
Abstract
Venous thromboembolism (VTE), encompassing deep venous thrombosis and pulmonary embolism, is a potentially fatal but preventable complication of stroke. Reported rates of VTE after stroke have decreased over the last four decades, possibly due to the implementation of stroke units, early mobilization and hydration, and increased early use of antiplatelets. Additional means of thromboprophylaxis in stroke include mechanical methods (ie, compression stockings) to prevent venous stasis and medical therapy including antiplatelets, heparins, and heparinoids. Risk of VTE must be balanced by potential risk of hemorrhagic complications from pharmacotherapy. Unfractionated heparin, low-molecular-weight heparin (LMWH), and danaparoid are acceptable options for chemoprophylaxis though none have shown superior efficacy for VTE prevention without an associated increase in major hemorrhage. The efficacy and timing of pharmacological thromboprophylaxis in hemorrhagic stroke are not well defined. Graduated compression stockings are associated with an increased rate of adverse events and are not recommended and intermittent pneumatic compression stockings require further investigation.
Keywords
Introduction
Venous thromboembolism (VTE) encompasses both deep vein thrombosis (DVT) and pulmonary embolism (PE). The incidence of VTE among patients with stroke is high, and PE remains the third-highest cause of case fatality in stroke.
Stroke places patients at high risk of VTE. Immobility is generally a key risk factor for VTE and as many as two thirds of patients will be immobile or require assistance with walking immediately after their stroke. A third will be nonambulatory or require assistance at 3 months.1,2 Immobility due to stroke may be compounded by deconditioning and by comorbidities including dementia, arthritis, and peripheral vascular disease. 3 Systemic inflammation from cerebral injury4–6 and infectious complications may also contribute to thrombosis risk.
Antithrombotic therapy been widely investigated as a means of thromboprophylaxis alongside nonpharmacologic interventions including mobilization, hydration, and mechanical methods. In addition to being a major risk factor for VTE, stroke is also a major risk factor for intracranial bleeding or, in the case of hemorrhagic stroke, hematoma expansion.
The weighing of the benefits of thromboprophylaxis against the risks of hemorrhage is an ever-present challenge for those involved in post-stroke care and necessitates a careful assessment of the available evidence.
Methods
A literature search (PubMed) was performed to locate relevant articles and studies pertaining to the incidence of VTE in stroke and trials of thromboprophylaxis in stroke. The reference lists of relevant articles were then hand-searched for other references. Relevant articles also underwent a “cited reference search” (ISI Web of Science). Studies that were not in English language or published in abstract form only were excluded. Specific search terms included “venous thromboembolism,” “DVT,” “deep venous thrombosis,” “pulmonary embolism,” “stroke,” ischemic stroke,” “intracerebral hemorrhage,” “ICH,” and “subarachnoid hemorrhage,” “prophylaxis,” “thromboprophylaxis,” “physical,” “mechanical,” and “electrical stimulation.”
Epidemiology
Most DVT after stroke is asymptomatic. Reported incidence of VTE after stroke varies on the timing of screening and sensitivity of the screening modality. 7
Studies conducted prior to the era of routine prophylaxis report a post-stroke deep venous thrombosis (DVT) rate of 45% to 75% detected by 125I-fibrinogen scanning.8–10
Ischemic Stroke
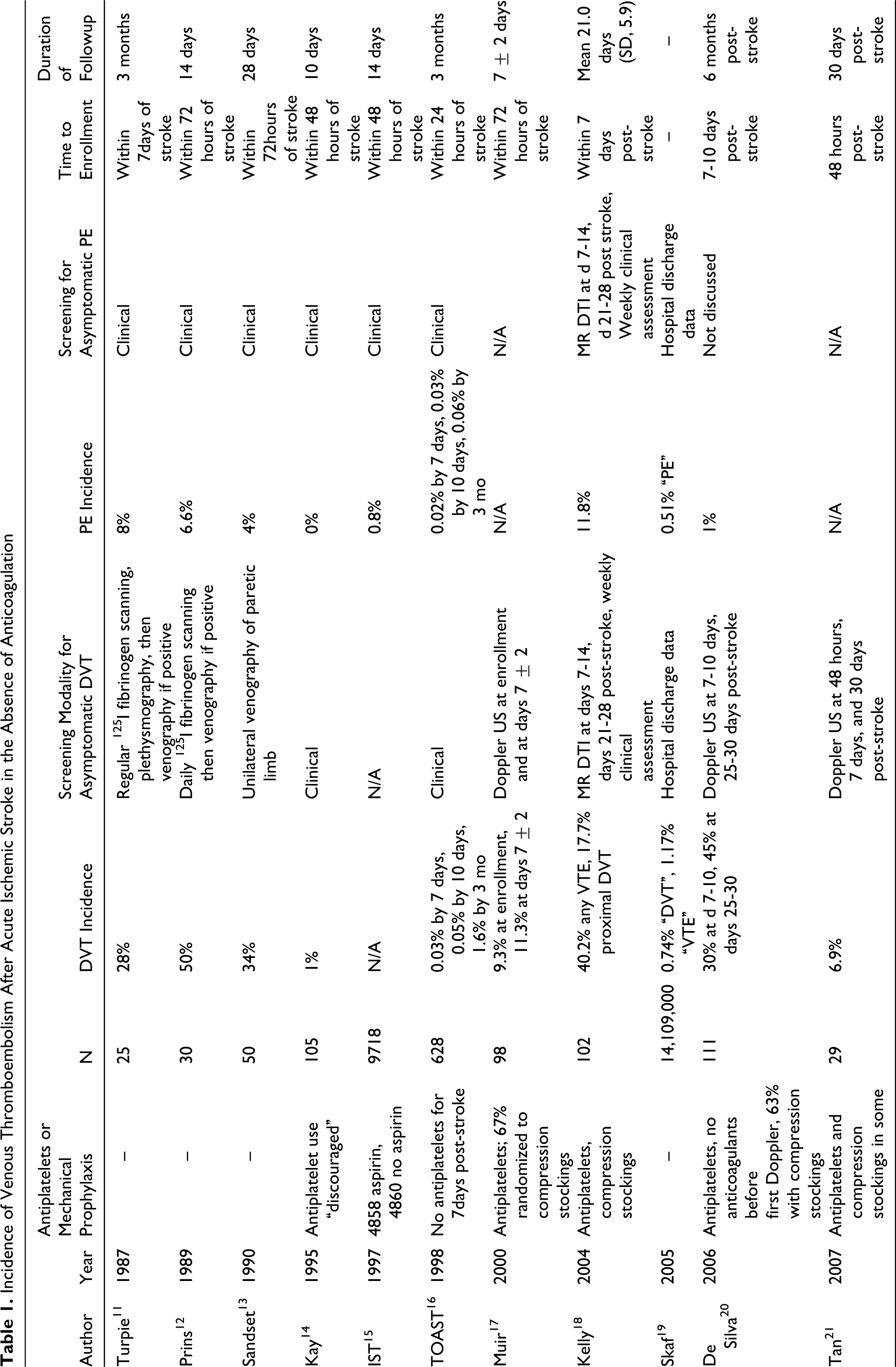
The majority of studies that report thrombotic complications of stroke does not distinguish between ischemic and hemorrhagic index events. The reported incidence of clinically detected DVT in ischemic stroke ranges from 1% to 1.6%, whereas methods that screen for asymptomatic thrombi report a much higher incidence. Incidence detected by fibrinogen scanning or venography is 28% to 50%, and by Doppler US, 6.9% to 30%. Rates of clinically detected PE vary from 0% to 6.6% after 2 weeks, and up to 8% after 3 months. (Table 1, 2 )
