
Abstract
Lipoprotein-associated phospholipase A2 (Lp-PLA2) is an independent risk factor for cardiovascular disease. Accordingly, studies from many countries around the world have shown an association between Lp-PLA2 and cardiovascular events in patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI), but this association has not been documented among the Chinese. The aim of this study was to assess the use of Lp-PLA2 as a useful marker for predicting the long-term prognosis of Chinese patients with ACS undergoing PCI. A total of 651 consecutive patients undergoing PCI between September 2013 and January 2015 were divided into 2 groups: the high Lp-PLA2 group (n = 262, Lp-PLA2 > 138 nmol/L) and the low Lp-PLA2 group (n = 389, Lp-PLA2 ≤ 138 nmol/L). The end point was all-cause mortality and rehospitalization. The median follow-up was 24 months. Multivariate analysis showed that high Lp-PLA2 was an independent predictor of all-cause mortality and rehospitalization (hazard ratio: 1.429, 95% confidence interval [CI]: 1.411-1.448; P < .05). The Lp-PLA2 had good accuracy for predicting all-cause mortality and rehospitalization among patients with ACS undergoing PCI (area under the receiver–operating characteristic curve: 0.858, 95% CI: 0.819-0.898; P < .05), and a good correlation with the Global Registry of Acute Coronary Event score (r = 0.525, P < .05). This study provided evidence that Lp-PLA2 could predict all-cause mortality and rehospitalization risk among patients with ACS undergoing PCI.
Introduction
Cardiovascular disease is the leading cause of death globally. The major pathogenic mechanisms are atherosclerosis and thrombosis, in which inflammation plays a key role. 1 Accordingly, inflammation-based markers have been used to distinguish between patients and prognosticate based on risk profiles. Lipoprotein-associated phospholipase A2 (Lp-PLA2) is one of these markers that has come to be associated with a higher incidence of cardiovascular events and is a potential pathogenic factor participating in the progression of atherosclerosis. 2 Moreover, an increased Lp-PLA2 is associated with coronary heart disease and ischemic stroke. 3 –5 However, there is a scarcity of data regarding the relationship of Lp-PLA2, coronary heart disease, and mortality in China. Besides Lp-PLA2, other laboratory variables, such as mean platelet volume (MPV), platelet distribution width (PDW), serum uric acid (SUA), and red blood cell distribution width (RDW), have also been associated with coronary heart disease. 6 –10 The Global Registry of Acute Coronary Event (GRACE) risk stratification, as a clinical scoring system, can help us identify patients in high risk. 11,12 However, GRACE score is based on several clinical and laboratory variables that limit its use. Thus, it is necessary to find effective and easily obtainable biomarkers for predicting the prognosis of patients with acute coronary syndrome (ACS). Therefore, the aim of this study was to assess Lp-PLA2 an effective marker for predicting the long-term prognosis of Chinese patients with ACS undergoing percutaneous coronary intervention (PCI).
Methods
This study was a prospective study among all patients with ACS who were hospitalized and underwent PCI at the Affiliated Hospital of Chengde Medical College. A total of 651 patients were selected between September 2013 and January 2015 in this large-scale hospital study in Northwest China. Initially, all consecutive patients undergoing PCI were identified from Picture Archiving and Communication Systems and were assigned a unique study ID. Then, patients’ information were recorded, including demographic and clinical characteristics, and laboratory measurements. Additionally, each patient was mandated to sign an informed consent agreement before enrollment, and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. Left ventricular ejection fraction was measured by echocardiography using the biplane method of discs during hospitalization. 13 A computer analysis system was used to estimate the angiographic characteristics, while thrombolysis in myocardial infarction (TIMI) flow grade was determined as previously defined. 14 The GRACE score was calculated at admission, and only patients with intact GRACE score variables were enrolled in the present study. All other events were obtained from the patients’ medical records and from the patients by telephone interview and/or outpatient clinic visits. All patients were followed up for a mean duration of 24 months.
All cases underwent blood testing and clinical examination, during which blood samples were taken from a peripheral vein after an overnight fast for the measurement of laboratory variables including MPV, PDW, SUA, RDW, triglyceride, low-density lipoprotein, high-density lipoprotein, lipoprotein(a), and lipoprotein(b). Blood samples for the measurement of Lp-PLA2 were taken from a peripheral artery before coronary angiography, and the nonheparinized blood serum was segregated and stored at −80°C for further detection. The Lp-PLA2 was detected by enzyme-linked immunosorbent assay.
