
Abstract
Patients with stage 5 chronic kidney disease (CKD5D) have a higher risk of developing neurocognitive deficits. Stroke, cervical carotid artery disease (CCAD), and intracranial atherosclerotic disease (ICAD) are causes of such deficits in CKD5D. Chronic inflammation from renal failure elevates risk for these diseases through oxidative stress and vascular dysfunction. The adverse impact on the carotid and intracranial vasculatures contributes to the multifactorial pathophysiology of stroke. Eleven plasma biomarker levels in patients with CKD5D (n = 97) and healthy controls (n = 17-50) were measured using sandwich enzyme-linked immunosorbent assay (ELISA) method. Of the 97 patients with CKD5D, 24 had CCAD, 19 had ICAD, and 23 had acute stroke. Elevations in NACHT, LRR, and PYD domains-containing protein 3 (NALP3) levels in patients with CKD5D (+)CCAD (1.80 ± 0.11 ng/mL) compared to patients with (−)CCAD (1.55 ± 0.08 ng/mL) were statistically significant (P = .0299). Differences in D-dimer levels were also found to be statistically significant (P = .0258) between CKD5D (+)stroke (1.83 ± 0.42 μg/mL) and (−)stroke (0.89 ± 0.13 μg/mL) groups. The ages of the (+) neurovascular disease groups were found to be significantly elevated compared to the (−) neurovascular disease groups (P = .0002 carotid AD; P < .0001 ICAD; P = .0157 stroke). D-dimer levels were positively correlated with age in CKD5D (P = .0375). With the possible exception of NALP3 for CCAD, profiling levels of specific biomarkers for risk stratification of neurovascular diseases in the CKD5D population warrants further investigation.
Keywords
Introduction
Patients with stage 5 chronic kidney disease (CKD5D) have a higher risk of developing neurocognitive deficits. 1 Such deficits depend on the location of affliction in the central nervous system and can include impairments in executive function and motor skills, as well as alterations in attention and perception. 2 Stroke, along with other impairments of the cerebrovascular system such as cervical carotid artery disease (CCAD) and intracranial atherosclerotic disease (ICAD), are major causes of neurocognitive deficits in the CKD5D population. 3 According to the National Institute of Diabetes and Digestive and Kidney Diseases, 5.4% of the deaths in patients with CKD5D from 2012 to 2014 were caused by stroke alone. Previous studies have shown that stroke risk in the CKD5D population ranges from 5 to 11 times that of the general population. 4,5 Chronic kidney disease, often presenting with comorbid diabetes and hypertension, imminently leads to increased stroke risk through decreased toxin filtration, vascular dysfunction, and arterial calcification. 6 Upregulated inflammation and oxidative stress caused by CKD5D adversely impacts the carotid and intracranial vasculatures, ultimately contributing to the multifactorial pathophysiology of stroke in the CKD5D population. 7 Blood plasma biomarkers have played a critical role in multiple disease processes. Cardiac troponins for myocardial infarctions and cystatin C for renal dysfunctions are a few examples where plasma biomarkers have aided clinicians in diagnosis and prognosis. 8,9 As the role of biomarkers on neurological outcomes in patients with CKD5D is not yet known, measuring biomarker levels in these patients may be clinically beneficial for risk stratifications of stroke, CCAD, and ICAD in the CKD5D population.
We sought to evaluate the role of 11 commercially available biomarkers of hemostasis and thrombosis on the progression of vascular dysfunction in the CKD5D population. Angiopoietin-1 (Ang-1) and angiopoietin-2 (Ang-2) are known for their modulation of the vascular system through inflammation, permeability, and remodeling. 10 Soluble CD40 ligand (CD40L) plays a significant role in hemostasis, thrombosis, and the upregulation of various endothelial mediators. 11 C-reactive protein (CRP) and D-dimer are both well-characterized molecules with the former being an acute phase reactant and the latter a product of fibrinolysis. Both are relevant to inflammatory processes and thrombosis. 12 Intercellular adhesion molecule-1 (ICAM-1) is a member of a class of endothelial adhesion molecules known to participate in atherosclerosis. 13 NACHT, LRR, and PYD domains-containing protein 3 (NALP3), also known as cryopyrin, are integral components of inflammasomes, the presence of which leads to the formation of interleukin-1β and interleukin-18 levels, and subsequently atherosclerosis. 14 Elevated levels of plasminogen activator inhibitor-1 (PAI-1) has been correlated with obstructive atherosclerotic coronary artery disease. 15 Procalcitonin (PCT) is a useful biomarker for septic shock both in terms of diagnosis and prognosis, and thus its measurement could prove useful for patients with CKD5D where vascular inflammation via infective etiologies are common. 16,17 Tumor necrosis factor-alpha (TNF-α) is another well-characterized acute phase reactant, while von Willebrand factor (vWF) has an established role in thrombosis. Measuring and analyzing these biomarkers may thus contribute to our understanding of the pathogenesis of the cerebrorenal axis in patients with CKD5D.