Incidence of Venous Thromboembolism After Acute Ischemic Stroke in the Absence of Anticoagulation
Pooled Estimate of Incidence of Venous Thromboembolism After Acute Ischemic Stroke by Screening Modality
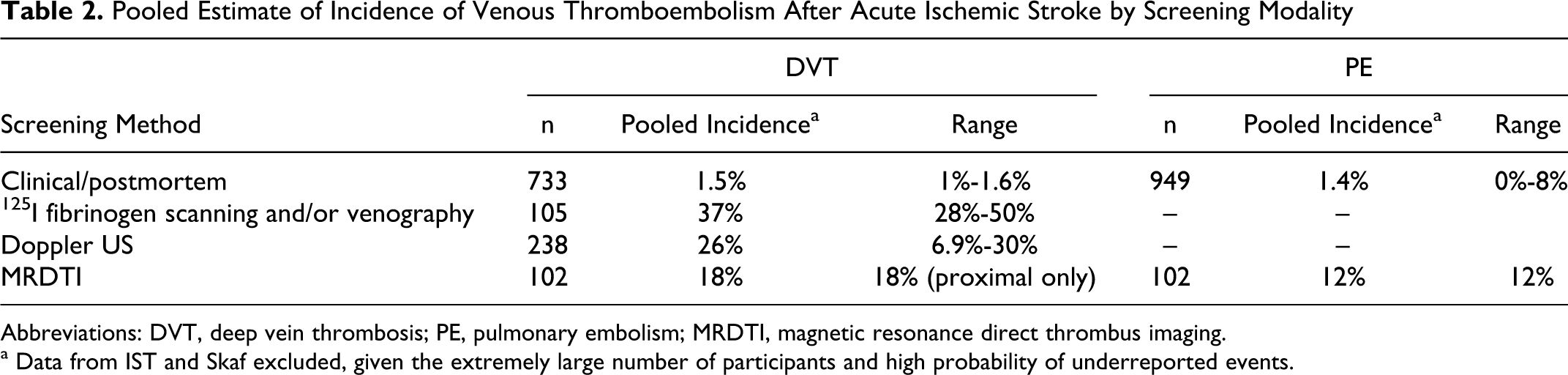
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism; MRDTI, magnetic resonance direct thrombus imaging.
a Data from IST and Skaf excluded, given the extremely large number of participants and high probability of underreported events.
In a 2004 study where patients with ischemic stroke received care per the UK guidelines, at 3 weeks there was 3% incidence of clinically detectable DVT and 18% incidence of DVT detected by magnetic resonance direct thrombus imaging (MRDTI). There was an 11.8% incidence of PE on MRDTI and a 5% incidence of clinically detected PE. 18 Using the criteria of oxygen saturation ≤92% and respiratory rate of >20 minutes as being “symptomatic” for PE, only 3% of clinically evident PE were detected by the attending medical team. 18 In the CLOTS-1 trial, in which the majority of participants (91%) had an ischemic event, 10.5% of controls receiving routine care (including antiplatelets or anticoagulants) without graduated compression stockings (GCS) had DVT at 30 days postevent by Doppler US, a less sensitive screening technique. Incidence of PE on imaging 22 or at autopsy was 1.3%
Intracerebral Hemorrhage
Overall, reported rates of VTE in intracerebral hemorrhage (ICH) range from 16% to 21% for DVT detected by regular Doppler US screening23–25 and from 0.4% to 2% for clinically diagnosed PE. 26 In controls from 3 trials of recombinant factor VIIa for ICH, rates of clinically diagnosed DVT and PE were 1% to 3% and 1% to 2%, respectively. 23
Some studies directly comparing the rates of VTE between patients with ischemic and hemorrhagic strokes suggest that VTE may occur more frequently in ICH. This may be a result of more severe weakness, depressed level of consciousness, and avoidance of routine antiplatelets in the ICH group. 27 A retrospective cohort of administrative data from an American tertiary care center found a higher rate of DVT and PE in ICH than in ischemic stroke (DVT 1.9% of 1126 ICH vs 0.5% of 15 599 ischemic stroke; PE 0.4% vs 0.1%). 28 A larger retrospective study of American administrative data from the National Hospital Discharge Survey found the same (DVT 1.37% of 1 606 000 ICH vs 0.74% of 14 109 000 ischemic stroke; PE 0.68% vs 0.51%). 19 A substudy of patients with hemorrhagic stroke initially included in the International Stroke Trial found that patients with ICH had a higher rate of clinically diagnosed PE than patients with ischemic stroke (1.3% vs 0.7% P = .06) when controlling for disease severity.29,30
Subarachnoid Hemorrhage
There are scant data specific to patients with aneurysmal subarachnoid hemorrhage (SAH) in the neurosurgical literature regarding prevention or prevalence of VTE. The rate of DVT detected by Doppler US was 14% in 1 series of patients with SAH without prophylaxis; the reported rate31–34 of PE ranges from less than 1% to 2%.
Morbidity and Mortality
Pulmonary embolism carries a mortality rate 35 of 30% to 50% and causes 10% to 25% of case fatality in stroke. It is the third leading cause of post-stroke mortality after the stroke itself and secondary infection.36–38 The rate of clinically evident PE after DVT ranges from 15% to 35%.9,35 Pulmonary embolism rates were highest 2 to 4 weeks after stroke in 1 series. Pulmonary embolism, however, may occur many weeks post-stroke, which heralds the common clinical problem of how long to provide prophylactic therapy. 36 A retrospective series found 50% of 30 patients with stroke having PE presented with sudden death. 39
Thrombi form in the proximal or distal limb; PE associated with proximal DVT is less frequent but more likely to be clinically evident and carries higher morbidity and mortality. 35 Two thirds of DVT after stroke were below knee, 40 explaining why most DVT associated with stroke is asymptomatic.
