
Abstract
Introduction
Coronary atherosclerotic heart disease (CAHD) and chronic kidney disease (CKD) are risk factors for each other.1 CKD patients are more easily complicated with CAHD,2 for example, more than 50% of patients with severe CKD are complicated with CAHD. Meanwhile the proportion of life risk due to CAHD is significantly higher than the aggravation and progression of CKD itself,2 elderly CKD patients are 5-10 times more likely to die of cardiovascular disease than to develop end-stage renal disease (ESRD). In addition to the traditional risk factors of atherosclerosis, patients with CAHD and CKD are also exposed to uremia related risk factors such as inflammation, oxidative stress, calcium and phosphorus metabolism disorder. Due to the severity and complexity of coronary artery disease, the drug treatment of CAHD patients with CKD was affected by renal function to varying degrees, which caused restrictions and obstacles to the treatment, especially after coronary intervention, and the overall prognosis was poor. Especially in elderly patients, age is an established risk factor for both CKD and CAHD patients, and the proportion of patients with CKD and CAHD is higher in the elderly population. Therefore, it is of clinical significance to understand the clinical features and risk factors for cardiac death of elderly and severe CKD patients with CAHD after percutaneous coronary intervention (PCI).
Methods
Patient Selection
This was a retrospective analysis of patients hospitalized in Beijing Anzhen Hospital from January 1, 2008, to December 31, 2017. A total of 1010 CAHD-CKD patients over 60 years of age who had CKD stage 3 or above and underwent percutaneous coronary intervention (PCI) as a revascularization method. Hydration therapy was performed 12 h before PCI to 24 h after PCI, and 0.9% sodium chloride 0.5-1 ml/kg.h was injected intravenously. All the patients were followed up for at least 3 years. The medical records of patients included in the study were counted and analyzed. The inclusion criteria were: patient over 60 years old had CKD stage 3 or above and underwent PCI. The exclusion criteria were: Non-Asian, under 60 years of age, CKD stage 1 or 2, acute renal injury or recovery of renal function, infectious diseases, malignant tumors, severe heart diseases (eg, aortic dissection and hypertrophic cardiomyopathy), severe systemic disease, systemic inflammatory disorders, glucocorticosteroid therapies within 2 months, failed PCI or change to coronary artery bypass grafting (CABG). PCI was defined as balloon dilatation and drug-eluting stent implantation after coronary angiography. And “failed PCI” was defined as failure to stent implantation and balloon dilation, or percutaneous coronary balloon dilation only. The flowchart outlining the study is shown in Figure 1.

Flow chart of patient selection. PCI, percutaneous coronary intervention; CKD, chronic kidney disease; PTCA, percutaneous transluminal coronary angioplasty; CABG, coronary artery bypass grafting.
Definition of CKD
Patients with a history of above-normal creatinine for at least 3 months or with a definite diagnosis of CKD were included, except for those with a gradual decline in creatinine levels that returned to normal during hospitalization. The estimated glomerular filtration rate (eGFR) was calculated by the Cockcroft-Gault Formula 18 [(140-age)*body weight (kg)/serum creatinine (mg/dL)*72] (*0.85 in women). Participants with eGFR<60 (ml/min.1.73 m2) were defined as CKD stage 3 according to the classification of the National Kidney Foundation.
Data Extraction and Quality Assessment
Clinical data were collected on patients’ general status, such as age, sex, height, and weight, family history of coronary heart disease, and risk factors or complications of atherosclerosis, such as hypertension, diabetes, dyslipidemia, cerebral infarction, and history of lower extremity arteriosclerosis obliterans (LEASO) defined as patient had symptoms of intermittent claudication or resting pain in the lower limbs, and the arterial pulse of the lower limb arteries was weakened or no pulse. Lower extremity arterial ultrasound showed that the blood flow signal weakened or disappeared, and ankle brachial index (ABI) was <0.8. History of revascularization defined as previous PCI or CABG. Acute kidney injury (AKI) defined as serum creatinine was 25% higher than baseline or the absolute value was higher than 44 umol/L within 48 hours after coronary angiography. Important laboratory examinations during hospitalization mainly included routine blood examination, liver and kidney function, blood lipid level, ion detection, coronary artery impact data and information about interventional diagnosis and treatment, including lesion characteristics, PCI target vessels, dosage of contrast agent and postoperative effect. An Excel database was established, collating these data. The situation and time of cardiac death were recorded with telephone follow-up as the main form, supplemented by the inquiries of outpatient and inpatient medical records in Anzhen Hospital.
