
Abstract
CHADS2 and CHA2DS2-VASc scores have been used to assess the prognostic risk of thromboembolism in non-valvular atrial fibrillation patients. Recent studies have shown the utility of CHADS2 and CHA2DS2-VASc scores for evaluating the severity of coronary artery disease (CAD). The newly defined CHA2DS2-VASc-HSF score evaluates atherosclerosis and is associated with CAD severity. This study investigated the association between the CHA2DS2-VASc-HSF score and acute coronary syndrome (ACS) severity as assessed by the Gensini score and the number of vessels. Furthermore, this study also compared the diagnostic value of the CHADS2, CHA2 DS2-VASc, and CHA2DS2-VASc-HSF score for ACS. A total of 2367 eligible inpatients (ACS group [n = 2030]; non-CAD group [n = 337]) were consecutively enrolled in this study. Receiver operating characteristic curve diagnostic tests and logistic regression models were used to analyze the risk factors for ACS. The CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were significantly higher in the ACS group than those in the control group. After adjusting for numerous traditional CAD risk factors, an increased CHA2DS2-VASc-HSF score was found to be an independent risk factor for patients with ACS (odds ratio 1.401, 95% confidence interval 1.044, −1.879; P < 0.05). A newly diagnosed CHA2DS2-VASc-HSF score predicts the severity of ACS.
Coronary artery disease (CAD) is responsible for one-third of the total deaths in people older than 35. 1 As a type of CAD, acute coronary syndrome (ACS) is the leading cause of death worldwide, comprising a group of conditions that include ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), 2 and unstable angina. The most common cause of ACS is occlusion of a coronary vessel secondary to the disruption of an atherosclerotic plaque with subsequent thrombus formation. 3 CHA2DS2 and CHA2DS2-VASc score models are widely used to predict the risk of subsequent thromboembolic events in patients with atrial fibrillation (AF) and include similar risk factors for the development of CAD.4,5 Recent evidence has shown that the CHADS2 score has prognostic ability in CAD,6,7 regardless of the presence of AF, 8 and has suggested the power of CHADS2 and CHA2DS2-VA to assess major adverse cardiovascular outcomes in the setting of ACS. 9 Moreover, a retrospective study found that the CHA2DS2-VASc score was associated with a higher risk of in-hospital mortality rates in patients who underwent primary percutaneous coronary intervention (PCI) for STEMI. 10 We formulated a new score, the CHA2DS2-VASc-HSF, which includes the variables hyperlipidemia (H), smoking (S), and family history of CAD (F), in addition to the previous risk factors to assess the risk of CAD (Table 1). 11 We sought to evaluate the ability of this new score to independently predict ACS and compared its predictive ability to that of the CHA2DS2 and CHA2DS2-VASc scores in patients with ACS with multiple vessels.
CHADS2-VASc-HSF score.

CAD: coronary artery disease
Methods
A total of 2030 inpatients with ACS (case group) and 337 non-CAD inpatients (control group) were consecutively enrolled in this retrospective study in the Department of Cardiology at the Affiliated Hospital of Chengde Medical University, from December 2015 to May 2019. All patients were subjected to diagnostic coronary angiography (CAG). ACS patients included those with unstable angina, non-STEMI, STEMI, and CAG showing stenosis of ≥50% in the left main, left anterior descending, left circumflex, right coronary, and/or their main branches. Patients with a history of coronary artery bypass graft surgery, infectious or inflammatory disease, severe liver or renal disease, neoplasm, or hematological disorders were excluded. The Gensini score was used to assess the degree of coronary stenosis in all angiograms, and the CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were calculated. The study complied with the Declaration of Helsinki, and the protocol was approved by the institutional ethics committee of the Affiliated Hospital of Cheng de Medical University(Number:CYFYLL2021174).Demographic characteristics and clinical data of all patients, including age, gender, hypertension 12 (defined as measurements of systolic blood pressure [SBP] and diastolic blood pressure [DBP] ≥140/90 mm Hg or taking antihypertensive medications), diabetes mellitus 13 (defined as a fasting blood glucose level >126 mg/dL, blood glucose ≥200 mg/dL, or using antidiabetic drugs), hyperlipidemia 14 (defined as increased level of low-density lipoprotein cholesterol [LDL-C] according to the National Cholesterol Education Program-3 recommendations and history of using lipid lowering medications), previous ischemic stroke or transient ischemic attack (TIA), vascular disease (defined as myocardial infarction [MI] and peripheral artery disease, including prior revascularization, angiographic evidence, or aortic plaque), chronic heart failure (CHF) (defined signs/symptoms of heart failure confirmed with objective evidence of cardiac dysfunction), smoking status 15 (defined as smoking >10 cigarettes a day for ≥1 year without a quit attempt), and family history of CAD (defined as MI before 55 years of age for men or 65 years of age for women in first-degree relatives).