Methods and Materials
Predialysis blood samples from 97 patients with CKD5D (aged 19-87 years, mean 60) treated at the Loyola Outpatient Dialysis Center were collected in 3.2% (0.109 mol/L) sodium citrate tubes during March and April 2017. Samples were centrifuged at 1100 × g for 15 minutes, within 2 hours of venous sampling. Each resulting plasma was then divided into 10 aliquots of 100 μL plasma, which were then frozen at −80°C for later analysis. Plasma samples from 25 male and 25 female, nonsmoking, drug-free healthy volunteers (aged 19-54 years, mean 33) were purchased as controls from George King Bio-medical, Inc (Overland Park, Kansas). The use of healthy controls would serve to elucidate normal levels of circulating blood biomarkers, as well as confirm the relative elevation of these levels in patients with CKD5D.
Stage 5 chronic kidney disease and control plasma samples were used to profile levels of biomarkers of inflammation and hemostatic dysregulation. Biomarkers measured in this study included Ang-1, Ang-2, CD40L, CRP, D-dimer, ICAM-1, NALP3, PAI-1, PCT, TNF-α, and vWF. Biomarker levels were measured using commercially available sandwich ELISA kits (CRP, D-dimer, PAI-1, and vWF – Hyphen Biomed, Neuville-sur-Oise, France; Ang-1, Ang-2, CD40L, ICAM-1, and TNF-α – R&D Systems, Inc, Minneapolis, MN; NALP3 – LifeSpan BioSciences, Inc., Seattle, Washington). Reagents, standards, and sample solutions were thawed, diluted, and prepared according to respective ELISA manufacturer’s specifics.
Patient demographic data (age, sex, and diagnoses) and comorbid conditions were extracted from electronic medical record. Any documentation of CCAD (n = 24), ICAD (n = 19), and acute stroke (n = 23) for each patient was noted. It should be noted that of the 63 patients without any documentations of intracranial or extracranial vascular disease, 9 had vascular imaging confirming so. Given the patient sample size for this study, acute stroke encompasses both hemorrhagic and ischemic subtypes. Biomarker and demographic data were collected in Microsoft Excel and analyzed using GraphPad Prism 7. Mean ± standard error of the mean was used as the standard expression for the quantitative results. Comparisons were performed using Mann-Whitney t tests and Kruskal-Wallis nonparametric analysis of variance. Nonparametric Spearman was used for correlations. P values less than .05 were considered statistically significant.
The study was approved by the institutional review board at Loyola University Medical Center.
Results
Comparing CKD5D versus Healthy Controls
Patients with CKD5D had significant elevations in plasma concentration of every inflammatory and hemostatic biomarker compared to healthy controls (P = .0002 CRP; P = .0010 ICAM-1; P < .0001 Ang-1, Ang-2, CD40L, D-dimer, NALP3, TNFα, PCT, vWF), except for PAI-I (Table 1). The ratio of Ang-1 to Ang-2 was found to be lower among the CKD5D cohort (0.08 ± 0.01) compared to healthy controls (0.11 ± 0.08) and the difference was statistically significant (P < .0001). Both patients with CKD5D and healthy control samples exhibited weak positive correlations between vWF levels and age and between CD40L and Ang-1 levels (Supplemental Table S1). The healthy controls uniquely had a positive correlation between NALP3 levels and age (r = 0.4578, P = .0245), and a negative correlation between TNF-α and PCT levels (r = −0.4986, P = .0214). Plasma from the CKD5D population, by contrast, had 10 positive correlations not seen in healthy controls, the strongest of which was between CRP and Ang-2 levels (r = 0.4233, P < .0001).
Biomarker Levels Reported as Mean ± SEM for Healthy Controls (n = 17-50) and Total CK5D Patients (n = 97). P Value and Percentage Change (%Δ) Between the 2 Groups are Also Reported.