Statistical Analysis
All data were statistically analyzed using SPSS 26.0 for Windows (IBM Corp.), Stata 15.0 (Stata Corp.) All continuous variables were tested for normality using the Kolmogorov–Smirnov method. Normally distributed continuous variables are expressed as the mean ± standard deviation, nonnormally distributed variables are expressed as the median and interquartile range, and categorical variables are expressed as the number and percentage. Statistical significance was defined as P < .05 with two-sided tests. The patients were divided into groups according to whether they died or not and whether there were differences between the two groups. The measurement data with a normal distribution were compared between the two groups by Student's t-test, the measurement data with a skewed distribution were compared by the Mann–Whitney U-test, and the qualitative data were compared by the chi-square test and Fisher's exact test. After univariate analysis of all variables, the variables with P < .2 were selected for further logistic regression, and the forward LR method was used to gradually fit the model. Both were bilateral tests, and at P ≤ .05, the difference was considered statistically significant.
Results
Different Clinical Features Between the two Groups
A total of 1010 patients with CAHD-CKD met the study criteria, and 142 patients had cardiac during at least 3–12 years of follow-up. The two groups were compared with age, sex, body mass index (BMI), length of stay, renal function, family history, smoking history, history of revascularization, contrast media dosage, AKI proportion of patients with hypertension, diabetes, blood lipid abnormalities, heart failure and cerebral infarction, heart rate and Grace score at admission, and none were significantly different. There were no differences in leukocyte count, erythrocyte count, platelet count, liver function, uric acid and blood lipids, myocardial enzymes and ions, double antiplatelet drug treatment and perioperative use of parenteral anticoagulants and IIbIIIa receptor antagonists, beta-blockers, renin-angiotensin-aldosterone system inhibitors (RAASI) calcium channel blockers (CCBs) and nitrates, coronary artery lesion characteristics or surgical approach.
The proportions of patients with systolic blood pressure <90 mmHg and diastolic blood pressure <60 mmHg at admission were higher (5 [3.50%] vs 11 [1.30%]) and (9 [6.30%] vs 27 [3.10%]), the proportion of patients with lower extremity arteriosclerosis obliterans (LEASO) was increased (11 [7.70%] vs 29 [3.30%]), and the proportion of patients receiving single-vessel interventional therapy was decreased (94 [66.20%] vs 656 [75.60%]) in the mortality group compared with the nonmortality group. The above differences were statistically significant (P < .05) (Table 1).
Characteristics and Therapies in the Different Treatment Groups

Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; BMI, body mass index; PFH, positive family history; SAP, stable angina pectoris; UAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; OMI, old myocardial infarction; HF, heart failure; LEASO, lower extremity arteriosclerosis obliterans; CKD, chronic kidney disease; TFI, transfemoral intervention; SVD, single-vessel disease; DVD, double-vessel disease; TVD, three-vessel disease; AKI, acute kidney injury; CCC, coronary collateral circulation; CTO, chronic total occlusion; PCI, percutaneous coronary intervention; LM, left main; LVEF, left ventricular ejection fraction; RAASI, renin-angiotensin-aldosterone system inhibitors; LMWH, low-molecular-weight heparin; CCB, calcium channel blocker; PPI, proton pump inhibitors; ICA, isotonic contrast agent; WBC, white blood cell; RBC, red blood cell; PLT, platelets; UA, uric acid; eGFR, estimate glomerular filtration rate; CK, creatine kinase; CK-MB, creatine kinase isoenzymes; TG, triglyceride; TCH total cholesterol; HDLC, high-density lipoprotein cholesterol; LDLC, low-density lipoprotein cholesterol; AST, aspartate aminotransferase; ALT, alanine aminotransferase; TP, total protein.