For each patient, SBP, DBP, ejection fraction (EF), left atrial diameter, left ventricular end-diastolic dimension (LVEDD), left ventricular end-systolic diameter (LVESD), white blood cell (WBC) count, total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), LDL-C, uric acid (UA), blood urea nitrogen (BUN), and renal function test results were obtained. All participants provided written informed consent.
CAG was performed using the standard Judkins technique. CAG: the stenosis at least or more than 50% in one or more of the left main, left anterior descending, left circumfex, right coronary, or their main branches. The Gensini score is a comprehensive score that assesses the extent of CAD burden on angiography. This score is calculated as the sum of the severity scores assigned depending on the degree of angiographic luminal stenosis in each segment of the coronary artery, exponentially increasing by the severity of lesions (25%, 50%, 75%, 90%, 99%, and 100% coronary stenosis), with a cumulative effect according to multiple lesions and lesion location.
The CHADS2 nomenclature represents congestive heart failure (C), hypertension (HT), age (A), diabetes mellitus (DM), and stroke (S) and is calculated by assigning 1 point each for the presence of C, HT, A >75 years, and DM, and by assigning 2 points for history of S or TIA. The CHA2DS2-VASc score, a modification of the CHADS2 score, extends the latter by including additional common stroke risk factors, including vascular disease (V), age 65 to 74 years (A), and female sex (as a sex category [Sc]). In the CHA2DS2-VASc score, age >75 years (A2) was assigned 2 points. The CHA2DS2-VASc-HSF score (Table 1) adds hyperlipidemia (H), smoking (S), family history (F) and male gender (instead of female gender) to the previous scores. 7 The maximum CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores are 6, 9, and 12, respectively.
Statistical analyses were performed using the Statistical Package for Social Sciences software (version 26.0; SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to analyze continuous data with normal or skewed distributions. The mean ± standard deviation and quartile median are used to express normal and skewed continuous data, respectively. To investigate differences between the groups, the t-test was applied for normally distributed continuous variables, the Mann-Whitney U-test for continuous variables with abnormal distribution, and the Chi-square test for categorical variables. Regression analyses were performed to identify candidate variables among demographics, risk factors, and biomarkers. Logistic regression analysis was performed to investigate the multivariable adjusted association of CHADS2-VASc-HSF score with ACS. Statistical significance was set at a two-tailed P-value of <0.05.
Results
Both age and the proportion of males was greater in the ACS group than in the control group (both, P < 0.001). Dyslipidemia, hypertension, type 2 DM (T2DM), vascular disease, ischemic stroke, current smoker, history of MI, and history of heart failure (HF)/EF<40% were more common in the ACS group than in the control group (all P < 0.05). Similarly, the medians of heart rate, SBP, LVEDD, and LVESD were higher in the ACS group than in the control group; however, the median EF was lower in the ACS group (all P < 0.001). Moreover, the median white blood cell (WBC) count, TC, TG, and LDL-C levels were higher in the ACS group than in the control group, whereas HDL-C was higher in the control group than in the ACS group (all P < 0.05). In addition, the prevalence rate of family history of CAD was higher in the ACS group than in the control group, but the difference was not statistically significant (P > 0.05). Interestingly, the CHADS2,CHA2DS2-VASc, and CHADS2-VASc-HSF scores were significantly higher in the ACS group than in the control group (all P < 0.05) (Table 2).
Baseline characteristics and laboratory measurements of patients.

CAD: coronary artery disease; DBP: diastolic blood pressure; EF: ejection fraction; HDL-C: high-density lipoprotein-cholesterol; HF: heart failure; HR: heart rate; LA: left atrial; LDL-C: low-density lipoprotein-cholesterol; LVEDD: left ventricular end-diastolic dimension; LVESD: left ventricular end-systolic diameter; SBP: systolic blood pressure; TC: total cholesterol; TG: triglycerides; T2DM: type 2 diabetes mellitus; WBC: white blood cell
The diagnostic test analysis showed that in the ACS and control subgroups, the area under the curve (AUC) of the CHADS2 score, CHA2DS2-VASc score and CHADS2-VASc-HSF score were 0.593, 0.538, and 0.692, respectively; the optimal diagnostic cut-off point values were 1.5, 2.5, and 2.5, respectively; the sensitivity was 30.8%, 25.8%, and 76.8%, respectively; and the specificities were 83.7%, 82.5%, and 51.6%, respectively (Table 3).
