a third reviewer.
Publication Bias
Since data analysis included less than 10 studies, publication bias could not able to be evaluated in this meta-analysis. 10
Statistical Analysis
Stata 16.0 software was used to conduct the meta-analysis. The quantity of heterogeneity of the included study was measured by the Cochran's Q and I2 test developed by Higgins, with an I2 value >50% considered to represent a statistically high degree of heterogeneity. The random effects model was used to calculate pooled effect sizes with 95% CIs if Q-test's P < 0.05 or I2≤50%; otherwise, the fixed effects model was used. Statistical analyses were two-sided, and P values <0.05 were considered statistically significant.
Results
Study Inclusions
The search strategy is shown in Figure 1. A total of 2136 articles were identified by the initial search of the four databases. After removing 438 duplicates, 1661 studies were excluded by carefully reading the titles and abstracts. The full text of the remaining 37 studies was assessed for eligibility. Thirty articles were excluded because 18 were brief reports, four were incomplete data, two were reviews, two compared with warfarin, two were duplicate data, one was a protocol study and one was a meta-analysis. Finally, six retrospective studies and only one RCT were identified.8,11–16 Considering the differences in study design, evaluation methods, and evidence levels between RCTs and retrospective studies, we included six retrospective studies in the final meta-analysis.8,11–15
Characteristics of the Studies
The characteristics of these studies are presented in Table 1. Considering the different types of research, data synthesis and merge conducted in the six retrospective cohort studies, which included 559,422 patients who newly started anticoagulant treatment. However, one study by Teerapat Nantsupawat et al. (total number of patients = 247) did not mention whether patients received NOACs for the first time. The sources of data in the four studies were obtained from the nationwide insurance and medical beneficiary databases, and the other two studies were obtained from the hospital database. Half of the studies were conducted in the United States and the other three in Asia (two in South Korea and one in Hong Kong, China). The indications for NOACs in the four studies were the prevention of stroke and systemic embolism in patients with atrial fibrillation or other patients who need prevention or treatment of acute vein thrombosis or pulmonary thromboembolism, while others only enrolled patients with atrial fibrillation. As for NOAC types, three studies focused only on dabigatran, while the other three studies also focused on other NOACs (rivaroxaban, apixaban, and edoxaban),11,12,14 two of which performed subgroup analyses.12,14 As for intervention, four studies enrolled patients undergoing PPIs or H2RAs co-therapy, and the other two studies included those who were concomitantly administered with PPIs, although none of them had further analyzed the two different types of acid suppressants or different types of PPIs. The clinical outcomes in two studies11,12 were upper GIB and the others were overall GIB.8,13–15 Statistical measures of outcomes were presented by adjusted HR in four studies, adjusted OR in one study, and adjusted IRR in two studies.
Feature of included studies.

GIB: gastrointestinal bleeding; UGIB: upper gastrointestinal bleeding; PPI: proton pump inhibitor; H2RA: histamine type 2 receptor antagonist; NOACs: Non-vitamin K Oral Anticoagulants; HR: risk ratio IRR: incidence rate ratio; OR: odds ratio; CI: confidence interval
The evaluation of study quality using NOS is presented in Table 2. NOS scores ranged from 5 to 8, with an average of 7. None of the studies demonstrated whether GIB was present at the start of the study. Two studies were reviewed for less than 3 years and only included patients with an indication for atrial fibrillation; therefore, the corresponding item scored 0 points.
NOS scores of included studies.

Overall GIB on NOACs with or Without Acid Suppressant co-Therapy
As shown in Figure 2A, the pooled outcome of six studies showed the protective effect of acid suppressants on NOACs-related GIB (RR: 0.70; 95% CI: 0.61-0.82; Z = −4.542; P < 0.001; I2 = 56.3%; random-effects model). Figure 2B presents the calculated RR according to the number of specific events. Considering Chan et al. did not give the respective number of GIB events in the acid and non-acid suppressants groups separately, we excluded this study. In total, 115,547 patients were prescribed with NOACs with acid suppressant co-therapy and 439,081 patients were prescribed with NOACs without acid suppressant co-therapy. A total of 1078 patients developed GIB in acid suppressants and 3100 in without acid suppressants. Acid suppressants use was not associated with a decreased risk of GIB (RR: 1.17; 95% CI: 0.94-1.45; Z = 1.385; P = 0.166; I2 = 75.1%; random-effects model).