Logistic Regression of Cardiac Death
The variables with P < .2 that could be included in logistic regression were systolic blood pressure (SBP) < 90 mmHg, diastolic blood pressure (DBP)<60 mmHg, revascularization history, smoking history, stable angina pectoris (SAP), ST-segment elevation myocardial infarction (STEMI), LWASO, transfemoral intervention (TFI), single-vessel disease percutaneous coronary intervention (SVD PCI), no statins, white blood cells (WBCs), and serum potassium (K). The continuous variables WBC and K were converted into binary variables according to the cutoff value (the cutoff value of WBC is 6.555 × 109/L, the cutoff value of K is 4.285 mmol/L) and were included in the regression model. SVD PCI (OR = 0.612, 95% CI: 0.416-0.899, P = .012) was a protective factor against cardiac death. SAP(OR = 4.723, 95%CI: 1.098∼20.322, P = .037), combined with LWASO (OR = 2.631, 95%CI: 1.272∼5.440, P = .009), K > 4.285 mmol/L(OR = 1.44, 95%CI: 1.002∼2.069, P = .049), and without statins (OR = 2.015, 95%CI: 1.072∼3.789, P = .030) were risk factors for cardiac death (Table 2 and Figure 2).

Multivariate logistic regression of cardiac death. OR, odds ratio; CI, confidence interval; SVPCI, single-vessel percutaneous coronary intervention; SAP, stable angina pectoris; LEASO, lower extremity arteriosclerosis obliterans.
Multivariate Logistic Regression of Cardiac Death.
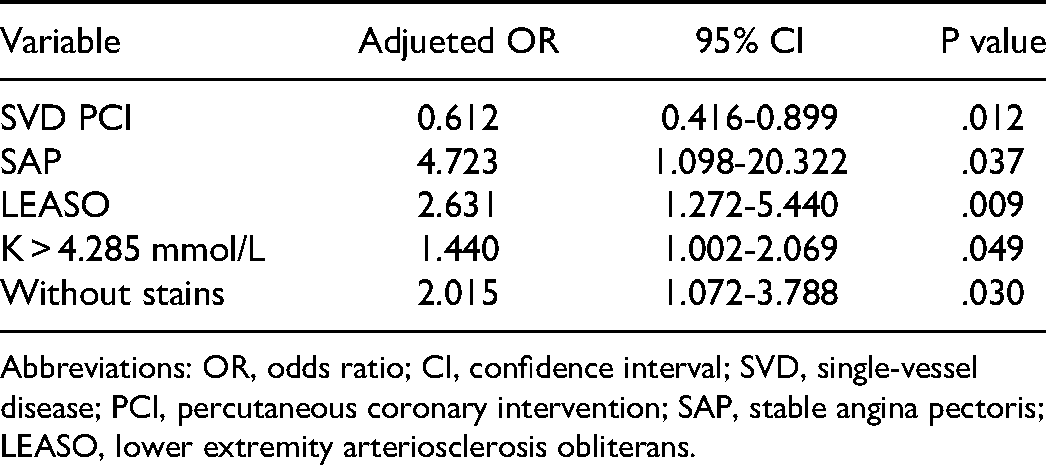
Abbreviations: OR, odds ratio; CI, confidence interval; SVD, single-vessel disease; PCI, percutaneous coronary intervention; SAP, stable angina pectoris; LEASO, lower extremity arteriosclerosis obliterans.
Discussion
Patients with renal dysfunction are more prone to cardiovascular disease (CVD), high mortality and poor prognosis.3 CVD is a major cause of morbidity and mortality in patients with CKD.4 To date, all randomized controlled studies on myocardial revascularization have excluded CKD patients; therefore, revascularization therapy with CKD is currently based on observational studies.5 Current retrospective studies have shown that CKD patients have better survival after revascularization than drug therapy.6,7 A large amount of registration data shows that inpatient revascularization is associated with improved survival regardless of the estimated glomerular filtration rate (eGFR).8 PCI was superior to CABG in short-term all-cause death and cerebrovascular accident rates.2,9 However, some studies have shown that the restenosis rate after PCI in ESRD patients is almost twice that of patients with normal renal function.10 Cardiovascular event (CV) risk and mortality are inversely proportional to eGFR,8 but the eGFR level that begins to increase the risk is not clearly defined.10,11 Elderly individuals are more likely to be complicated with CAHD and CKD. Therefore, it is of great practical significance to systematically analyze the clinical characteristics of elderly patients with severe CKD under PCI treatment and to establish a multifactor risk prediction model to improve the identification and management of patients with poor prognosis, PCI treatment strategies and the clinical prognosis of these patients.