According to current guidelines, unstable angina patients were identified based on ischemic symptoms suggestive of ACS without electrocardiogram changes indicating ischemia. Thus, non-ST-elevation myocardial infarction (NSTE-MI) was defined as no ST elevation in electrocardiograms but with an increase in cardiac ischemia markers, while STE-MI was defined as patients with typical ischemic chest pain lasting more than 20 minutes along with 1 of the following criteria: at least 1 mm ST elevation, the elevation of cardiac markers at least twice the maximum normal values. After confirmation of ACS, PCI was undertaken according to current guideline recommendation. The use of aspiration thrombectomy, heparin, or glycoprotein IIb/IIIa inhibitor was decided by the operators. All patients received standard care according to the current guidelines. 12,15 Exclusion criteria included (1) coronary artery bypass grafting, (2) active infection, (3) hematological disorders, (4) severe liver or renal disease, (5) autoimmune disease or steroid therapy, and (6) no blood sample before coronary angiography or unavailability of GRACE score.
The clinical end points were defined as the composite of all-cause mortality and rehospitalization during the follow-up period. All end points were based on standardized definitions. 16
Statistical analyses for this study are as follows: Quantitative variables with normal distribution were expressed as mean (standard deviation), and those with nonnormal distribution were expressed as median (interquartile range). Comparisons of parametric values were done by independent sample t test, while comparisons of nonparametric values were done using Mann-Whitney U test. Categorical variables were represented as counts and percentages (%) and were compared by the χ2 test or Fisher exact test. Correlation analyses of 2 quantitative variables with normal distribution were performed by linear correlation, while coefficient of correlation was expressed using Pearson and other correlation between variables was expressed by Spearman. In addition, multiple regression and logistic regression were used to identify independent predictors of high-risk patients. Kaplan-Meier was used to analyze the univariate effect on event-free survival and was tested by log rank (P < .05). Cox proportional hazards regression modeling was used to analyze the multivariate effect of variables on event-free survival. The variables that showed significance in univariate analysis (P < .05) and other variables known to affect prognosis after ACS were “entered” into the model. Results were expressed as hazard ratios (HRs) with associated 95% confidence intervals (CIs). The area under the receiver–operating characteristic curve (ROC-AUC) was used to assess the predictive value and calculate the cutoff of Lp-PLA2. All tests were 2 sided, and the statistical significance was defined as P < .05. All statistical analyses were performed using SPSS version 19 (SPSS Inc, Chicago, Illinois).
Results
Baseline clinical characteristics of the population (n = 651), among whom 262 had high Lp-PLA2 while 389 had low Lp-PLA2, are listed in Table 1. Patients with high Lp-PLA2 had significantly higher GRACE scores than those with low Lp-PLA2 (Table 1). The rates of TIMI flow grade 0/1 before PCI use of glycoprotein IIb/IIIa inhibitor were found to be significantly higher in the high Lp-PLA2 group (Table 1). Subsequently, using Pearson or Spearman correlation coefficient, we estimated the correlation of Lp-PLA2 with clinical characteristics and found a significant correlation between Lp-PLA2 and GRACE score (r = 0.525, P < .05; Table 2).
Baseline Clinical Characteristics.