Sensitivity Analysis
To reveal the source heterogeneity, a sensitivity analysis was conducted, in which one study at a time was removed and recalculated the combined estimate for the remaining study. When Lauffenburger et al.’s study was excluded, the heterogeneity of the results was significantly reduced, and the combined risk estimate of GIB was consistent and without apparent fluctuation (RR: 0.66; 95% CI: 0.63-0.69; Z = −16.420; P < 0.001; I2 = 0; fixed-effects model) (Figure 3). To verify the stability of the pooled result, another sensitivity analysis that only included studies that used HR as an indicator of outcome was conducted. The result was consistent, and acid suppressants also had a protective effect against NOACs-related GIB. (HR: 0.72; 95% CI: 0.53-0.98; Z = −2.093; P = 0.036; I2 = 68.2%; random-effects model) (Supplemental Material 3).
Subgroup Analysis
The occurrence of UGIB/GIB according to subgroups
The incidence of UGIB was analyzed further. The risk of UGIB was further reduced in patients with acid suppressants, although there was no significant difference (UGIB: RR: 0.45; 95% CI: 0.22-0.90; Z = −2.240; P = 0.025; I2 = 71.1%; GIB: RR: 0.76; 95% CI: 0.55-1.05; Z = −1.684; P = 0.092; I2 = 76.1%; random-effects model). The overall RR was consistent with the previous results (RR: 0.67; 95% CI: 0.56-0.82; Z = -3.945; P = <0.001; I2 = 74%; random-effects model) (Figure 4). These results revealed that acid suppressants have stronger effect in preventing UGIB.