Receiver operator characteristic curves of the CHADS2 score, CHA2DS2-VASc score and CHA2DS2-VASc-HSF score value for prediction of acute coronary syndrome.

AUC: area under the curve; CI: confidence interval; SE :standard error;Se: sensitivity; Sp: specificity
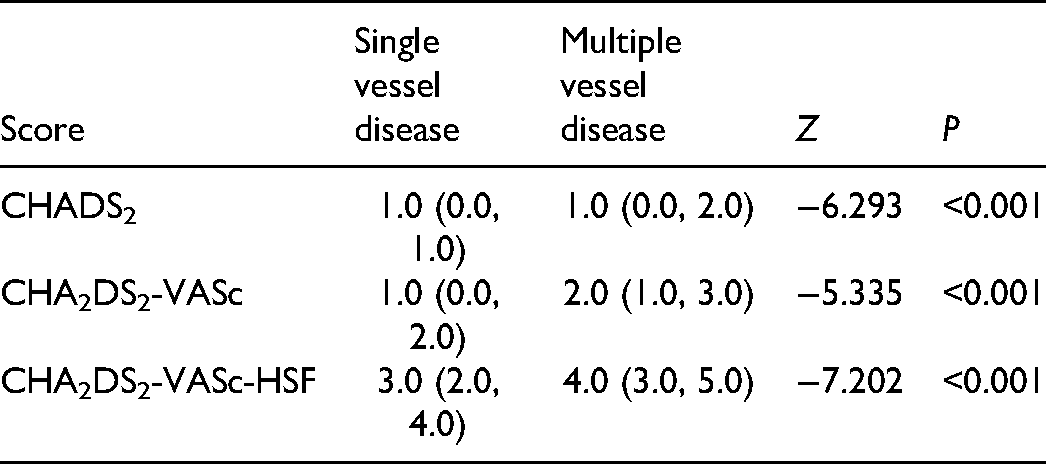
The median CHADS2,CHA2DS2-VASc, and CHADS2-VASc-HSF scores were significantly higher in the multiple vessel disease group than in the single-vessel group (all P < 0.001) (Table 4).
Comparison of CHADS2 score, CHA2DS2-VASc score and CHA2DS2-VASc-HSF score and number of diseased vessels.
Multivariate logistic regression mode l showed that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and CHA2DS2 score were independent risk factors for ACS, and the odds ratios (ORs) of these factors were 3.781 (2.928, 4.883), 2.058 (1.583, 2.675), 2.029 (1.317, 3.125), 2.095 (1.629, 2.695), 2.231 (1.382, 3.602), 2.800 (1.826, 4.292), and 1.573 (1.085, 2.279), respectively (all P < 0.05). Mode 2 revealed that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and CHA2DS2-VASc score were independent risk factors of ACS, and the ORs of these factors were 4.241 (3.238, 5.556), 1.899 (1.445, 2.496), 2.171 (1.456, 3.238), 2.072 (1.610, 2.667), 2.245 (1.388, 3.631), 2.696 (1.756, 4.139), and 1.689 (1.153, 2.474), respectively (all P < 0.05). Mode 3 showed that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and the CHADS2-VASc-HSF score were independent risk factors for ACS, and the ORs of these factors were 2.890 (2.172, 3.845), 1.971 (1.515, 2.565), 2.168 (1.469, 3.200), 2.039 (1.583, 2.627), 2.060 (1.272, 3.337), 2.788(1.817, 4.276), and 1.751 (1.319, 2.324), respectively (all P < 0.05) (Table 5).
Results of the multivariate regression analyses for the predictors of acute coronary syndrome.