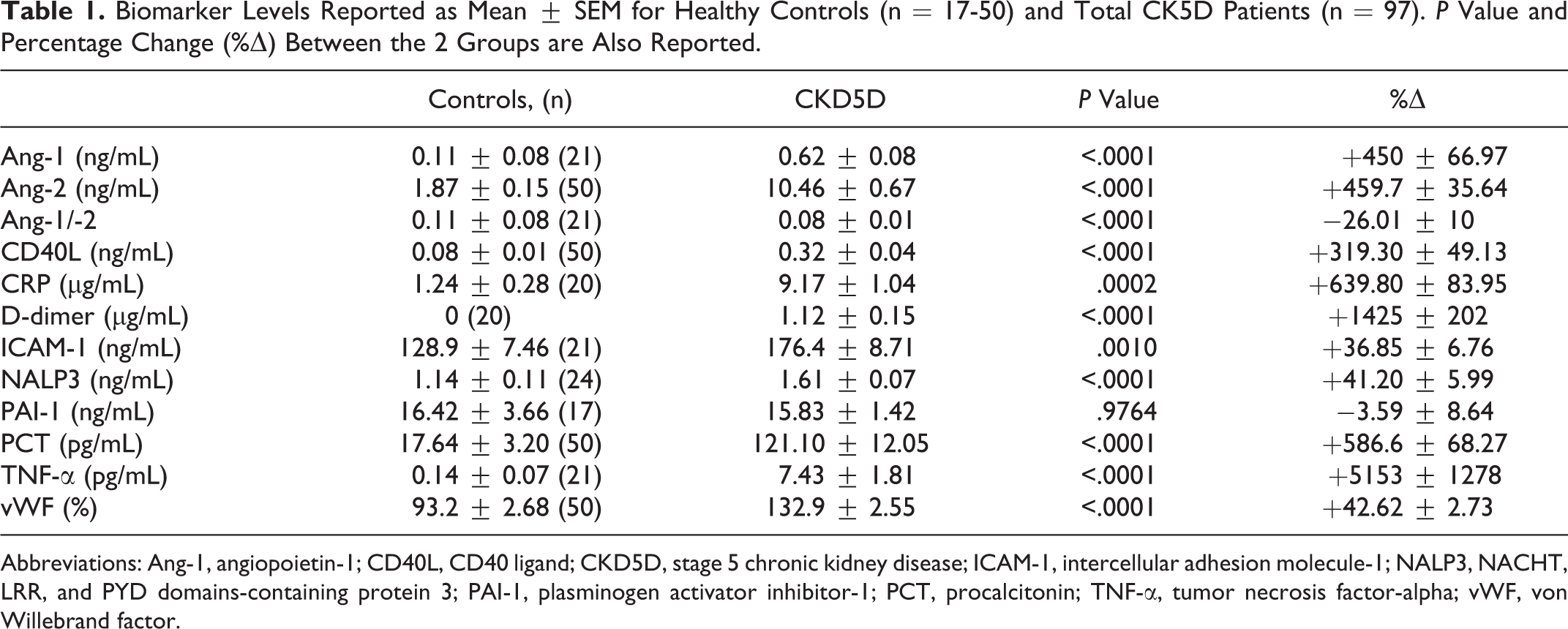
Abbreviations: Ang-1, angiopoietin-1; CD40L, CD40 ligand; CKD5D, stage 5 chronic kidney disease; ICAM-1, intercellular adhesion molecule-1; NALP3, NACHT, LRR, and PYD domains-containing protein 3; PAI-1, plasminogen activator inhibitor-1; PCT, procalcitonin; TNF-α, tumor necrosis factor-alpha; vWF, von Willebrand factor.
Comparisons Between Respective CKD5D (+) and (−) Neurovascular Disease Categories
Table 2 lists biomarkers with higher levels in CKD5D (+) neurovascular disease groups compared to their respective (−) neurovascular disease groups. Compared to patients with CKD5D (−)CCAD, those who were (+)CCAD had elevated mean levels of ICAM-1 (183.9 ± 16.3 ng/mL vs 173.9 ± 10.3 ng/mL), NALP3 (1.80 ± 0.11 ng/mL vs 1.55 ± 0.08 ng/mL), and vWF (140.5 ± 5.2% vs 130.4 ± 2.9%; Table 2). Of these comparisons, statistical significance was found between (+) and (−) CCAD NALP3 levels (P = .0299; Figure 1). Mean levels of CD40L (0.36 ± 0.09 ng/mL vs 0.31 ± 0.04 ng/mL), NALP3 (1.66 ± 0.13 ng/mL vs 1.60 ± 0.08 ng/mL), PCT (135.5 ± 36.3 pg/mL vs 117.5 ± 12.1 pg/mL), and vWF (143.3 ± 4.6% vs 130.4 ± 2.9%) were found to be increased in patients with ICAD compared to those without. However, statistical significance was not found among the levels of vascular biomarkers between the (+) and (−) ICAD patient groups. Mean levels of D-dimer (1.83 ± 0.42 μg/mL vs 0.89 ± 0.13 μg/mL), ICAM-1 (200.4 ± 16.2 ng/mL vs 168.9 ± 10.1 ng/mL), PAI-1 (19.7 ± 3.5 ng/mL vs 14.6 ± 1.5 ng/mL), and vWF (137.1 ± 4.0% vs 131.6 ± 3.1%) were found to be increased in patients with CKD5D who experienced acute stroke compared to those who did not. Statistical significance was found between the (+) and (−) stroke patients with CKD5D in terms of D-dimer levels (P = .0258; Figure 2). Further analysis of D-dimer levels revealed a weak correlation with age in the CKD5D population (r = 0.2115, P = .0375). Ages between each (+) and (−) disease groups were also found to be significantly different (P = .0002 CCAD; P < .0001 ICAD; P = .0157 stroke).