Subgroup analysis of the types of NOACs
NOACs include direct factor Xa inhibitors (rivaroxaban, apixaban, and edoxaban) and direct thrombin inhibitors (dabigatran). The largest reduction in GIB risk with acid suppressant co-therapy was observed in the dabigatran group. (RR: 0.53; 95% CI: 0.45-0.62; Z = −7.887; P = <0.001; I2 = 39.8%; fixed-effects model). Moreover, the protective effect of acid suppressants was slightly greater in the apixaban group than in the rivaroxaban group (apixaban: RR: 0.67; 95% CI: 0.54-0.84; Z = −3.573; P = <0.001; I2 = 0; rivaroxaban: RR: 0.73; 95% CI: 0.66-0.81; Z = -5.989; P = <0.001; I2 = 37.6%; fixed-effects model) (Figure 5).

Flow chart of study selection.
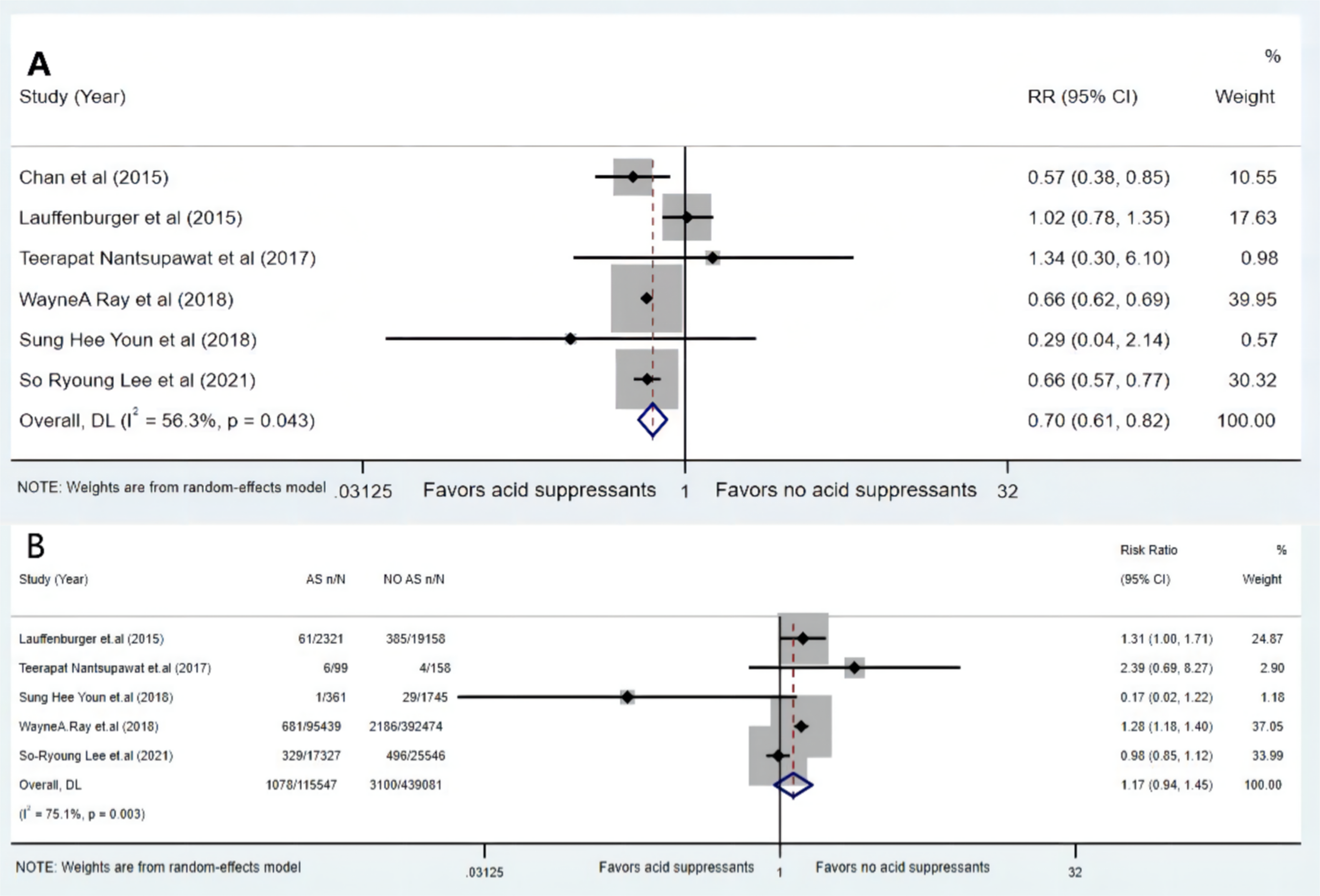
Forrest plot for meta-analyses demonstrating the effect of acid suppressants on NOACs related gastrointestinal bleeding A: The pooled effect calculated by risk ratio (random-effects model) B:The pooledeffect calculated by event number (random-effects model); RR: risk ratio; CI: confidence interval; AS: acid suppressant.

Forrest plot for sensitivity analysis after excluding high heterogeneity study (fixed-effects model) ; RR: risk ratio; CI: confidence interval.
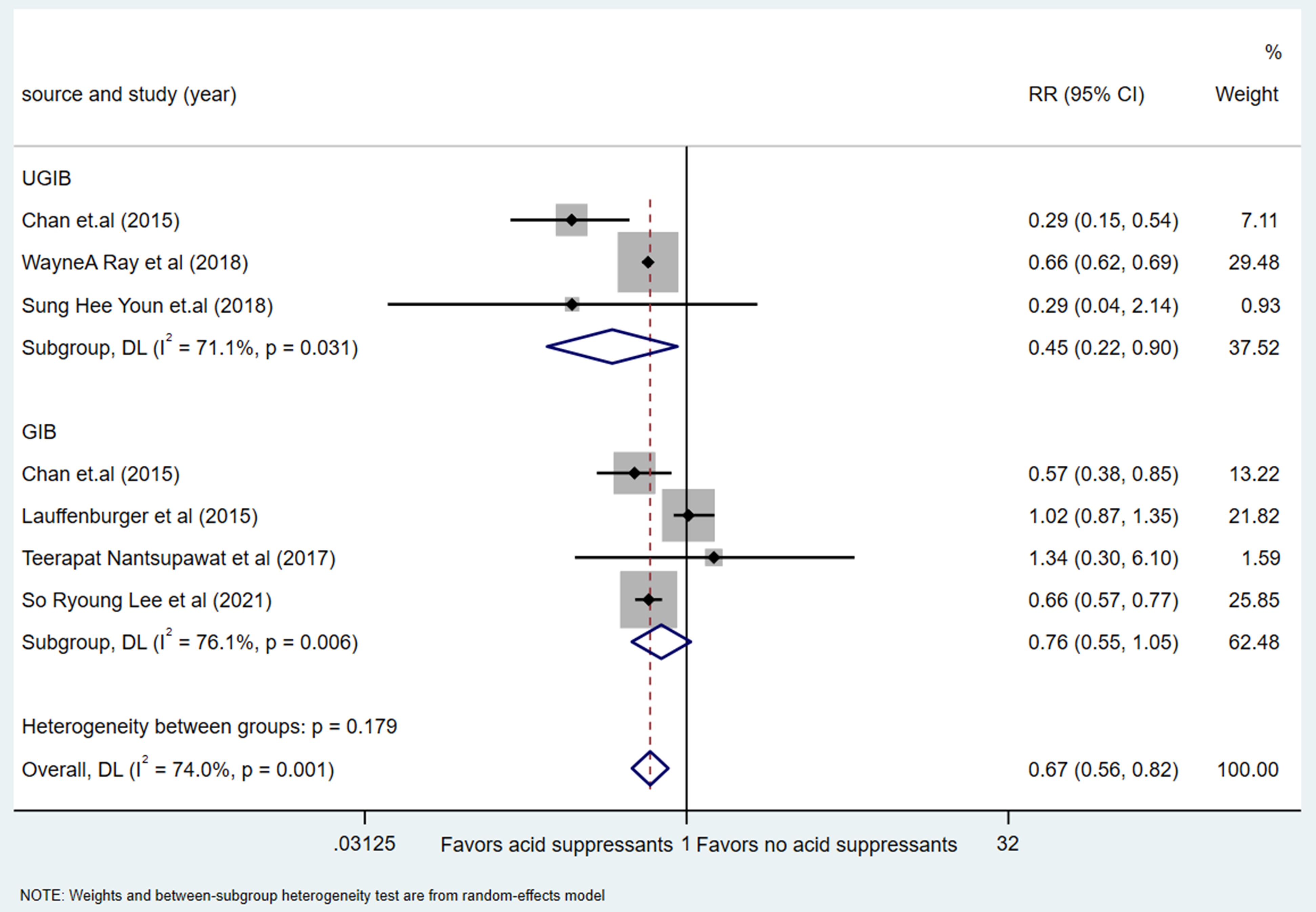
