
Abstract
Background
A venous thromboembolism (VTE) bundle was launched in 2016 at the University of Illinois Hospital aiming to reduce the rate of VTE in the neurosurgical ICU. Main elements of the bundle included correct and early use of intermittent pneumatic compression and subcutaneous heparin.
Methods
Patients with SAH were retrospectively identified from 2014 until 2018. VTE events were diagnosed using twice weekly lower-extremity venous Duplex ultrasound and chest computerized tomography when appropriate.
Results
A total of 133 patients was included in each group. The incidence of VTE was not significantly different before and after the bundle (15% vs. 12%, p = 0.47). No difference was found regarding new episode of intracranial hemorrhage secondary to SQH (1.5% vs. 2.1%, p = 0.65). Multivariate analysis demonstrated that longer ICU LOS, higher Caprini score, and presence of baseline lung diseases were associated with VTE development.
Conclusions
With a median Caprini score of 9, our patient population was found to be at high risk for developing VTE. The implementation of the VTE bundle did not significantly reduce the rate of VTE in patients with non-traumatic SAH at UIH.
Introduction
Venous thromboembolism (VTE) remains a common morbidity in patients with subarachnoid hemorrhage (SAH). Past studies have reported the incidence of VTE ranging from 0% to as high as 24%, most occuring within the first two weeks following SAH.1,2 The higher rate is often associated with the use lower-extremity surveillance ultrasonography, where higher rates of asymptomatic deep vein thrombosis were detected. Collectively, past studies have identified various risk factors for developing VTE including immobility, presumed infections, presence of central venous catheter, older age, black race, male sex, teaching hospital, congestive heart failure, neurologic disorders, paralysis, coagulopathy, fluid and electrolyte imbalance, and obesity.1–4 In 2015, the Neurocritical Care Society published an evidence-based guideline on Prophylaxis of Venous Thrombosis in Neurocritical Care Patients. 5 They recommended the initiation of subcutaneous heparin (SQH) and intermittent pneumatic compression device (IPC) in all patients with SAH as soon as possible. The guideline also highlighted the safety and potential benefits of early ambulation in neurologically and medically stable patients with a good grade as another measure to reduce the risk of VTE and even lower the frequency and severity of vasospasms.5,6
At the University of Illinois Hospital (UIH), a retrospective, observational study was completed in 2010 to identify incidence and risk factors of VTE in patients with non-traumatic hemorrhagic stroke, primarily in SAH and intracerebral hemorrhage (ICH). The VTE incidence was reported at 18.3% in patients with SAH and found lower compliance to SQH, increase in length of intensive care unit stay, and lower physical therapy (PT) sessions as independent risk factors for developing VTE. With persistent observation of high incidence noted in this patient population over the years, a VTE bundle was developed by the neurosurgical quality and improvement committee for patients admitted to the Neuroscience Intensive Care Unit (NSICU) to decrease the incidence of VTE. In this study, we sought to evaluate the impact of such bundle on the rate of VTE and other pertinent outcomes.
Methods
Study Design and Participants
Upon receiving the approval from our institutional review board, we conducted a retrospective, single-center, pre- and post-cohort study at our institution between April 2014 and July 2018. Since the VTE bundle had been implemented at our institution in April 2016, this timeframe allowed us to evaluate its impact on the outcomes of interest at a two-year snapshot before and after. Patients were categorized into either pre- or post-bundle group. Based on our historical aforementioned VTE rate of 18.3%, we would need 83 participants per study arm to see a 75% reduction of VTE events as a result of the bundle, assuming power of 80% and alpha of 0.05. Patients over 18 years of age admitted to UIH with a confirmed diagnosis of non-traumatic SAH, using ICD-9 (430) and ICD-10 (I60.00 – I60.90) codes, were included. The exclusion criteria included patients with intensive care unit (ICU) survival less than 72 hours, history of traumatic brain injury, use of continuous infusion of unfractionated heparin immediately after aneurysm treatment, whose admiting diagnosis was not SAH, and past SAH diagnosis presenting to clinic as an outpatient visit. Both groups received standard of care at UIH for the treatment of SAH, including twice weekly lower extremity venous duplex ultrasound scan (VDUS) until death or ICU discharge, whichever occured first. The VTE bundle was developed based on the ninth edition of the American College of Chest Physicians guidelines. 7 The VTE bundle included VDUS within 24 hours of admission, patient/family education on prevention of VTE within 48 hours of admission; prospective and daily audit on the use of IPC (proper position of sleeves and functional status of the device); and SQH (at the dose and frequency at the discretion of the treating physician) as early possible, preferrably within 24 hours of admission to the NSICU. The VTE bundle was a joint and multidisciplinary collaboration between physicians, nurses, pharmacists, and physical therapists. Prior to its implementation, the VDUS and patient education had not been done consistently and within the 24- and 48-hour timeframes, respectively. The quantification of IPC use was solely dependent on charting and did not reflect the actual compliance. Early mobility with PT was also strongly encouraged as part of the bundle initiative. However, for the purpose of this study, we decided not to measure this particular element due to lack of objective findings to best capture it. Days ambulated were defined as days patients ambulated without any assistance.