CI: confidence interval; EF: ejection fraction; LDL: low-density lipoprotein; OR: odds ratio; SBP: systolic blood pressure; T2DM: type 2 diabetes mellitus
Multivariate logistic regression mode l showed that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and the CHA2DS2 score were independent risk factors for a high Gensini score, with ORs of 3.082 (2.468, 3.849), 1.794(1.436, 2.242), 1.429 (1.018, 2.006), 2.025 (1.635, 2.507), 2.012 (1.368, 2.959), 2.589 (1.844, 3.635), and 1.661 (1.219, 2.263), respectively (all P < 0.05). Mode 2 reflected that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and the CHA2DS2-VASc score were independent risk factors for a high Gensini score, and the ORs of these factors were 3.473 (2.735, 4.410), 1.692 (1.342, 2.133), 1.616 (1.186, 2.202), 2.016 (1.628, 2.497), 2.002 (1.360, 2.946), 2.496 (1.776, 3.507), and 1.630 (1.179, 2.255), respectively (all P < 0.05). Mode 3 indicated that male sex, age ≥60 years, T2DM, SBP ≥140, LDL ≥3.4, EF <50%, and the CHADS2-VASc-HSF score were independent risk factors of a high Gensini score, and the ORs of these factors were 2.499 (1.952, 3.200), 1.780 (1.424, 2.225), 1.658 (1.227, 2.241), 1.998 (1.613, 2.476), 1.861 (1.263, 2.740), 2.577(1.835, 3.619), and 1.553 (1.212, 1.991), respectively (all P < 0.05) (Table 6).
Predictors of Gensini score in multivariate analyses.

CI: confidence interval; EF: ejection fraction; LDL: low-density lipoprotein; OR: odds ratio; SBP: systolic blood pressure; T2DM: type 2 diabetes mellitus
Table 7 manifests the results of multivariate logistic regression for the association of the CHADS2-VASc-HSF score among multiple vessels. There were 7 models after adjusting for age, sex, dyslipidemia, hypertension, T2DM, vascular disease, current smoking, history of HF, history of kidney failure, cardiogenic shock, family history of CAD, alcohol abuse, heart rate, ventricular EF, elevated SBP, WBC count, BUN, creatinine level, UA level, elevated fasting glucose, reduced HDL-C, elevated TG, TC, and LDL-C. The ORs were 1.879, 1.363, 1.504, 1.369, 1.345, 1.376, and 1.360 for ACS with multiple vessels in models 1, 2, 3, 4, 5, 6, and 7, respectively (all P < 0.05) (Table 7).
Logistic Regression model of CHA2DS2-VASc-HSF score in the acute coronary syndrome subgroup with multiple vessels.

Model 1: adjusted for age≥60, sex
Model 2: adjusted for dyslipidemia, hypertension,T2DM, vascular disease (prior myocardial infarction/peripheral artery disease/aortic calcification) + Model 1
Model 3: adjusted for dyslipidemia, hypertension, vascular disease (prior myocardial infarction/peripheral artery disease/aortic calcification), current smoker + Model 1
Model 4: adjusted for history of heart failure, history of kidney failure, cardiogenic shock, and family history of CAD + Model 2
Model 5: adjusted for SBP ≥140 mm Hg, HR ≥100 bpm and EF <50% + Model 4
Model 6: adjusted for white blood cell count >10*1012/L, BUN >7.1 mmol/L, UA >510 mmol/L, Scr >110 mmol/L, and fasting glucose >6.1 mmol/L + Model 4
Model 7: TC >5.2 mmol/L, TG >1.7 mmol/L, LDL >3.4 mmol/L and HDL <1.0 mmol/L + Model 6
BUN: blood urea nitrogen; EF: ejection fraction; HDL: high-density lipoprotein; HF: heart failure; HR: heart rate; SBP: systolic blood pressure; Scr: serum creatinine; TC: total cholesterol; TG: triglycerides; T2DM: type 2 diabetes mellitus; UA uric acid
Discussion
The main findings of this present study were as follows: (1) the CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were significantly different for various numbers of diseased vessels; (2) the CHA2DS2-VASc-HSFscore showed better predictability for patients with ACS than did the CHADS2 and CHA2DS2-VASc scores; (3) the CHA2DS2-VASc-HSF score was an independent risk factor for patients with ACS; (4) the CHA2DS2-VASc-HSF score was the best score scheme to predict ACS severity, and a score >2.5 may predict ACS severity. The results suggest that the CHA2DS2-VASc-HSF score is a comprehensive risk scoring tool for the risk stratification of patients with ACS.