In a nonstroke population, the risk of proximal extension of distal DVT is 1 in 6; one study found a 20% rate after stroke.11,18 Peak incidence of DVT is between days 2 and 7 post-stroke.40,41 Deep vein thrombosis most often occurs in the paretic leg though up to 22% will have bilateral DVT. 18
Risk Factors
Risk factors for VTE in stroke include older age, greater limb weakness, 42 greater stroke severity, or severe functional impairment. In one study examining clinically evident and asymptomatic VTE by MRDTI, age >70 (odds ratio [OR] 2.9; 95% confidence interval [CI] 1.1-7.8), and severe functional impairment with Barthel Index ≤90 at 2 days post-event (OR 8.3; 95% CI 2.7-25.2) were associated with a higher risk of VTE. Rates of VTE in the PREVAIL study of patients with National Institute of Health Stroke Scale Scores (NIHSS) of ≥14 were double that of patients with NIHSS <14 (23.1% of 488 using pharmacoprophylaxis vs 11.2% of 1268 patients using pharmacoprophylaxis). 18
Deep Vein Thrombosis Prophylaxis
Both DVT and PE are preventable complications of stroke. Reported rates of VTE after stroke have decreased over the last four decades 7 ; possibly attributable to parallel improvements in post-stroke care including implementation of stroke units, early mobilization and hydration, and increased early use of antiplatelets. Institution of measures to prevent VTE after stroke is used as a quality indicator for stroke centers. 43
Additional means of thromboprophylaxis in stroke include mechanical methods (ie, compression stockings) to prevent venous stasis and medical therapy including antiplatelets, heparins, and heparinoids. Risk of VTE must be balanced by potential risk of hemorrhagic complications from pharmacotherapy, particularly in the context of hemorrhagic stroke. Nonpharmacologic methods are commonly used as an adjunct to chemoprophylaxis or in patients with contraindication to anticoagulants.
The literature on evidence-based therapy for both pharmacologic and nonpharmacologic prevention of VTE in stroke is not robust with practice guidelines often being based upon extrapolations from studies in other, primarily surgical, patient groups. The stroke population, however, defies straightforward comparisons to other study populations: they are typically elderly and have more comorbid illness than their counterparts; in addition their duration of immobility may be prolonged and they remain at risk of developing additional complications, such as infection, that may heighten the risk of VTE.
Optimal duration for VTE prophylaxis in stroke patients with prolonged immobility is not well defined. Deep vein thrombosis is reported in the stroke rehabilitation population in up to 10% to 30%; 20% of cases may occur after 12 weeks post-stroke onset. 44 Pulmonary embolism may occur up to 4 months post-stroke. 39 Some advocate continued prophylaxis for patients with persistent immobility.7,45 In spinal cord injured patients with complete diplegia, by 6 months post-injury the risk of DVT declines to that of the general population. 46 Whether the risk of VTE declines similarly in stroke patients is unknown and requires further study.
Types of DVT Prophylaxis
Nonpharmacologic
Early mobilization and hydration
The efficacies of early mobilization and hydration in reducing DVT have not been evaluated directly in clinical trials. Rates of DVT, however, are lower in stroke units encouraging early mobilization. 47 Early mobilization is recommended as a means to prevent VTE in guidelines from the America Heart Association/American Stroke Association (AHA/ASA), Canadian Stroke Network (CSN), Australian National Stroke Foundation (NSF), and European Stroke Organization ([ESO] Table 3 ). In addition to reducing venous stasis, early mobilization is also associated with reduced depression, 54 improved mobility, 55 and reduced costs of care. 54
Summary of Guidelines by Stroke Type
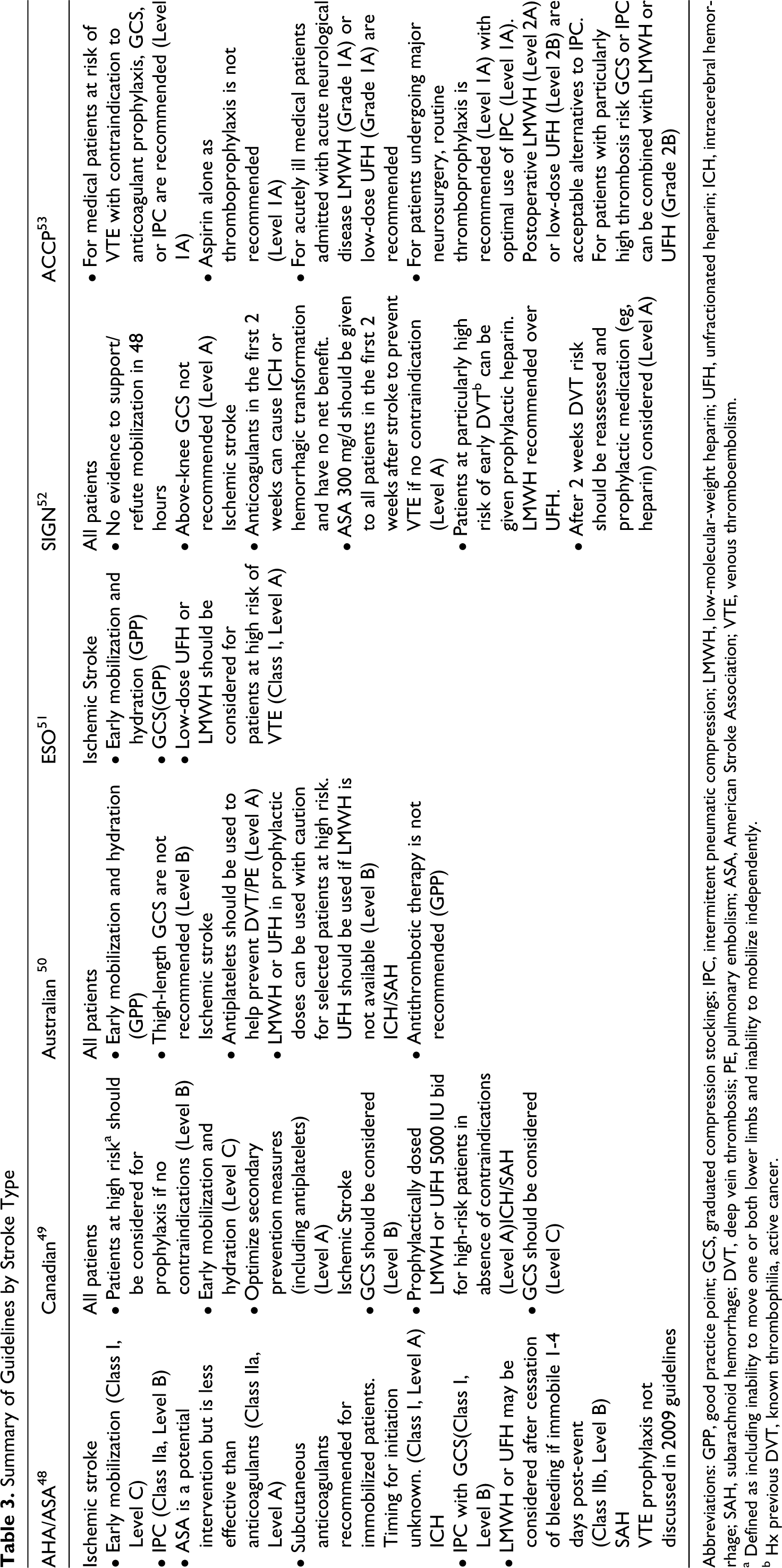
Abbreviations: GPP, good practice point; GCS, graduated compression stockings; IPC, intermittent pneumatic compression; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; DVT, deep vein thrombosis; PE, pulmonary embolism; ASA, American Stroke Association; VTE, venous thromboembolism.
a Defined as including inability to move one or both lower limbs and inability to mobilize independently.
b Hx previous DVT, known thrombophilia, active cancer.