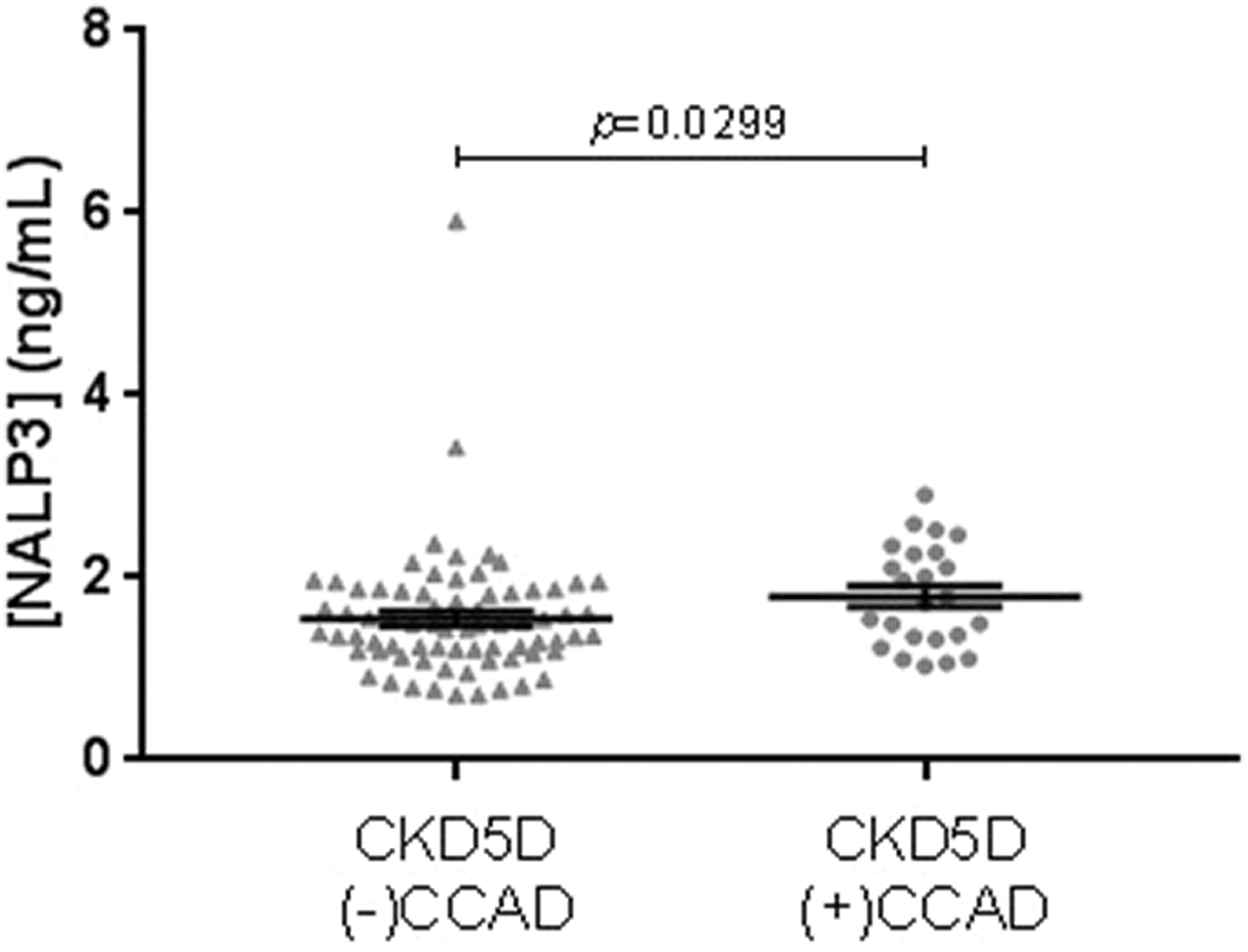
Comparison of NALP3 levels between CKD5D (−)CCAD (n = 73) and CKD5D (+)CCAD (n = 24). Mean levels were 1.55 ± 0.08 ng/mL for (−)CCAD, and 1.80 ± 0.11 ng/mL for (+)CCAD.