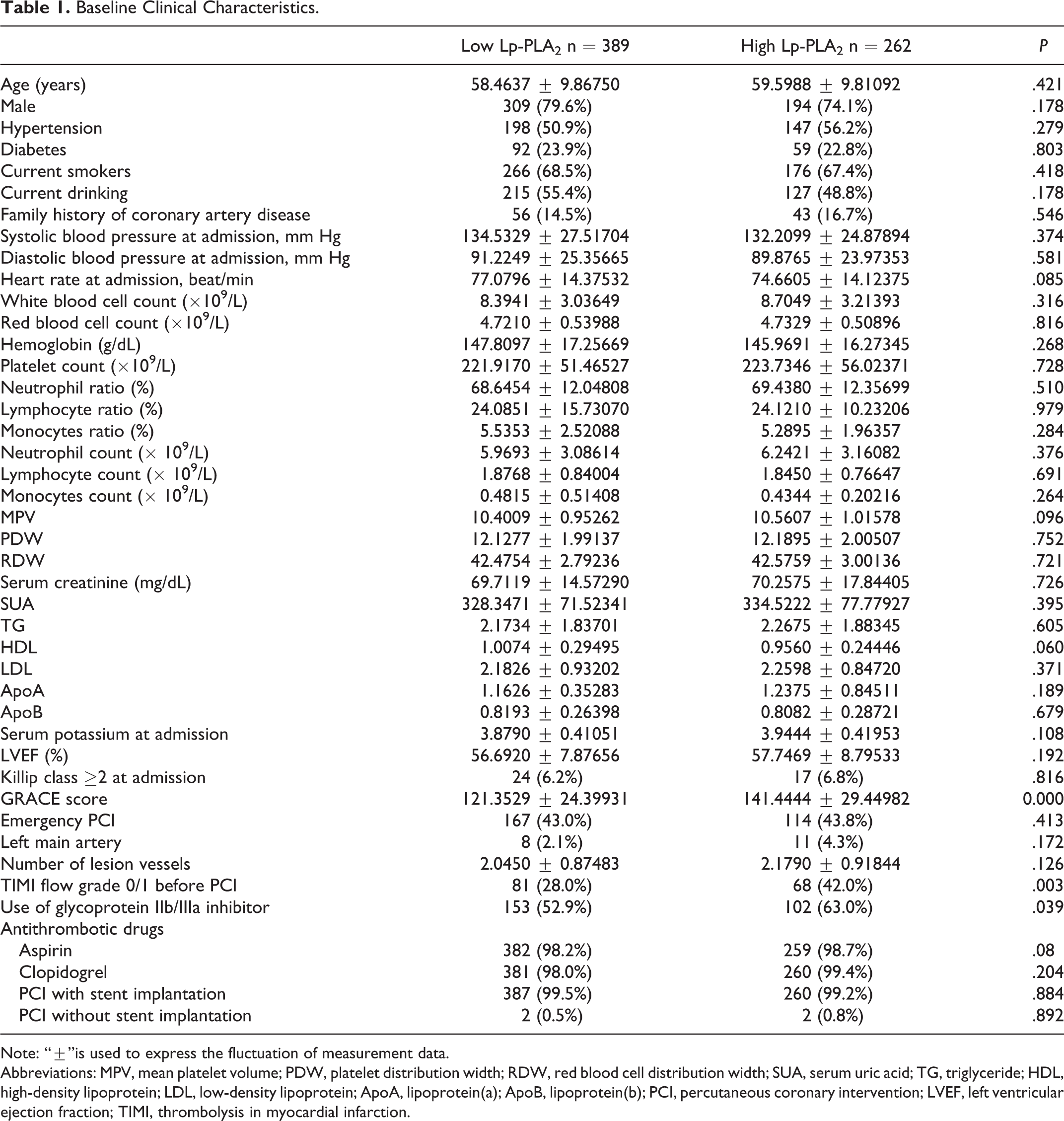
Note: “±”is used to express the fluctuation of measurement data.
Abbreviations: MPV, mean platelet volume; PDW, platelet distribution width; RDW, red blood cell distribution width; SUA, serum uric acid; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ApoA, lipoprotein(a); ApoB, lipoprotein(b); PCI, percutaneous coronary intervention; LVEF, left ventricular ejection fraction; TIMI, thrombolysis in myocardial infarction.
Correlation Analyses of Lp-PLA2 Levels With Other Variables.
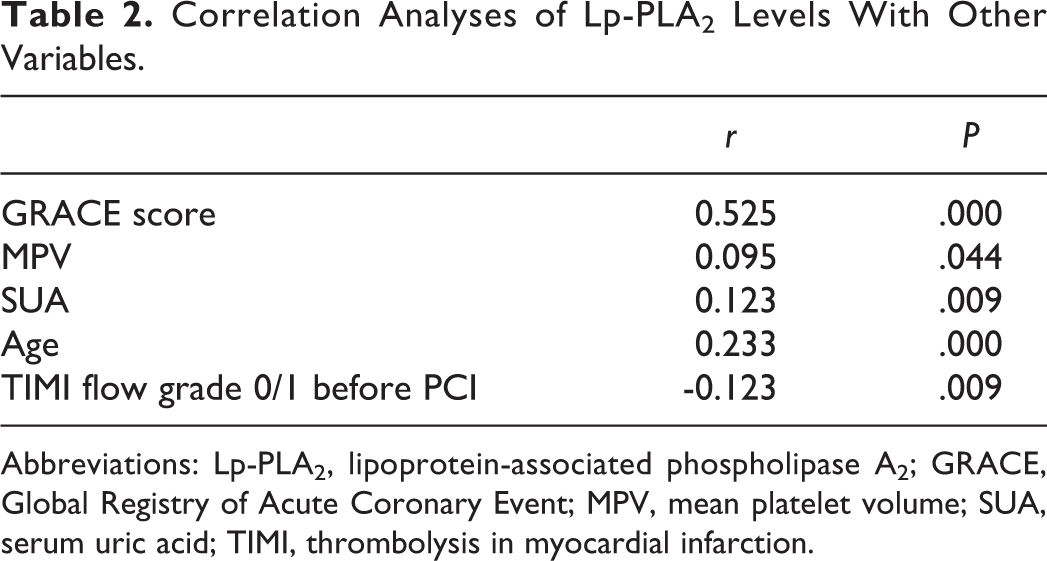
Abbreviations: Lp-PLA2, lipoprotein-associated phospholipase A2; GRACE, Global Registry of Acute Coronary Event; MPV, mean platelet volume; SUA, serum uric acid; TIMI, thrombolysis in myocardial infarction.