Dehydration is strongly associated with DVT in stroke. 56 Patients with stroke are at particularly high risk of dehydration from reduced fluid intake as a consequence of dysphagia or depressed level of consciousness, even in those who are receiving nasogastric or parental fluids. 57 Hydration is recommended for VTE prophylaxis in guidelines from the CSN, NSF, and ESO (Table 3).
Mechanical Methods to Prevent DVT and PE
Nonpharmacologic methods to prevent VTE are commonly used as an adjunct to chemoprophylaxis or when anticoagulants are contraindicated. Available methods include repetitive electrical stimulation of the calf muscles, graded elastic compression stockings, and intermittent pneumatic compression (IPC) devices. Patients with dermatologic disease, severe peripheral vascular disease, or neuropathy are at greater risk of complications with mechanical therapy.58,59
Repetitive Electrical Stimulation
Electrical stimulation for the prevention of DVT was first introduced in the medical literature in the 1960s but has not been widely adopted. Induced contraction of calf muscles with intermittent application of low electrical current is thought to increase venous return and thus reduce stasis. Stimulation rates in studies vary from 2 to over 100 pulses per minute. The method has been investigated both as stand alone therapy and as adjunct to anticoagulants in small trials involving surgical60–63 and trauma64,65 patients, with inconsistent results. Electrical stimulation was investigated in 8 patients with stroke in the pilot phase of a study comparing methods of thromboprophylaxis in rehabilitation, though this method was abandoned due to discomfort and blister formation at electrode sites. 66 Studies in healthy controls suggest newer models of electrical stimulation devices employing lower currents may be better tolerated.67,68 Electrical stimulation remains underexplored in the population with stroke.
Graded Elastic Compression Stockings
Graded elastic compression stockings, commonly known as “TED stockings” in North America, are effective in preventing VTE in surgical patients 69 and, prior to CLOTS-1, were recommended for patients with stroke.48,49,51
The CLOTS-1 trial assessed the efficacy of graded elastic compression stockings in reducing VTE after stroke. A total of 2518 patients unable to ambulate independently within 1 week of ischemic or hemorrhagic stroke (excluding SAH) were randomized to routine care with or without thigh-high graded elastic compression stockings. 22 Primary outcome was occurrence of symptomatic or asymptomatic DVT in the popliteal or femoral veins on Doppler US at 7 to 10 days, and, when feasible, 25 to 30 days post-event. In all, 85.2% of participants had ischemic stroke. There was no significant difference between control and intervention groups with respect to the primary outcome, including symptomatic, asymptomatic, and below-knee DVT (10% in the graded elastic compression stockings group, 10.5% control; absolute risk reduction [ARR] 0.5%, 95% CI −1.9%-2.9%) or in PE confirmed by imaging or autopsy. No additional differences emerged in subgroup analyses examining earlier versus later randomization, concomitant use of anticoagulants or thrombolysis, or leg weakness. However, the rate of adverse events with graded elastic compression stockings, including skin necrosis and ulcerations, was 4-fold that of controls (5.1% GCS, 1.3% control; OR 4.18, 95% CI 2.40-7.27).
The CLOTS-2 trial comparing thigh-high versus knee-high graded elastic compression stockings was terminated early in light of results of CLOTS-1. Deep vein thrombosis occurred in 98 (6.3%) patients in the thigh-high group and in 138 (8.8%) in the below-knee group (ARR 2.5%, 95% CI 0.7-4.4; P = .008). 70 However, given the high adverse event rate, elastic compression stockings cannot be recommended for patients with stroke.
Intermittent Pneumatic Compression Devices
Intermittent pneumatic compression devices are thought to prevent VTE by reducing venous stasis. 71 There is some evidence that IPC devices may also affect levels and activity of endogenous fibrinolytic substances, though studies are conflicting.72–77 Intermittent pneumatic compression devices are associated with reduced risk of DVT in surgical patients. 78
Intermittent pneumatic compression devices are recommended after stroke in certain national guidelines (Table 3), though supporting evidence is not robust.48,49,53 Four completed studies have investigated IPC devices in stroke. One small study randomized 26 patients within 72 hours of clinically diagnosed stroke to below-knee IPC devices or no IPC devices for 10 days. Patients were evaluated for VTE using 125I-Fibrinogen scanning daily for 10 days. There was no significant difference between groups in the incidence of DVT (6 of 13 patients in each group). 79 Another trial compared thigh-high IPC devices with graded elastic compression stockings versus graded elastic compression stockings alone for 10 ± 2 days in 151 patients with spontaneous or traumatic ICH who were mobile or immobile at randomization. Patients were evaluated at 10 ± 2, 30, and 90 days for DVT using Doppler US. There were fewer DVT in the IPC devices group at day 10 (4.7% IPC devices group vs 15.9% control; relative risk [RR] 0.29, 95% CI 0.08-1.00). All events were asymptomatic. There were 3 proximal DVT in controls and none with IPC devices. 25 A meta-analysis of thromboprophylaxis trials 80 in an unselected population of neurosurgical patients found that IPC devices were superior to placebo in preventing DVT (RR 0.41, 95% CI 0.21-0.78).
The CLOTS-3 trial is currently investigating routine care with and without IPC devices for prevention of VTE in stroke. The study aims to enroll 2000 participants by 2014 and should provide greater clarity on the efficacy of IPC devices. 81
Pharmacologic Prophylaxis by Stroke Type
Ischemic stroke
With pharmacoprophylaxis, clinicians must balance the benefit of VTE risk reduction with associated risk of intracranial and extracranial hemorrhage. Options in ischemic stroke include antiplatelets, unfractionated heparin (UFH), low-molecular-weight heparins (LMWH), factor Xa inhibitors (heparinoids), and direct oral thrombin inhibitors (DTIs).