Currently, it is believed that patients with CKD stage 3 and above receiving invasive strategies do not experience reduced end events,12 but in the real world, a large number of patients with CKD still need revascularization therapy, which is driven by severe ischemic events. In this study, PCI did not reduce the risk of cardiac death in CKD patients with stable angina. This conclusion was also confirmed by the results of ischemia-CKD clinical trials.13–15 Among patients with stable coronary disease, advanced chronic kidney disease, and moderate or severe ischemia, the Ischemia-CKD Clinical Trials did not provide evidence that the initial invasive strategy, in contrast to a conservative strategy with maximal medical management,13 reduced the risk of death, myocardial infarction or nonfatal myocardial infarction14 and relieved angina symptoms.15
A study16 including 453 573 subjects showed that LEASO is more common in patients with CKD and is related to lower extremity complications and mortality. CKD is more interrelated with wide vascular disease compared with the general population. Patients with both conditions had lower survival rates.17 Some studies17,18 have suggested that CKD patients with albuminuria have decreased GFR, inflammatory conditions, and calcium and phosphate metabolism disorders that cause systemic vascular damage. Therefore, a number of authors considered CKD to be a risk factor for vascular disease. Currently, the great majority of organizations suggest the detection of LEASO in CKD patients. A recent study supports this suggestion because the results showed that a low ABI was a predictor of organ failure and death.19 In addition, we cannot ignore that LEASO is a significant symbol of severe systemic atherosclerosis and is strongly associated with poor prognosis.20
CKD patients are liable to electrolyte disturbance, which is related to poor prognosis. For CKD patients, both hypo- and hyperkalemia can have direct harmful physiological effects. Some meta-analyses21 show that the U-shaped curve corresponds to the relationship between potassium levels and the risk of adverse outcomes, with the lowest risk at serum potassium levels of 4–4.5 mmol/L. In our study, the results also confirm this conclusion. Hyperkalemia leads to poor prognosis in patients with CAHD, which may be due to arrhythmia, influence on the use of ACEIs or ARBs, etc.22,23
In actual clinical work, the proportion of CKD patients receiving reperfusion or revascularization treatment is significantly reduced; therefore, the proportion of CKD patients receiving aspirin, clopidogrel, statins, ACEIs or ARBs and β-blockers is significantly lower than that of patients with normal renal function. Some studies24 suggest that statins have a poor effect in reducing cardiovascular complications in CKD patients, and statins are not recommended for dialysis patients. However, in other studies,25 when the indication was extended to all CKD patients, the authors concluded that atorvastatin therapy significantly reduced the relative risk of major outcomes in CKD patients. Focused atorvastatin therapy reduces the cardiovascular risk for CKD patients in the real world compared with conventional treatment, and there is no significant difference in treatment effects between patients with and without CKD. In addition, the eGFR did not decrease in patients treated with atorvastatin during the study period.
SVD PCI was a protective factor against cardiac death and may be related to mild CAHD and nonsevere and complex vascular disease. SVD PCI can control the dosage of contrast medium and avoid the aggravation of renal function damage or AKI.
CAHD is very common in CKD. CKD alters the traditional risk factors for atherosclerosis, and CKD has some unique mechanisms, such as inflammation and changes in mineral metabolism, playing a major pathophysiological role in the decline of renal function.26 Therefore, it is of great significance for clinical work to understand the prognostic risk factors for patients with severe CKD complicated with CAD.
Limitation
The limitations of this study are mainly reflected in the single-center retrospective study, which may have certain selection bias. Second, due to the study enrollment group is relatively rare and the enrollment time is long, there are great developments and changes in coronary intervention technology during this period. Third, prospective multicenter studies are needed to further verify the results.
Conclusions
In elderly and serious CAHD-CKD patients after PCI, SVD PCI was a protective factor against cardiac death. However, SAP, CAHD-CKD combined with LEASO, K > 4.285 mmol/L, and no statins were independent risk factors of cardiac death for elderly patients with severe CKD after PCI.
Footnotes
Author Contributions
YZ and JLW contributed to the conception or design of the work. GYZ contributed to the acquisition, analysis, orinterpretation of data for the work. YZ drafted the manuscript. YJZ critically revised the manuscript. All gave final approval and agreeto be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Municipal Administration of Hospitals’ Mission Plan, Beijing Municipal Administration of Hospitals’ Ascent Plan, National Key Research and Development Program of China, (grant number SML20180601, DFL20150601, 2017YFC0908800).
Ethical Approval
This study was approved by the Ethics Committee of Beijing Anzhen Hospital.
Informed Consent
The requirement for informed consent was obtained for this study by follow-up