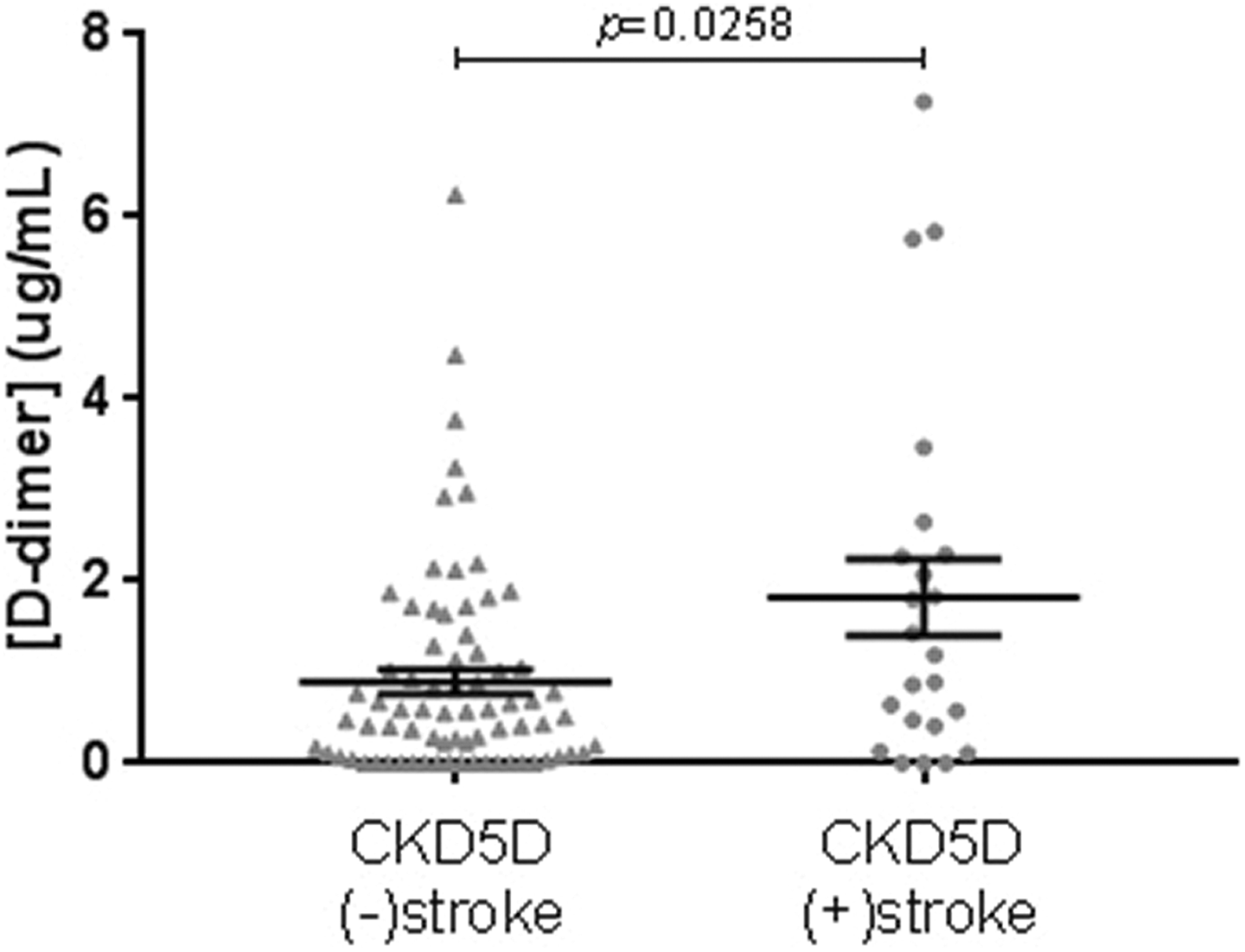
Comparison of D-dimer levels between CKD5D (−)stroke (n = 74) and CKD5D (+)stroke (n = 23). Mean Levels were 0.89 ± 0.13 μg/mL for (−)stroke, and 1.83 ± 0.42 μg/mL for (+)stroke.
Increased Levels of Biomarkers in Patients With CKD5D and Comorbid Neurovascular Disease. Levels are Reported as Mean ± SEM for each (+) and (−) Disease Groups. P Values and Average Percentage Changes (Avg. %Δ) Between Each Respective Groups are Also Reported.