Forrest plot for subgroup analysis based on the occurrence of UGIB/GIB (random-effects model) RR: risk ratio; CI: confidence interval.
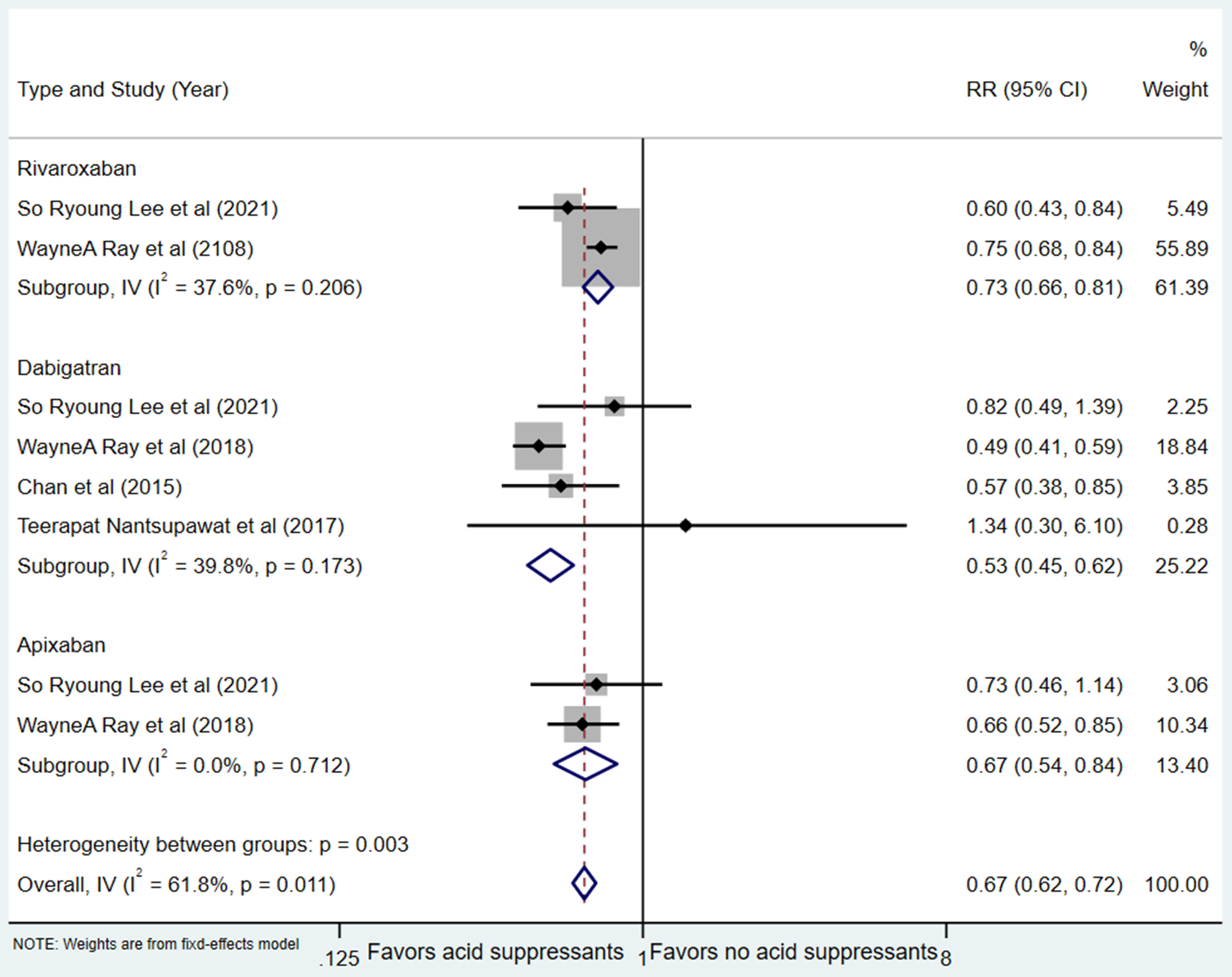
Forrest plot for subgroup analysis based on the types of NOACs (fixed-effects model) RR: risk ratio; CI: confidence interval.
Discussion
Antithrombotic drugs are the cornerstone of embolism-prone diseases (such as non-valvular atrial fibrillation, pulmonary embolism, arteriovenous embolism, etc) to prevent thrombosis and embolic complications. Generally, NOACs are more effective and safer than warfarin.,217 However, it cannot be ignored that GIB was more common in patients taking NOACs than in those taking warfarin.4–6 Classical acid-inhibitory drugs, such as H2RAs and PPIs, are often used in combination with antiplatelet drug therapy, to reduce gastrointestinal complications, such as peptic ulcers and bleeding. 18 A recent meta-analysis based on pharmacodynamics and pharmacokinetics suggested the protective effect of PPIs against warfarin-related GIB. 19 However, the effect of acid suppressants on NOACs-related GIB has not been systemically reviewed.
In this meta-analysis, which included six retrospective cohort studies, we observed that the combination of acid suppressants was associated with a significantly reduced risk of GIB in patients treated with NOACs. The RR calculated according to the number of events is insignificant, because the included studies mostly use HR as the statistical indicator of outcome, which takes into account the time when the outcome occurs. Therefore, we speculate that the effect of acid suppressants on reducing NOACs-related GIB requires a certain period of time. Most patients who used NOACs had indications for non-valvular atrial fibrillation, which often requires long-term anticoagulant therapy. Whether PPIs would increase cardiovascular events is still controversial. 20 Therefore, it is crucial to balance the risk-benefit value before the co-prescription of NOACs and acid suppressants. After excluding the Lauffenburger et al. study, the heterogeneity of the combined results was significantly reduced. The sources of heterogeneity came from three aspects: First, the indication for the included patients to use dabigatran was only if they had non-valvular atrial fibrillation. Second, unlike the other five studies, which were divided into groups who used acid suppressants and those without acid suppressants, Lauffenburger et al.’s study was divided into the bleeding and non-bleeding groups, and acid suppressants were only a covariate (although HR could still be calculated). Third, the follow-up time of the cohort was too short (the end time of the study was December 31, 2012; however, the US FDA approved the use of dabigatran on October 19, 2010).