Outcomes
The primary outcome was the incidence of acute VTE, as detected by routine VDUS and chest computed tomography (CT) when there was a suspicion for pulmonary embolism (PE). In the post-bundle group, VTE events detected at admission to UIH NSICU were not included in the final analysis given a large amount of outside hospital transfers to our institution. The secondary outcomes were proportions of patients with ICH during the period in which SQH was given and disposition status (dependence versus independence). Independent disposition status was defined as discharged to home, whereas discharging to skilled nursing facility, sub-acute and acute rehabilitation facility, nursing home, and death were counted as dependent.
Data Collection
All pertinent data points from admission up to date of VTE diagnosis or discharge from hospital, whichever occurred first, were collected directly from the electronic health record. Data points regarding risk factors known to cause VTE were collected until the day of VTE diagnosis in order to best capture associated contributors leading to such event. We also collected the Hunt-Hess and modified Fisher scores given their strong association with the overall outcomes and risks of symptomatic vasospasm, one of which had been deemed as a predictor of VTE in our patient population.8,9 Moreover, many studies validated the association between a high Caprini risk category and the risk of VTE development in patients undergoing craniotomy (ie up to 6% risk of VTE in the absence of pharmacological or mechanical thromboprophylaxis). 7 As a result, we sought to collect an array of Caprini score components, many of which were also found to be VTE risk factors in the SAH patient population..2,3,9,10 The final mean Caprini score was calculated and reported for the overall cohort. Presumed or documented infection was defined as the initiation of antimicrobial therapy as a treatment course. Patient was deemed to have mobilized if the documented activity stated “ambulate without assistance.”
Statistical Analysis
All continuous variables were tested for normality using the Shapiro-Wilk test. Parametric continuous data were analyzed using the student's t-test and reported as means with standard deviations. Non-parametric continuous data were analyzed with the Mann-Whitney U-test and reported as medians with interquartile ranges (IQR). For categorical variables, the Chi-square test (or Fisher's exact test when n < 5) was utilized. All pertinent VTE risk factors were analyzed using univariate analysis, followed by multivariate regression analysis. A p-value of less than 0.05 was considered statistically significant.
Results
Study Population
A total of 813 potential patients were identified using the aforementioned ICD codes. However, 547 of them were excluded. The most common reasons for exclusion were outpatient encounters, SAH as a complication of a different primary problem, death within 72 hours from admission, and traumatic SAH. As a result, 133 patients were included in each group. Our patients in the two groups were average age in the upper 50 s and many without major comorbidities. The majority of patients in both groups presented with a Hunt-Hess score of 2 and modified Fisher grade of 3 but this data point was missing in 12.8% and 0.8% in the two groups, respectively. Aneurysm clipping was found to be the most common surgical intervention. Other baseline characteristics were similar between the two groups with the exceptions of rate of mechanical ventilation, phytonadione use, major surgery (>45 min), minor surgery (<45 min), Caprini score, and hospital length of stay (LOS). See Table 1 for the complete set of baseline characteristics.
Baseline characteristics and reported VTE risk factors.

Abbreviations: SD, standard deviation; BMI, body mass index; INR, international normalized ratio; EVD, external ventricular device; IQR, interquartile range; ICU, intensive care unit; LOS, length of stay; VTE, venous thromboembolism; SQH, subcutaneous heparin.
Intervention and Outcomes
Among 133 patients in the post-bundle, 31% of them were started on SQH on the first day of admission compared to 35% in the pre-bundle (p = 0.18). However, 92% of patients were started on IPC on hospital day 0 in the post-bundle compared to 72% in the pre-bundle (p < 0.001). Out of all intended interventions within the VTE bundle, initiation of IPC and its compliance were found to be significantly higher in the post-bundle (see Table 2).
Compliance rate to the VTE bundle: early and routine use of SQH and IPC

Abbreviations: SQH, subcutaneous heparin; IQR, interquartile range; IPC, intermittent pneumatic compression.