Antiplatelets
Studies in medical and surgical populations have demonstrated a decreased risk of DVT and PE with antiplatelet use.82,83 The mainstay of secondary prevention in noncardioembolic stroke, antiplatelets are also associated with a modest decrease in VTE in some stroke trials. Patients in The International Stroke Trial (IST) 84 receiving 300 mg of aspirin (ASA) daily had lower rates of PE than patients in the non-ASA group (0.7% of 4858 ASA patients, 0.9% of 4859 controls; OR 0.80, 95% CI 0.51-1.24). There was no difference in rates of PE in stroke patients given 160 mg ASA daily versus placebo in the Chinese Acute Stroke Trial (0.1% of 10 335 ASA patients, 0.2% of 10 320 control). Neither study prospectively evaluated VTE or had predetermined criteria for PE. 30 A meta-analysis acknowledges that PE may have been underreported. 15 A Cochrane review found a significantly lower rate of PE with antiplatelets as compared to control (71 of 20 664 antiplatelet patients vs 100 of 20 661 controls; OR 0.71, 95% CI 0.53-0.96). Deep vein thrombosis rates were only provided in 2 small studies with significant heterogeneity; there was a nonsignificant reduction with antiplatelets as compared to control (23.9% of 67 antiplatelet participants vs 28.8% of 66 controls; OR 0.78, 95% CI 0.36-1.67; P = .52). 85 The American College of Chest Physicians (ACCP) does not recommend aspirin monotherapy for thromboprophylaxis after stroke; Canadian guidelines recommend that antiplatelets use be optimized for secondary stroke prevention (Table 3), but in both cases any reduction in VTE is a secondary benefit of strategies to prevent recurrent arterial stroke.49,53
Heparins and heparinoids
In comparison to placebo, low-to-medium dose UFH, LMWH, and heparinoids have all been shown to reduce VTE after stroke. 93 Which one method is most efficacious is controversial. Direct comparison of low-dose (5000 IU twice daily [bid]) versus medium-dose (thrice daily [tid]) UFH has not been investigated, though in the International Stroke Trial, 10 000 IU daily did not reduce PE over placebo (Table 4 ). 84 Unlike UFH, LMWH has a longer half-life and can be dosed daily without monitoring, has more predictable pharmacokinetics, and a lower risk of heparin-induced thrombocytopenia (HIT). Low-molecular-weight heparin is not well reversed with protamine sulfate in the event of bleeding and is renally cleared, requiring cautious dosing in patients with renal failure. Heparinoids more selectively inhibit factor Xa and carry very low risk of HIT but cannot be reversed. Unfractionated heparin is the least expensive and can be reversed with protamine if bleeding occurs. 94 Anticoagulation should be avoided in the first 24 hours postthrombolysis; whether anticoagulation can be safely initiated before the first 24 hours in nonthrombolysis patients has not been studied.7,95,88
Commonly Used Antithrombotic Medications for DVT Prophylaxis in Ischemic Stroke and Relevant Trials a
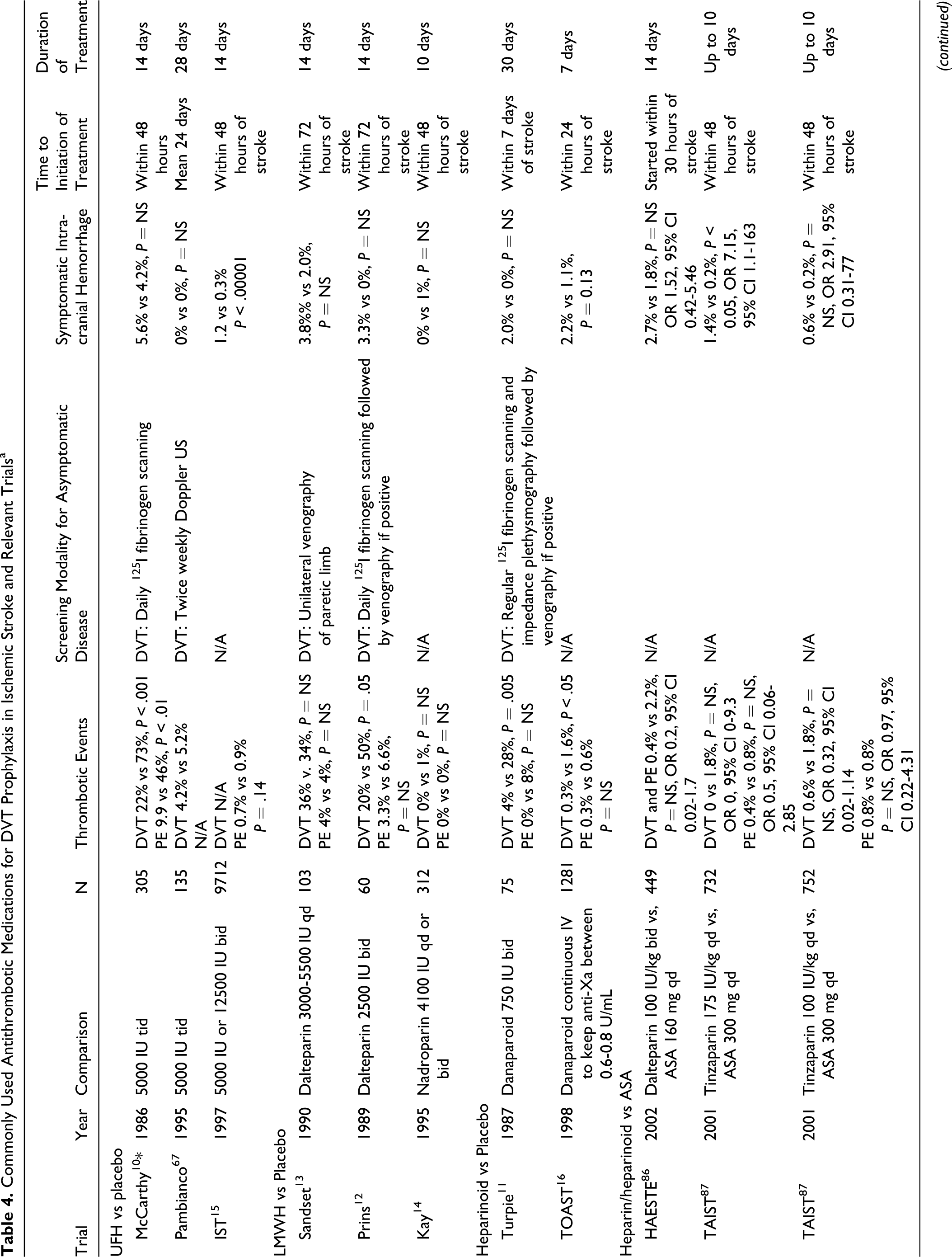
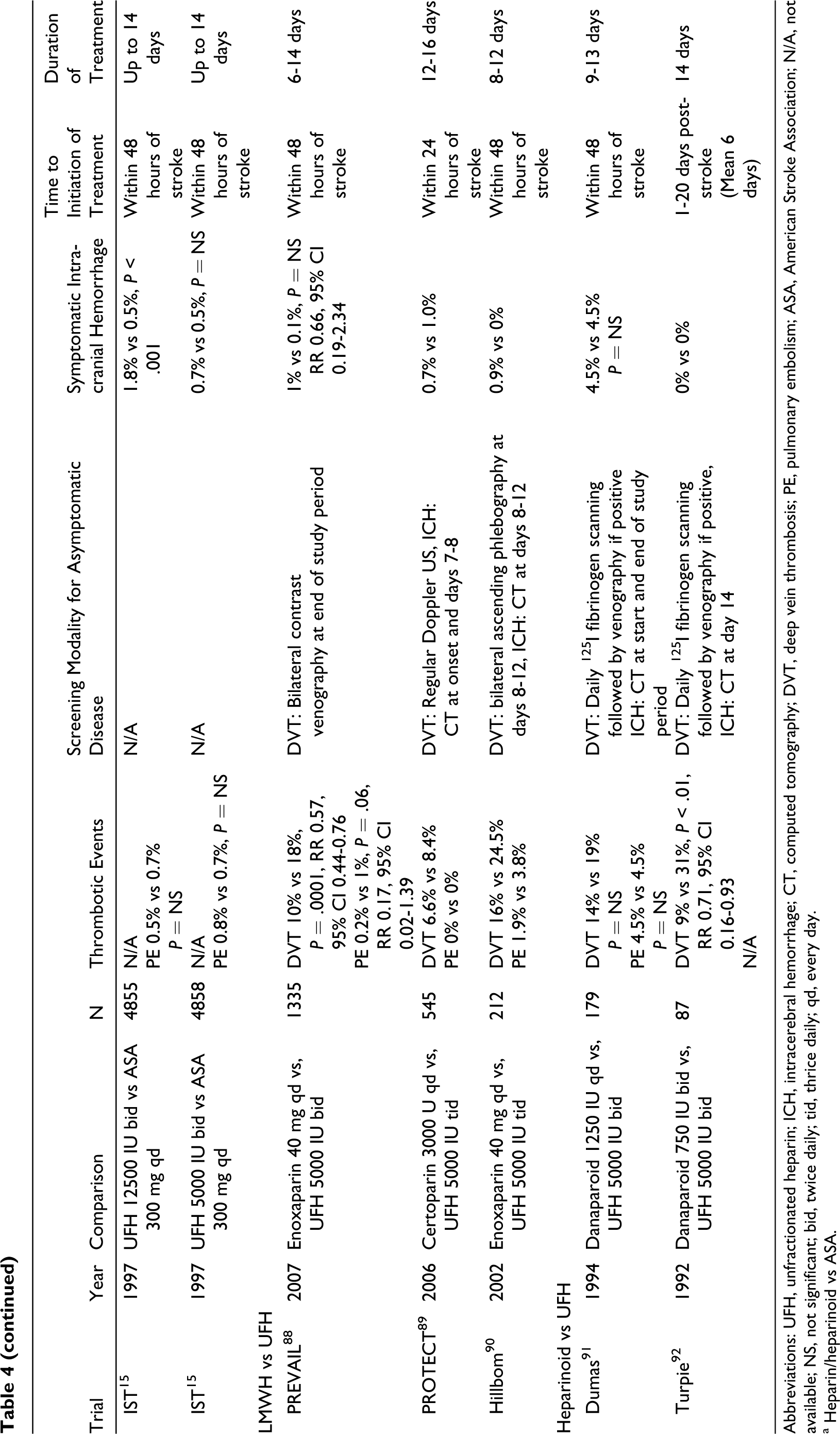
Abbreviations: UFH, unfractionated heparin; ICH, intracerebral hemorrhage; CT, computed tomography; DVT, deep vein thrombosis; PE, pulmonary embolism; ASA, American Stroke Association; N/A, not available; NS, not significant; bid, twice daily; tid, thrice daily; qd, every day.
a Heparin/heparinoid vs ASA.