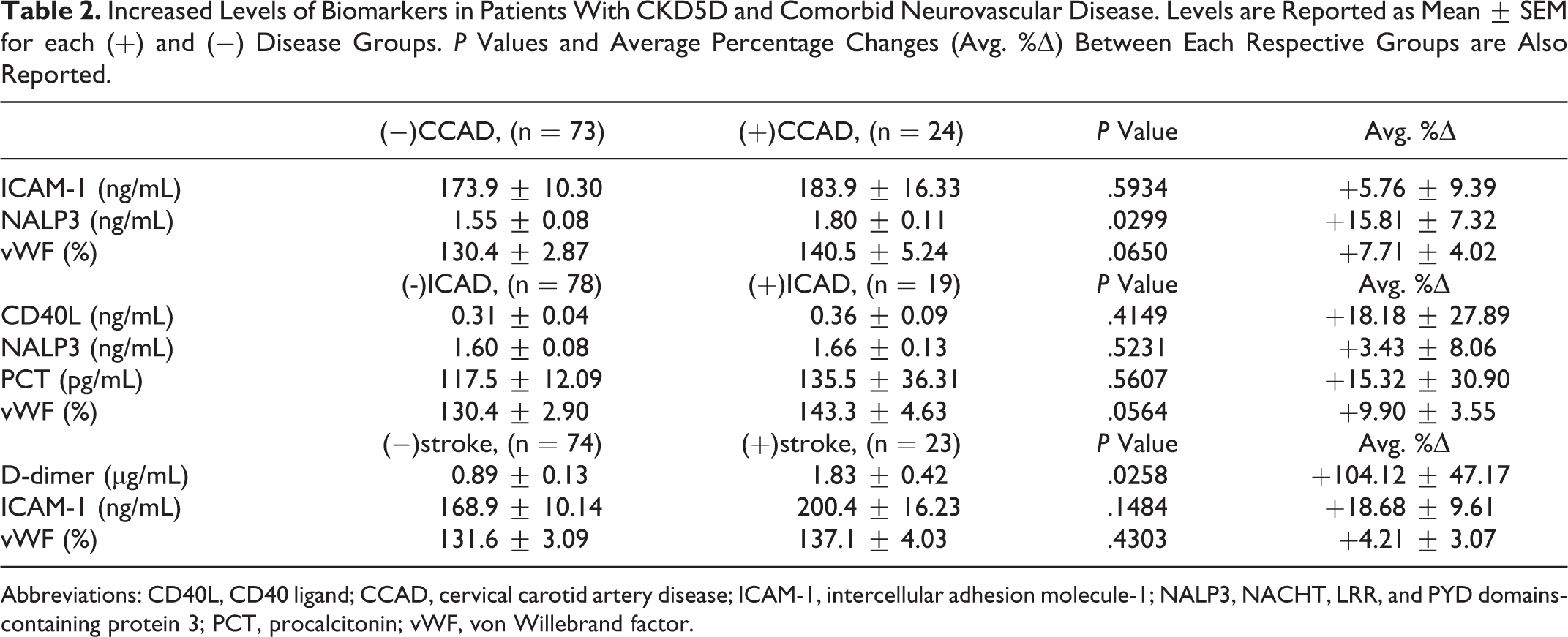
Abbreviations: CD40L, CD40 ligand; CCAD, cervical carotid artery disease; ICAM-1, intercellular adhesion molecule-1; NALP3, NACHT, LRR, and PYD domains-containing protein 3; PCT, procalcitonin; vWF, von Willebrand factor.
Top Quartile Analyses
Comparative analyses were also carried out whereby only the top quartile values of plasma biomarker levels of each neurovascular disease category were used for respective comparisons. Comparison between patients with CKD5D (−)CCAD (n = 18) and patients with (+) CCAD (n = 6) found statistically significant elevations in vWF (P = .0183) and NLRP3 (P = .0056) levels in the (+) neurovascular disease group, while those of Ang-2 (P = .0396) and CD40L (P = .0396) were decreased. Comparison between patients with CKD5D (−)ICAD (n = 19) and (+)ICAD (n = 5) only revealed a statistically significant decrease in CRP levels (P = .0240) in the (+) neurovascular disease group. Comparison between patients with CKD5D (−) stroke (n = 18) and (+)CCAD (n = 6) found a statistically significant elevation in D-dimer levels (P = .0118) in the (+) neurovascular disease group, while those of TNF-α (P = .0148) and CD40L (P = .0183) were decreased.
Discussion
Circulating levels of inflammatory and hemostatic blood biomarkers can generally be expected to be elevated in patients with renal dysfunction. 18 Presence of CKD5D confers chronic systemic inflammation via the retention and accumulation of normally excreted toxins. 19 The presentation of a patient with CKD5D can vary depending on not only the multiple locations and degrees of inflammatory damage but also the unique set of uremic toxins present, as well as their corresponding blood concentrations. 20 Vascular calcifications, derangements of bone mineralization, and cardiovascular dysfunction thus result from lingering presence of the uremic toxins. 21 Atrial fibrillation is one such cardiac disease process found to be prevalent within the CKD5D population, and this condition in itself drastically contributes to the risk of stroke via cardioembolism. Such disease processes ultimately contribute to the pathophysiology of neurovascular diseases in patients with CKD5D.