For the primary outcome, there was no significant difference between the two groups regarding the incidence of acute VTE: 15% in the pre-bundle compared to 12% in the post-bundle, p = 0.47. Average time to VTE diagnosis was 13.5 vs 12.4 days, respectively. During the NSICU stay, where the VTE bundle was implemented from the day of hospital admission, VTE was diagnosed in 14% vs 11% in pre- vs post-bundle (p = 0.79). Breaking down the VTE events by subtypes, we found no significant differences between the two groups with all four major subtypes [asymptomatic lower deep vein thrombosis (aDVT), symptomatic lower DVT, upper DVT, and PE]. Asymptomatic lower DVT was found to be most prevalent in both groups. There was no significant difference on the rate of ICH during SQH therapy: 1.48% in the pre-bundle versus 2.26% in the post-bundle. The proportions of patients independently discharged were statistically lower in the post-bundle (60% vs 42%, p = 0.049). See Table 3 for the complete results of the primary and secondary outcomes.
Primary and secondary outcomes

Abbreviations: VTE, venous thromboembolism; ICU, intensive care unit; IQR, interquartile range; LE US, lower extremity ultrasound; DVT, deep vein thrombosis; ICH, intracranial hemorrhage; SQH, subcutaneous heparin.
Risk Factors for VTE
In a univariate analysis, the following variables were significantly different between patients with and without VTE: Hunt and Hess scale 1-2 vs. 3-5, modified Fisher 1-2 vs. 3-4, presence of external ventricular drain, history of lung disease, documented bedrest for ≥72 hours, blood product usage, use of mechanical ventilation, use of phytonadione, history of hip or knee surgery, total number of major surgeries, total median duration of major surgeries, Caprini score, NSICU LOS, number of missed low-dose UFH, IPC compliance, and number of days ambulated. Using a multivariate regression analysis, Caprini score, NSICU LOS, and the presence of baseline lung diseases (ie asthma or COPD) were found to be significantly associated with VTE (see Table 4). The NSICU LOS was chosen in lieu of that of the hospital as these two variables were correlated and most VTE events took place in the NSICU.
Multiple logistic regression analysis: factors associated with VTE development
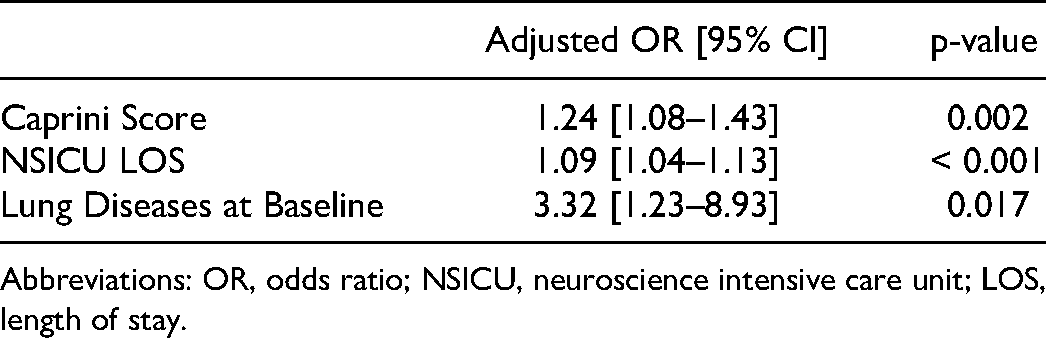
Abbreviations: OR, odds ratio; NSICU, neuroscience intensive care unit; LOS, length of stay.
Discussion
Our study demonstrated no significant impact of the VTE bundle on the overall 12% incidence of VTE. This incidence is similar with the reported range noted in the literature for SAH population, typically ranging from 4.4% to 21%.1–4,9 Furthermore, our study also identified three significant predictors of VTE – Caprini score, NSICU LOS, and the presence of baseline lung diseases. This finding corroborates immobility as the primary underlying cause of increased risk of VTE in SAH patients. This is particularly relevant in SAH population given the typically more prolonged LOS for vasospasm monitoring compared to patients with ICH and acute ischemic stroke. On the other hand, the presence of lung diseases at baseline, particularly chronic obstructive pulmonary disease (COPD), had been previously reported in the literature as a risk factor for VTE. Both COPD disease severity and activity were found to put patients at higher risk for VTE, especially PE events.11,12 Several mechanisms have been proposed including baseline immobility and comorbidities along with the pro-inflammatory state found in patients with COPD.