In the subgroup analysis of the source of GIB, we further confirmed the protective effect of acid inhibitors on UGIB. Notably, bleeding events from the lower gastrointestinal tract are more common than UGIB in patients receiving NOACs, representing one-third and one-half of bleeding events under Xa (rivaroxaban, apixaban, and edoxaban) and direct thrombin (dabigatran) inhibitors respectively. 21 Interestingly, most of lower GIB were mild bleeding that usually did not require medical intervention. 22 Therefore, internists introduced the concept of “major gastrointestinal bleeding (MGIB)” according to International Society on Thrombosis and Haemostasias criteria, 23 which is defined as symptomatic bleeding (eg, hematemesis, and melena) with GI tract lesions confirmed by endoscopy, radiology, pathology reports, surgery, autopsy, or occult bleeding from GI tract resulting in ≥2 g/dl reduction in hemoglobin or requiring transfuse red blood cells ≥2 units or surgical intervention. 24 Because patients with MGIB patients are mostly elderly and have many complications, the risk of emergency endoscopy or surgical intervention is very high. Therefore, identifying and managing MGIB as early as possible is still a topic to be further studied.
In the subgroup based on NOACs categories, we found that the largest reduction in GIB risk was noted in dabigatran with acid suppressant co-therapy. One hypothesis may be related to the reduction of dabigatran plasma levels by acid suppressants. Two recent studies have reported that pantoprazole and omeprazole can significantly reduce the trough and peak plasma levels of dabigatran.25,26 However, another study implicated that concomitant PPIs did not affect the anti-Xa bioactivity of apixaban and rivaroxaban. 27 Another hypothesis may be that the tartaric acid core of dabigatran requires a lower pH (<4) for absorption, and the combination of PPI reduces the absorption and availability of dabigatran. 28 Dabigatran etexilate and tartaric acid core are the two primary components of dabigatran. Tartaric acid provides the necessary acidic environment for the absorption of dabigatran etexilate, whereas dabigatran etexilate is an inactive prodrug that needs to be converted into its active form by esterase (existing in the liver, plasma, and bile acid). 29 The unabsorbed dabigatran etexilate is transformed into an active form through liver and bile acid metabolism. It accumulates locally in the intestine; therefore, it has a relatively higher ratio of lower GIB.30,31 PPI only affected the absorption of dabigatran, but did not affect this process, which may be the reason why we found that the protective effect was significant in the upper gastrointestinal tract. Among Xa factor inhibitors, the bleeding risk of rivaroxaban with acid suppressant co-therapy is higher than that of apixaban. This result is consistent with the latest cohort study of Asian patients with atrial fibrillation that all on concomitant NOACs and PPI. 32 The risk reduction of UGIB in apixaban (HR: 0.69; 95% CI: 0.51-0.93; P = 0.014) was larger than that in rivaroxaban (HR: 0.86; 95% CI: 0.69-1.06; P = 0.145). This may be due to the fact that rivaroxaban has a higher rate of GIB th.an apixaban in patients on NOACs and without acid suppressant co-therapy. Previous studies (post-marketing trials, real-world studies, and meta-analyses) have demonstrated that rivaroxaban had the highest risk of GIB among NOACs.33–35 In addition, the tartaric acid core of dabigatran that may cause more gastrointestinal symptoms (eg, dyspepsia and, abdominal pain), PPIs are recommended to relieve gastrointestinal symptoms in 2020 ESC Guidelines. 1 Whether acid suppressants will affect the anticoagulant effect of NOACs remains unclear. None of the studies included in our meta-analysis compared the rates of re-embolism and stroke between the acid and non-acid suppressants group. Meanwhile the aforementioned study by Bolek et al. failed to compare the clinical effects of PPI on NOACs due to the limited number of patients (n = 31). 26 In a large-scale observational study of patients with nonvalvular atrial fibrillation on OAC and PPI co-therapy, no significant difference in stroke incidence among the individual NOACs was observed. When compared to warfarin, the risk of death in dabigatran (HR: 0.79; 95% CI: 0.68-0.92; P = 0.002) was more reduced than that of rivaroxaban (HR: 0.86; 95% CI: 0.69-1.06; P = 0.145). 32 Therefore, from the perspective of preventing GIB, dabigatran combined with acid suppressants seems to be the preferred choice.