In terms of CCAD and ICAD, both are cerebrovascular diseases which may significantly contribute to the pathophysiology of acute and recurrent stroke events. 22,23 Both CCAD and ICAD share similarities extending to risk factors, pathogenesis, diagnostics, and clinical management. 22 –24 The use of surgical interventions differ, however, with aggressive medical management being preferred for ICAD, while revascularization techniques such as carotid endarterectomy and carotid angioplasty and stenting are available options for CCAD, alongside appropriate pharmacotherapy. 22,23 Additionally, literature suggests that the prevalence of the two cerebrovascular diseases differ among racial and ethnic groups, with African American patients exhibiting higher percentages of ICAD, while Hispanic and non-Hispanic white patients having higher percentages of CCAD. 25 –27 Reasons for these differences could be due to genetic susceptibility, as well as differences in lifestyle and risk factors. 22
Lack of a statistically significant difference in PAI-1 levels between patients with CKD5D and healthy controls could be due to anticoagulant mechanisms, particularly in terms of high dose administrations of unfractionated heparin prior to hemodialysis. 28 Samples for this study were collected after heparin administration. Levels of PAI-1 were expected to be elevated due to its function regarding the inhibition of fibrinolysis and its reputation as a potential biomarker for cardiovascular and atherosclerotic disease processes. 15 Although the main clinical use of heparin lies within its ability to bind antithrombin and inactivate the coagulation cascade, heparin can also bind to a variety of proteins to cause additional pharmacological effects, one of which may be the downregulation of PAI-1. 29,30 Indeed, a 2014 study by Wang et al also found a statistically significant decrease in PAI-1 levels in patients who underwent hemofiltration treatment for multiple organ dysfunction syndrome. 31
In terms of neurovascular diseases, studies have shown a connection between NALP3 expression and unstable atherosclerotic plaques in CCAD. 32 Increased levels of NALP3 has been implicated in the formation of several autoinflammatory diseases, such as familial Mediterranean fever, pyogenic arthritis pyoderma gangrenosum and acne syndrome, and hyperimmunoglobulinemia D syndrome. 33 NACHT, LRR, and PYD domains-containing protein 3, also known as cryopyrin, is an integral component of inflammasomes, the presence of which leads to the formation of interleukin-1β and interleukin-18 levels. These cytokines may be the reason for the elevated risk of carotid artery atherosclerosis, and subsequently stroke, in the patients with CKD5D population. 32
The elevated D-dimer levels found in CKD5D stroke patients could be due to increased age instead of stroke. This is consistent with literature, in which studies have also shown D-dimer levels to be progressively increased with age. 34 D-dimer levels have been found to be weakly, yet positively, correlated with age in our study, and the age of our patients with CKD5D are greater on average compared to our patients with nonstroke CKD5D. Interestingly, the same 2014 study in which Wang et al found decreases in PAI-1 levels, also found increases in D-dimer levels in all patients who underwent hemofiltration. 31 The diagnosis of deep venous thrombosis (DVT) might also provide an explanation for the elevated D-dimer levels in patients with CKD5D stroke, as higher prevalence of this disease has been noted when compared to that of the nonstroke patients (Table 3). However, it should be noted that the timing of DVT experienced by each affected patient relative to their blood draw date is not uniform throughout the cohort.
Prevalence of Various Vascular Pathologies Present Within the CKD5D Cohort and its Neurovascular Disease Subcategories.