A recent Cochrane review found that danaparoid and LMWH were both associated with significant reduction in DVT over UFH (OR 0.55, 95% CI 0.44-0.70; P < .00001); though this difference was no longer significant (OR 0.86, 95% CI 0.70-1.06) when analyzed in a “modified worst-case scenario” where patients who were not systematically screened for DVT and were assumed to have an event rate equivalent to that of the highest rate in controls out of all available trials (31%). Rates of PE, and intracranial and extracranial hemorrhages were too small to provide a reliable comparison between treatments. 87
Unfractionated heparin versus LMWH
In the pre-thrombolysis era, 212 patients were randomized within 48 hours of noncardioembolic ischemic stroke to 10 ± 2 days of enoxaparin 40 mg daily or UFH 5000 IU tid. There was no significant difference in the rates of DVT (16% LMWH vs 24.5% UFH), PE (1.9% vs 3.8%), intracranial hemorrhage (0.9% vs 0%), hemorrhagic transformation (13.2% vs 18.9%), or mortality (19.8% vs 26.4%). There was a trend toward increased bleeding with LMWH as compared with UFH (2.8% vs 1.9%). 96
The PROTECT trial, powered for noninferiority, randomized 545 nonthrombolysis ischemic stroke patients to LMWH cetroparin 3000 U daily or UFH 5000 IU tid. There was no significant difference in the primary end points of proximal DVT, PE, or VTE-associated death (6.6% LMWH vs 8.8% UFH, 97.5% CI −100.0-2.3; P = .008 with limit of noninferiority of 5% and P = .0117 with limit of 3%), and no difference in major intra- or extracranial bleeding (1.8% UFH vs 1.1% LMWH) or mortality (2.7% in each group). 90
The PREVAIL trial compared enoxaparin 40 mg daily to UFH 5000 IU bid within 48 hours after ictus for 10 ± 4 days after ischemic stroke in 1762 patients. Thrombolysis was an exclusion criterion only if it occurred less than 24 hours prior to randomization. Primary outcomes were symptomatic or asymptomatic DVT and symptomatic or fatal PE. Symptomatic intracranial or major extracranial hemorrhage and all-cause mortality were primary safety end points. Contrast venography, or Doppler US if venography could not be performed, occurred at day 10 ± 4. In all, 6% of the enoxaparin group and 7% of the UFH group received thrombolysis; 92% of the enoxaparin group and 90% of the UFH group took concomitant antiplatelets. There was significantly less DVT with enoxaparin (10% vs 17%, RR 0.57; 95% CI 0.43-0.75, P < .0001) and fewer PE though this did not reach significance due to a low event rate (<1% vs 1%, RR 0.17; 95% CI 0.02-1.39, P < .059). There was no difference in the rates of symptomatic intracranial hemorrhage (1% in each group, RR 0.66; 95% CI 0.19-2.34, P = .55), though the rates of major extracranial hemorrhage were significantly higher with enoxaparin (1% enoxaparin vs 0% UFH, P = .015). All-cause mortality at 14 and 90 days did not differ between groups. Thromboembolic events were 2-fold higher with NIHSS < 14 than with NIHSS ≥ 14 (8.3% enoxaparin and 14.0% UFH with NIHSS <14; 16.3% and 29.7% with NIHSS ≥ 14) though there was still significant benefit with enoxaparin. Bleeding events were also 2-fold higher in patients with more severe strokes (8.1% and 13.6% with NIHSS <14% and 16.3% and 29.1% with NIHSS ≥ 14), though there were no differences in bleeding rates with either drug. There was no significant benefit in favor of UFH in patients over the age of 75 in subgroup analysis (OR 0.72; 95% CI 0.41-1.28). 95 Critics of the study have drawn attention to the fact that enoxaparin was compared to a lower dose of heparin than in previous trials89,97 comparing the 2, that the trial was underpowered to detect hemorrhages, and that the study population was not representative of a typical stroke population given that three quarters of participants were under the age of 75.