Due to the lack of data on H2RA, we could not conduct a subgroup analysis based on the types of acid suppressants. In our search, no study directly explored the association between H2RA and NOACs for the outcome of GIB. The efficacy of acid suppressants in preventing gastroduodenal lesions caused by non-steroidal anti-inflammatory drugs (NSAIDs) or aspirin has been demonstrated to a large extent. In the 2020 Japan Clinical Guidelines For Drug-Related Peptic Ulcer, the protective effect of PPIs is better than that of H2RAs, and low-dose PPIs are remain the first-choice drugs to prevent drug-related ulcers and bleeding (eg, dual antiplatelet therapy and, NSAIDs). However, the level of evidence and strength of recommendation are low and weak for PPI co-prescription to prevent NOACs related UGIB. 36 Current guidelines recommend high-risk patients who are receiving NOACs to take PPIs to reduce the risk of GIB. The risk factors for GIB are: (1) age >75 years; (2) previous peptic ulcer disease; (3) a history of GIB; (4) concomitant use of aspirin, NSAIDs, antiplatelets or COX-2 inhibitor.36,37 In contrast to NSAIDs or aspirin, NOACs do not seem to cause gastric ulcer. One study reported that NOACs caused mucosal injury, using the modified LANZA score to evaluate gastric mucosal injury by endoscopy in subjects receiving NOACs with or without PPI co-therapy. PPI had a protective effect on the gastric mucosa of patients taking NOACs, especially in the case of taking apixaban. 38 Therefore, we propose that PPI may reduce the risk of NOACs-related GIB by reducing the damage caused by NOACs to the gastric mucosa.
This study has some limitations. First, our data analysis included a relatively small number of retrospective studies, so our conclusions are not sufficiently solid. These findings need to be verified by more prospective studies. Second, there is no detailed data on the concomitant use of acid suppressants, such as the category, dose, and duration of acid suppressants. Third, the included studies did not specifically report the effect of acid suppressants on the rate of lower GIB, although lower GIB is more common than upper GIB in patients receiving NOACs. Fourth, no included studies compared the incidence of embolic events with and without suppressant co-therapy. Whether acid suppressant co-therapy will minor therapeutic effects on NOACs is still unclear. The mortality and therapeutic difficulty of NOACs patients with related GIB are generally lower than those of related embolism diseases; Thus treatment should be guided by drug efficacy consideration over risk of GIB.
In conclusion, acid suppressants could decrease the risk of GIB, especially UGIB, in patients with NOACs. These drugs are more effective in reducing the risk of dabigatran for GIB than Xa factor inhibitors (rivaroxaban and apixaban). More RCTs are warranted to confirm the efficacy and the mechanism that how acid suppressants reduce the risk of GIB in patients treated with NOACs.
Supplemental Material
sj-docx-1-cath-10.1177_10760296211064897 - Supplemental material for Prevention of nNon-Vitamin K Oral Anticoagulants-Related Gastrointestinal Bleeding With Acid Suppressants: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cath-10.1177_10760296211064897 for Prevention of nNon-Vitamin K Oral Anticoagulants-Related Gastrointestinal Bleeding With Acid Suppressants: A Systematic Review and Meta-Analysis by Yongqi Dong, Song He, Xue Li and Zhihang Zhou in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Funding
This study was funded by the National Natural Science Fund (No. 81972285), Kuanren Talents Program of the Second Affiliated Hospital of Chongqing Medical University (13-002-011, 13-004-009).
Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contribution:
DYQ, LX contributed to study idea and design, drafting of the manuscript and data analysis; DYQ, LX, ZZH were involved in literature search and acquisition of data; ZZH, HS contributed to critical revision of the manuscript; HS is the guarantor of article. All authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Fund (No. 81972285) and Kuanren Talents Program of the Second Affiliated Hospital of Chongqing Medical University (13-002-011, 13-004-009).
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.