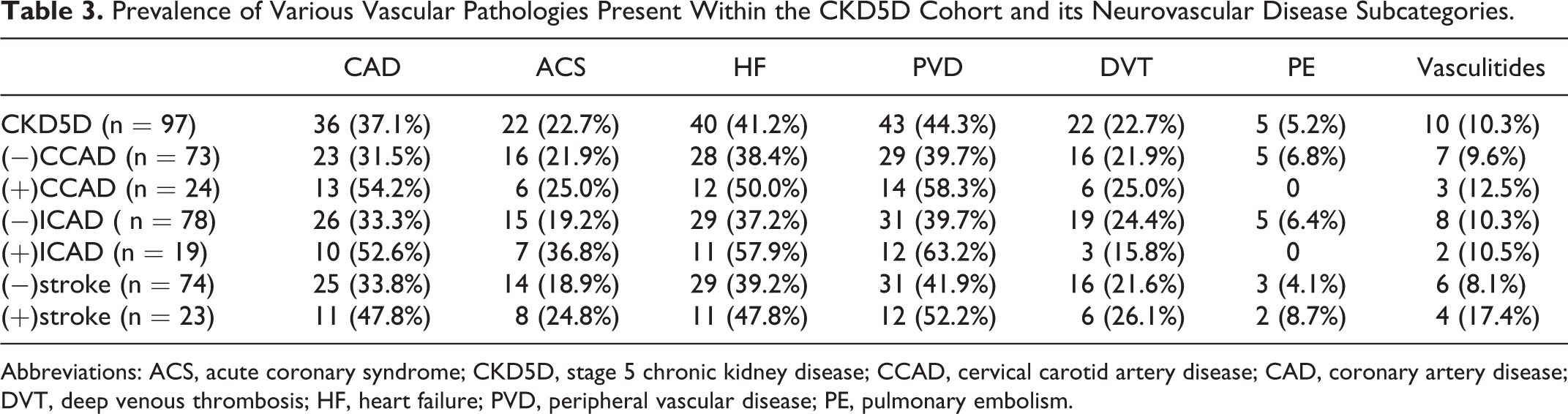
Abbreviations: ACS, acute coronary syndrome; CKD5D, stage 5 chronic kidney disease; CCAD, cervical carotid artery disease; CAD, coronary artery disease; DVT, deep venous thrombosis; HF, heart failure; PVD, peripheral vascular disease; PE, pulmonary embolism.
Top quartile comparative analyses confirmed the elevations of D-dimer in patients with CKD5D stroke and NALP3 in patients with CKD5D CCAD, but also presented with other findings. Elevations of vWF in patients with CKD5D (+)CCAD and CRP in patients with CKD5D (+)ICAD could also be due to increased age generally seen in our (+) neurovascular disease groups. 21 Although elevated levels of Ang-2, TNF-α, and CD40L have been associated with unstable atherosclerotic activity and worse rate for cardiovascular mortality, it is unclear why these levels are decreased in our (+) neurovascular disease groups. 35 –37
Finally, the prevalence of various vascular pathologies present within our CKD5D cohort were enumerated and stratified by the relevant neurovascular disease subcategories (Table 3). The diseases included coronary artery disease (CAD), acute coronary syndrome (ACS), heart failure (HF), peripheral vascular disease (PVD), DVT, pulmonary embolism (PE), and the broad vasculitides. The general trend is that the prevalence of a vascular pathology is relatively greater in patients with CKD5D with a neurovascular disease, with the exception of DVT for ICAD and PE for CCAD and ICAD. Additionally, CAD, ACS, HF, and PVD seem to have similar ratios in (+) to (−) neurovascular disease prevalence across the 3 neurovascular diseases.
Limitations of our study include the relatively small size of our cohort population, as well as differences in the timing of the neurovascular disease events experienced by the patients, particularly in terms of acute stroke. Additionally, samples were gathered only from the Loyola Outpatient Dialysis Center, the patient demographics of which might not reflect that of other communities. The definition of an acute stroke event in our study included both hemorrhagic and ischemic subtypes, and differences in blood biomarkers levels between these two might be better appreciated with a greater cohort size. Possible reasons for the lack of more significant differences in biomarker levels between the (+) and (−) neurovascular disease groups could be due to the blood–brain barrier, which might filter out the inflammatory and hemostatic biomarkers of our study. This could be besides the fact that systemic inflammation and ischemic events tends to disrupt the blood–brain barrier. 38 – 41
Conclusions
This study demonstrates that NALP3, an integral component of inflammasomes, is a potential biomarker in the risk stratification of CCAD, while other biomarkers may be of some limited value in the risk stratification of neurovascular deficits in the CKD5D population. Future investigation should also consider the diagnosis of atrial fibrillation in patients with CKD5D with neurovascular diseases, as well as related biomarkers such as natriuretic neuropeptides and the cardiac troponins I and T. Furthermore, as the diagnosis of CCAD and ICAD were not mutually exclusive in some of the cases of our patients with CKD5D, future investigations should consider analyzing these patients with concurrent neurovascular atherosclerotic processes.
Supplemental Material
Supplemental Material, Table_S1 - Biomarker Profiling of Neurovascular Diseases in Patients with Stage 5 Chronic Kidney Disease
Supplemental Material, Table_S1 for Biomarker Profiling of Neurovascular Diseases in Patients with Stage 5 Chronic Kidney Disease by Justin Lee, Jack Bontekoe, Brandon Trac, Vinod Bansal, José Biller, Debra Hoppensteadt, Paula Maia, Amanda Walborn, and Jawed Fareed in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors gratefully acknowledge the staffs of the Department of Pathology at the Loyola University Medical Center and the Loyola Outpatient Dialysis Center for the expert collection of blood samples. We would also like to thank members of the Hemostasis and Thrombosis laboratories for their continued guidance and collaboration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number T35HL120835.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.