To our best knowledge, our study is the first one to incorporate Caprini score calculation to predict the VTE rate in patients with non-traumatic SAH. With the median score of 9 in both groups, our patient population is considered at high risk of VTE development. With a Caprini score above 8 in general surgical population, the estimated rate VTE was found to be 10.7% and would have a 60% reduction in symptomatic VTE events upon receipt of chemoprophylaxis. 10 The use of IPC alone had been found to be effective in reducing the rate of DVT in a mixed neurosurgical population (RR, 0.41; 95% CI, 0.21 to 0.78). 13 Nonetheless, the additive benefit of IPC in lowering VTE incidence is now challenged by the PREVENT trial by Arabi and colleagues. In this study, IPC was applied to both lower limbs in a mixed ICU population, most of which were medically ill and already receiving VTE chemoprophylaxis for at least 18 hours daily (study group). The authors reported a high compliance rate of IPC (up to 98.1% with a median of 22 hours per day) in the study group and minimal use of IPC (10.2% with a median of 0 hour per day) in the control group (chemoprophylaxis alone). They ultimately demonstrated a failure of routine use of IPC in reducing the rate of PE or a composite outcome of VTE or death from any cause at 28 days in those already had been receiving chemoprophylaxis. 14 In our study, 70.68% and 59.4% patients of the pre- and post-bundle, respectively, were initiated on SQH by hospital day 2, with an overall median of missed dose of 1. Given the similar and high compliance rate to SQH in both groups, the increased IPC compliance in the post-bundle therefore did not clinically translate into a reduction of VTE rate. Such high IPC compliance rate was made possible by our nursing staff to ensure the early and consistent implementation of mechanical VTE prophylaxis, especially when chemical prophylaxis was not possible.
Regarding the safety outcome, our study further once again illustrated the minimal risk of using SQH in SAH population. It is important to acknowledge that 60.15% of patients in the post-bundle did have an EVD in place while receiving SQH. This is often a concern among clinicians in starting chemoprophylaxis due to the increased theoretical risk of ventriculostomy-related hemorrhage. With a rate of ICH complication up to 2.26% between the two groups, the benefit of using SQH may potentially outweigh the potential risk of hemorrhages in most individuals, as aforementioned in the literature.13,15–17 Lastly, the lower proportion of patients being independently discharged in the post-bundle group may be due to a higher level of acuity of SAH, demonstrated by a higher proportion patients with mechanical ventilation, higher Hunt-Hess score, and major surgeries lasting longer than 45 min.
Our study provided more insight into the controversy of VTE prevention in patients with non-traumatic SAH. Despite receiving both mechanical and chemical prophylaxis, our patient population still experienced a relatively high rate of VTE (12% in the post-group). Unlike other high-risk patient populations (eg trauma), switching from SQH to low-molecular weight heparin (LMWH) has not been fully investigated. LMWH is not necessarily more advantageous than SQH given its potentially higher bleeding risk and longer elimination half-life. 18 Taking a different approach, Kunz and colleagues conducted a retrospective trial evaluating the role of therapeutic anticoagulation with heparin compared to its prophylactic dosing using different aPTT goals (< 40 vs. 50–60 seconds, respectively). They found no significant difference in terms of VTE rate and, unsurprisingly, a higher rate of SAH-associated ICH in the therapeutic group. 19 Moving forward, it would be wise to screen patients at baseline and frequently thereafter for VTE along with stratify them into the appropriate risk category. Based on our study, the presence of baseline lung diseases coupled with a high Caprini score and prolonged ICU length of stay may put the patients at the highest risk. In addition to the use of IPC and SQH, the best strategy to prevent VTE in these patients remains unclear.
Our study is not without limitations. The lack of full compliance to early initiation of IPC and SQH upon admission may have led to underexposure and subsequently, the lesser effect on the overall VTE outcome. Furthermore, the documented IPC compliance was done as daily snapshots and did not capture the entirety of each hospital day. Finally, future investigators may consider further evaluating mobility status, level of physical activity, and/or distance traveled within the hospitalization as meaningful and novel methods to reduce VTE incidence. In our study, we were not able to objectively collect the level of patient activity via PT progress notes. The retrospective nature of the study made it very challenging to quantify it, not to mention that not all patients were able to mobilize during their admission.
Conclusion
Based on our cohort's median Caprini score of 9, all patients with non-traumatic SAH were found to be at high risk for developing VTE. The implementation of the guideline directed VTE bundle comprising of SQH with adjunctive IPC, while optimized the IPC compliance rate in the post-group, did not significantly reduce the rate of VTE in patients with non-traumatic SAH. Caprini score, ICU LOS, and presence of lung diseases at baseline were found to be predictive of VTE development. Further studies are warranted to investigate novel means to prevent VTE, especially in the realm of early mobility and physical activity post-SAH.
Our study findings were presented virtually at the Thrombosis and Hemostasis Summit of North America in 2020. We received no funding for the study.
Footnotes
Acknowledgements
We would like to acknowledge the nursing, physical therapy, medical, and pharmacy staff of the Neuroscience Intensive Care Unit at the University of Illinois Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.