Unfractionated heparin versus heparinoids
Danaparoid is the only Xa inhibitor investigated for VTE prophylaxis in stroke and has been compared against UFH in 2 trials in the pre-thrombolysis era. One study randomized 179 patients with ischemic stroke and leg weakness within 72 hours of onset to danaparoid 1250 IU daily or UFH 5000 IU bid for a minimum of 9 days. Patients underwent daily 125I-fibrogen scanning for DVT. There was no significant difference in the rates of DVT (14.6% danaparoid and 19.8% UFH, P = .392), PE (1.1% in each), symptomatic intracranial hemorrhage (1.1% in each), or all-cause mortality at 3 months. There was 1 major extracranial bleed with danaparoid and none with UFH. 98
Another study compared danaparoid 750 IU bid to UFH 5000 IU bid in 87 patients with ischemic stroke and leg weakness. Treatment was started as soon as possible and continued for 14 days or until discharge. The study ended prematurely due to stalled recruitment. There was a reduction in all DVT (8.9% danaparoid vs 31.0% UFH, relative risk reduction [RRR] 0.71; 95% CI 0.16-0.93, P = .014) but not in proximal DVT alone (11.9% vs 4.4%, RRR 0.63; 95% CI −1.14-0.96, P > .2). There was no symptomatic intracranial hemorrhage in either group. There was 1 major hemorrhage with danaparoid and none with UFH. 91
Direct oral thrombin inhibitors
There are no trials to date examining DTIs for the prevention of VTE after stroke. Direct thrombin inhibitor inactivates fibrin-bound thrombin and carries no risk of HIT but is associated with gastrointestinal discomfort. Dabigatran has been compared with enoxaparin for VTE prophylaxis after hip and knee arthroplasty. A recent Cochrane review found that DTIs, including dabigatran, are not superior to LMWH for prevention of VTE in orthopedic surgery, and that a detailed evaluation of symptomatic VTE events and mortality as well as more robust follow-up are required to more fully determine the safety profile of dabigatran. 92
Intracerebral Hemorrhage
The risk of facilitating hematoma expansion or causing another intracranial bleed in a patient with underlying susceptibility dissuades many clinicians from using anticoagulants for VTE prophylaxis in ICH. There is inconsistency among guidelines for VTE prophylaxis in ICH (Table 3). 53 A recent study 99 of the American “Get With the Guidelines—Stroke” registry found patients with ICH are also less likely to receive DVT prophylaxis per AHA/ASA guidelines than patients with ischemic stroke (OR 0.65; 95% CI 0.59-0.71).
The few studies published on anticoagulants for thromboprophylaxis in ICH suggest that they may be well tolerated, though this possibly reflects publication bias. Most hematoma expansion occurs early in ICH, 100 and the limited available data suggest that anticoagulation initiated 48 hours after the ictus may be safe, though this will need to be explored with large prospective randomized trials.
Unfractionated heparin
One trial investigated UFH 5000 U tid in 68 patients with ICH. Patients were designated to begin therapy on the second (22 patients), fourth 32 , or tenth 32 day following admission. The day 2 group had a significant reduction in PE that was clinically evident or detected by ventilation-perfusion scan (1 patient vs 5 in the day 4 group and 9 in the day 10 group). There was no rebleeding in the day 2 group. The timing of the rebleeding in the day 4 (1 patient) and day 10 (3 patients) groups was not described.41,101
Low-molecular-weight heparin
A total of 75 patients with ICH were randomized after 48 hours postadmission to enoxaparin 40 mg daily plus thigh-high GCS or GCS alone in 1 trial. There was no evidence in either group of hematoma expansion on computed tomography (CT) at 72 hours or later. At 1 week, there was no significant difference in DVT on Doppler US (3 in LMWH group, 1 in control; P = 1.0) or PE on spiral CT (1 patient in each group). There were no bleeding complications in either group. 102
One study examined a retrospective cohort of 407 patients with ICH who survived >48 hours after symptom onset admitted to a tertiary care center from 1993 to 2004. The exact criteria for initiating anticoagulation was not clearly outlined but appeared to be at the discretion of the treating physician, and use of anticoagulants for thromboprophylaxis appeared to increase in popularity during the study period. A total of 232 patients received anticoagulation—202 were given 20 mg enoxaparin daily, 24 received 40 mg, and 6 received other types of LMWH; 175 received neither pharmacological nor mechanical prophylaxis. Anticoagulation was initiated after 24 hours in 23%, after 48 hours in 61%, and after more than 120 hours in 16%. There was no significant difference in the rates of PE (2%, standard deviation [SD] 1 in each group), hematoma expansion (11.9%, SD 16.5 in LMWH; 11.5%, SD 11.1 control), GI bleeding, or other thromboembolic complications (6% SD 3 in LMWH; 4% SD 2 in control). 103
Safety of thromboprophylaxis in ICH has been evaluated in 2 retrospective cohorts of neurocritical care patients receiving either LMWH or UFH. One study 104 with 97 patients initiated therapy after 36 hours without evidence of hematoma expansion on repeat CT; 2 patients experienced hematoma expansion of 20.9% and 22.4%, 1 being symptomatic on day 7 and the other having asymptomatic change discovered on neuroimaging at day 9. The other study evaluated 73 patients who had ICH with intraventricular extension. Antithrombotic therapy was initiated 7 days after ictus; 2 experienced hematoma volume growth >33% within 4 days of thromboprophylaxis. 105
The safety and efficacy profile of anticoagulation in comparison to mechanical methods is not well defined and the literature would benefit from large randomized trials. The available studies are small and their methodology is not ideal. Their reported rates of VTE are far lower than those from more rigorous trials assessing the rates of VTE in stroke. Still, the current available data suggest that anticoagulants for VTE prophylaxis may be well tolerated in ICH.