In addition to predicting outcomes of patients with AF, the individual score components of the CHADS2 score are traditional risk predictors of coronary arteriosclerosis. Chan et al. previously reported an important association between the CHADS2 score and vascular endothelial function assessed by flow-mediated dilation in non-AF patients. 16 Patients with HF, HT, older age, and DM without AF have elevated markers of endothelial dysfunction and hypercoagulability,17–19 indicating that platelet activation might be attributed to underlying risk factors other than AF. Li et al. found that a higher CHADS2 score was associated with a higher risk of combined outcomes, all-cause death, and cardiovascular death in patients with CAD. 20 Chen et al. suggested that the CHA2DS2-VASc score may play a vital role in predicting MI and HF in patients without AF. 21 Furthermore, in patients who underwent primary PCI, the CHA2DS2-VASc score was shown to predict thrombus burden, 22 no-reflow phenomenon, 23 major adverse cardiac events, 24 in-hospital mortality, and long-term adverse clinical outcomes.25–27 By incorporating the majority of risk factors for CAD, the CHA2DS2-VASc-HSF score provides a comprehensive risk assessment for CAD. 11
This newly developed score has been independently associated with the severity of atherosclerosis and CIN development 28 in patients with STEMI. In line with previous reports, in our study the CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were obviously higher in the ACS group than those in the control group; the sensitivity value of the CHA2DS2-VASc-HSF score was greater than the specificity value, and the diagnostic efficiency of the CHA2DS2-VASc-HSF score in the ACS group was greater than that in the control group. The higher AUC in the CHA2DS2-VASc-HSF score (compared to that of the CHADS2 and CHA2DS2-VASc scores) indicates that it could be used as a predictive indicator for ACS. In Tabata's study, CAD patients with multivessel disease had a significantly higher CHADS2 score than those with single-vessel disease. 9 In particular, we recognize that all 3 scores were higher in multivessel disease than in single-vessel disease.
Cetin et al. showed that the CHADS2 and CHA2DS2-VASc scores correlated significantly with the Gensini score (r = 0.383 and 0.300, P < 0.001), suggesting that the CHA2DS2-VASc score reflects the severity of CAD. 15 However, our study is the first to report that the risk of elevated CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were higher in a high Gensini score group than in the low Gensini score.
Orcun et al. demonstrated that the CHA2DS2-VASc score was correlated with severe CAD by univariate analysis, but it did not independently predict severe CAD following multivariate analysis, whereas the CHA2DS2-VASc-HSF score did. 29 However, in contrast to previous studies, we demonstrated that CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores were independent risk factors for patients with ACS using multivariate logistic regression models for ACS analysis. The CHA2DS2-VASc-HSF scores differed between the ACS and control groups. Our study demonstrated that the risk of elevated CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HSF scores was greater in the ACS group than in the control group.
Zhang et al. demonstrated that the components of the 3 scores are common risk factors for atherosclerosis, vascular spasm, and microvascular dysfunction. 30 Hyperglycemia may be associated with vascular smooth muscle cell proliferation and migration, oxidative stress, a hypercoagulable state, and the inflammatory response, which contribute to CAD. 31 Dyslipidemia also contributes to cerebrovascular and cardiovascular disorders, which are considered in the CHA2DS2-VASc model. 32 In addition, male patients are more likely to smoke and suffer from obesity than female patients.30 Compared with the CHADS2 and CHA2DS2-VASc scores, the CHA2DS2-VASc-HSF score provided similar discrimination for ACS. After adjusting these factors and other traditional CAD factors, we consider that the CHA2DS2-VASc-HSF score remains a significant predictor for patients with ACS in multiple vessels, even following a multivariate analysis for traditional CAD characteristics, further supporting our hypothesis.
Our study had several limitations. First, this was a single-center study; further studies are needed to establish the value of this finding in the context of current clinical practice. Second, the sample size of patients in this study was relatively small. Third, the CHA2DS2-VASc-HSF score can be developed with other biochemical and echocardiographic predictors of atherosclerosis in further studies. Hence, a multi-regional and multi-ethnic study is needed in the future.
In summary, the CHA2DS2-VASC-HSF score may be convenient and easily applied in clinical practice, and it can be used to assess high-risk patients and prepare therapeutic interventions.
Footnotes
Acknowledgements
We are grateful for the assistance of doctors and technicians in the division of radiology, The Affiliated Hospital of Chengde Medical University.
Author Contributions
JY. L. contributed to the conception and design of the study, the acquisition, analysis, and interpretation of the data, and the drafting of the manuscript.Y.M., HW.B.,W.Q.and F.S. contributed to the acquisition of the data. Y.Z. contributed to the critical revision of the manuscript for important intellectual content. All authors approved the final version of the manuscript for publication.
Authors' Note
Ethical approval was obtained from the Institutional Review Board of The Affiliated Hospital of Chengde Medical University (Number: CYFYLL2021174). Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.