Logistic regression was used to detect the independent risk factors for cardiovascular events in patients with ACS after PCI. After multivariate analysis, in addition to the GRACE score, MPV, and Killip class ≥2 at admission (P < .05), Lp-PLA2 was found to be an independent risk factor (odds ratio: 1.429, 95% CI: 1.411-1.448; P < .05; Table 3).
Multivariate Logistic Regression Analysis to Identify the Independent Predictors of Cardiovascular Events.
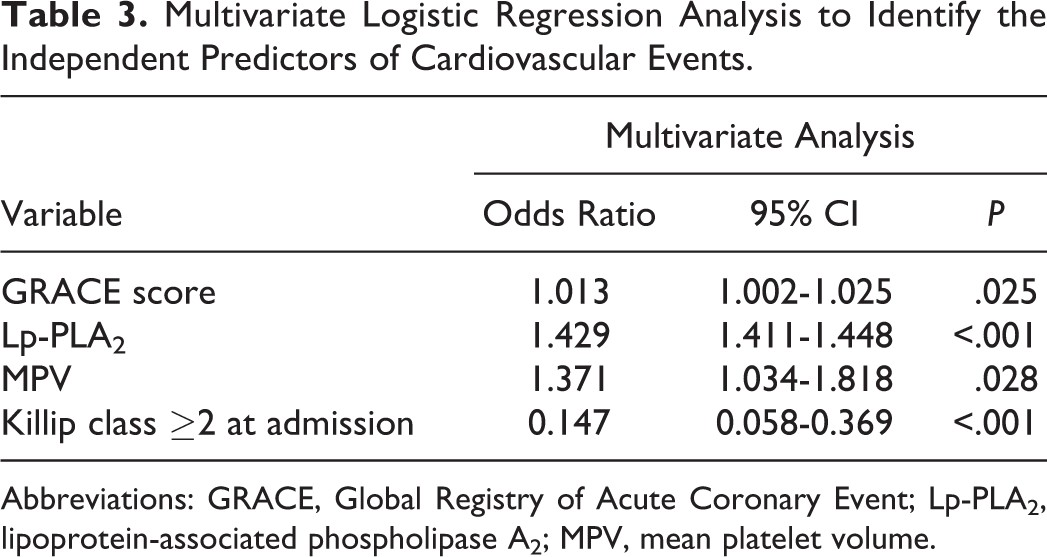
Abbreviations: GRACE, Global Registry of Acute Coronary Event; Lp-PLA2, lipoprotein-associated phospholipase A2; MPV, mean platelet volume.
The ROC curve analysis was used to assess predictive value of variables. The results demonstrated that Lp-PLA2 (AUC: 0.858, 95% CI: 0.819-0.898; P < .05), GRACE score (AUC: 0.683, 95% CI: 0.628-0.738; P < .05), MPV (AUC: 0.583, 95% CI: 0.525-0.641; P < .05), and age (AUC: 0.580, 95% CI: 0.523-0.636; P < .05) were significant for prognostication. Furthermore, the ROC curve analysis was used to determine the cutoff value of Lp-PLA2 to predict cardiovascular events, which was found to be 43.4, with 75.5% sensitivity and 87.0% specificity (Figure 1).