Subarachnoid Hemorrhage
Retrospective series in SAH patients given low-dose UFH and LMWH suggest that there is a low rate of iatrogenic intracranial hemorrhage but this would need to be confirmed in the context of large randomized trials with rigorous definition of VTE. A recent meta-analysis of 30 studies on VTE prophylaxis in neurosurgical patients found those undergoing surgery for “vascular procedures” had higher rates of intracranial hemorrhage. 80
A study conducted on patients with aneurysmal SAH between 1978 and 1980 found a 14% incidence of symptomatic DVT confirmed by contrast venography. Patients did not receive antifibrinolytics and were mobilized on the second postoperative day. Not surprisingly there was a lower rate of DVT in those patients operated on within the first week after ictus than in those who underwent surgery 2 to 3 weeks post-SAH (10% vs 17%). No patients experienced clinical PE. The timing of DVT in relation to surgery was not explained. Patients with DVT underwent immediate anticoagulation with 5 days of heparin and 3 months of warfarin. There were no bleeding complications in any patients receiving anticoagulation, though the duration of follow-up was not reported. 33
In a retrospective cohort of 250 patients with aneurysmal SAH who received endovascular or surgical treatment and survived >15 days, all received pre- and postoperative UFH 5000 bid, GCS, and IPC. In all, 18% developed symptomatic DVT and 2% developed symptomatic PE confirmed by spiral CT. A subgroup of 125 patients who received regular screening with Doppler US had a 24% rate of DVT. On multivariate analysis, DVT was associated with number of days in hospital and number of days in ICU. The authors mention that there were “no major ICH directly linked to the use of UFH” but do not elaborate as to whether there were other ICH under other circumstances. 106
In another retrospective study, a cohort of 235 aneurysmal SAH patients received UFH 5000 bid (73% of patients) or enoxaparin 40 mg od (25%), depending on physician preference. A small proportion (4%) received a combination of both. The authors did not state whether prophylaxis was started pre- or postoperatively. A subset of 178 patients were screened by Doppler US for DVT before or at day 12 ± 2. Prevalence of DVT was 3.4% in the screened group and 0% in the clinical group. Incidence of PE confirmed by V/Q scan or spiral CT was 1.1% in the screened group and 0% in the clinical group. There was a 1.3% incidence of new intracranial hemorrhage on follow-up imaging, though the authors did not clarify which patient group experienced hemorrhage, whether the hemorrhage was symptomatic, or when the reimaging occurred. 32
In a randomized, double-blind study investigating the effects of LMWH on preventing delayed ischemia in SAH due to vasospasm, 170 aneurysmal SAH patients receiving routine care with nimodipine and triple-H therapy (hypervolemia, hypertension, and hemodilution) 107 were given enoxaparin 40 mg daily or placebo. The study drug was initiated within 72 hours after ictus and within 12 to 24 hours after the aneurysm had been secured through surgical or endovascular means. There was a significantly lower rate of associated intraparenchymal hemorrhage in the enoxaparin group at randomization. There was no significant difference between groups with respect to reversible or fixed delayed ischemia. There were 4 cases of postoperative bleeding with enoxaparin and none with placebo. There were more symptomatic DVT and PE with placebo (3 and 1 in the placebo group, respectively; 1 and 0 in the enoxaparin group). The authors concluded against routine use of enoxaparin in the early postoperative period in SAH. 34
Some centers use anticoagulation routinely in patients with SAH.32,106 The evidence for efficacy of anticoagulation in patients with SAH for VTE prophylaxis in comparison to mechanical methods is not well defined nor is the rate of ICH in SAH patients receiving anticoagulation. The risks and benefits of routine anticoagulation in this patient population would be better defined with the aid of rigorous clinical trials.
Guidelines
The controversy surrounding thromboprophylaxis in stroke is illustrated by differences among several national guidelines on post-stroke care (Table 3). Early mobilization and hydration are advocated by the majority. Most of the guidelines were published prior to the release of the results of the CLOTS-1 trial; those published afterward recommend against above-knee GCS (Australian, ESO).
Antiplatelets are mentioned in most of the guidelines as an adjunct for VTE prophylaxis. The ACCP guidelines state explicitly that aspirin alone is not recommended for thromboprophylaxis; the AHA/ASA state that aspirin is a potential intervention but is less effective than anticoagulants. The Canadian guidelines advocate for antiplatelets to be optimized among other strategies for secondary prevention, whereas the Australian and SIGN guidelines mention antiplatelets specifically as a means to help prevent VTE. Only the SIGN guidelines recommend a specific dose (aspirin 300 mg/d).
All guidelines recommend prophylaxis with antithrombotics in high-risk patients with ischemic stroke; only the SIGN guidelines specifically recommend LMWH over UFH, whereas the others state that either is acceptable.
Those guidelines that address hemorrhagic stroke have conflicting recommendations; only the AHA/ASA guidelines support the use of mechanical methods and explicitly mention the consideration of use of pharmacoprophylaxis after ICH. The Australian guidelines recommend against thigh-high GCS for all patients and against antithrombotic therapy for hemorrhagic stroke explicitly; the Canadian guidelines recommend that mechanical methods be considered in cases of hemorrhagic stroke.
Future guidelines on post-stroke care will need to highlight the importance of mobilization and hydration, update recommendations on mechanical prophylaxis, and provide guidance regarding the role of antithrombotic therapy in hemorrhagic stroke.
Conclusions
Venous thromboembolism after stroke is common and contributes to increased morbidity and mortality, though recent improvements in post-stroke care have reduced its incidence. Intermittent pneumatic compression devices have shown to prevent DVT in small trials underpowered to detect PE. Intermittent pneumatic compression devices are routinely used for mechanical prophylaxis and a large randomized trial investigating their efficacy is underway. Graduated compression stockings do not significantly reduce VTE and are associated with skin breakdown. Unfractionated heparin, LMWH, and danaparoid are acceptable options for chemoprophylaxis, though all are associated with an increased risk of bleeding complications.
No pharmacotherapy has been clearly demonstrated as being clinically superior. Though 2 trials have demonstrated superior efficacy for enoxaparin and danaparoid over UFH in the reduction of VTE, the clinical implications of these trials are less clear. The dose of enoxaparin (40 mg) used in the PREVAIL trial and danaparoid 750 IU bid in the study by Turpie et al represent greater anticoagulant activity than the 5000 IU bid of UFH against which they were compared; both the enoxaparin and danaparoid groups experienced a higher rate of major hemorrhage. Additionally, danaparoid demonstrated no difference in preventing proximal DVT, which is more likely to be clinically evident and carries a higher risk of morbidity and mortality.
Cost may have an impact on the choice of agent: UFH is cheaper but requires twice daily dosing and has a greater potential for side effects. Once-daily dosing of LMWH may be preferable due to reduction in nursing time and patients may prefer 1 needle per day rather than 2.
The role of newer anticoagulants in VTE prophylaxis will need to be clarified by dedicated clinical trials. Hemorrhagic stroke is associated with a higher rate of VTE than ischemic stroke and presents a particular challenge in balancing the benefits of prophylaxis with its risk of iatrogenic hemorrhage. Preliminary evidence suggests that anticoagulation after 24 hours of ICH is well tolerated. Further studies are warranted with regard to chemoprophylaxis in ICH and SAH.
Footnotes
Acknowledgments
We thank the reviewers for their helpful suggestions.
MDH holds the Heart & Stroke Foundation of Alberta, NWT, NU Professorship in Stroke Research and is an Alberta Innovates-Health Solutions Scholar. TSF conducted the background literature search and primarily wrote the manuscript. MDH provided guidance on structure and content and edited the manuscript.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MDH has been funded by the Heart & Stroke Foundation of Alberta, Northwest Territories and Nunavut and by Alberta Innovates Health Solutions. The authors did not receive specific funding for this publication.