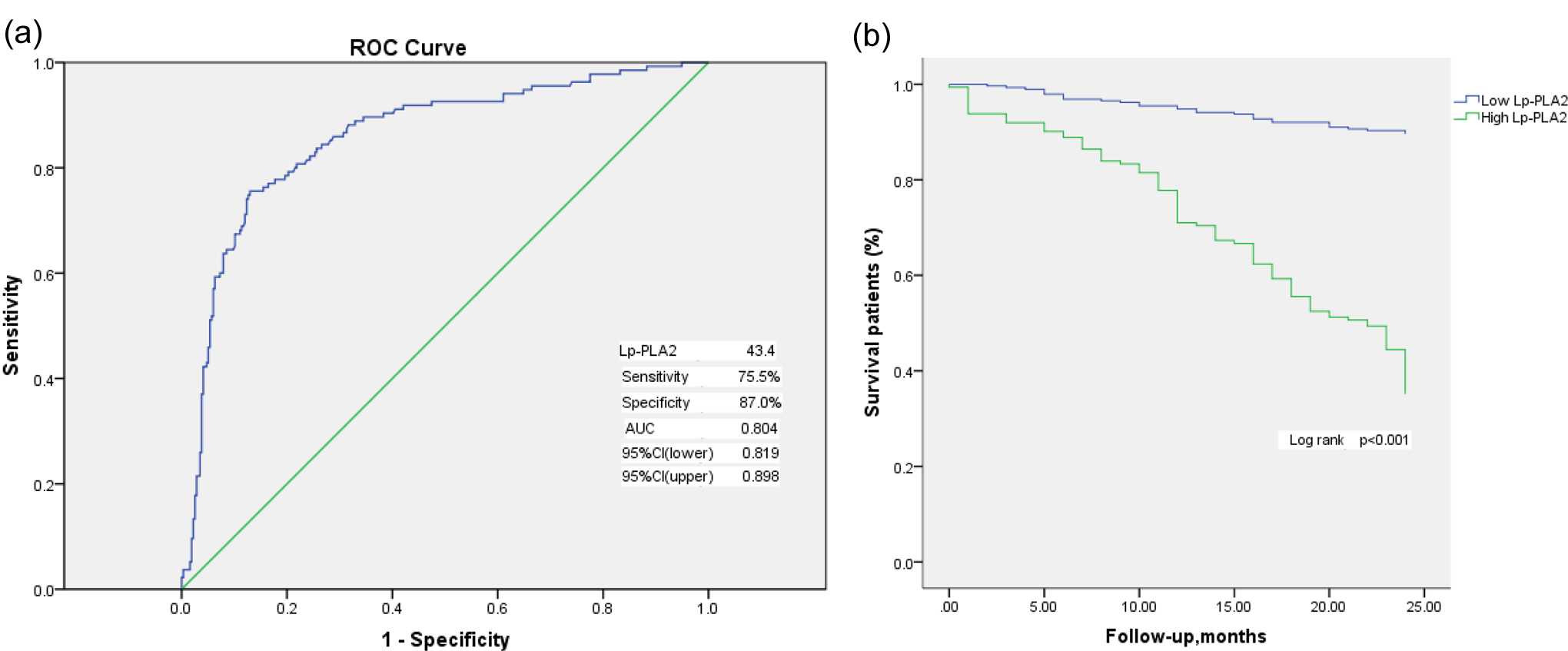
Receiver–operating characteristic curve.
In the overall study population, univariate Kaplan-Meier survival analysis indicated that Lp-PLA2 (HR: 1.332, 95% CI: 1.326-1.337; P < .05; Figure 1(b)) GRACE score (HR: 1.016, 95% CI: 1.011-1.021; P < .05), MPV (HR: 1.280, 95% CI: 1.089-1.506; P < .05), age (HR: 1.023, 95% CI: 1.005-1.041; P < .05), number of lesion vessels (HR: 1.356, 95% CI: 1.118-1.643; P < .05), and Killip class ≥2 at admission (HR: 0.389, 95% CI: 0.237-0.639, P < .05) were associated with greater cardiovascular events. Similarly, multivariate Cox proportional regression analyses (Table 4) showed that the major factors associated with increased cardiovascular events were Lp-PLA2 (HR: 1.329, 95% CI: 1.323-1.335; P < .05), GRACE score (HR: 1.007, 95% CI: 1.002-1.012; P < .05), and Killip class ≥2 at admission (HR: 0.436, 95% CI: 0.250-0.761; P < .05).
Variables Associated With Cardiovascular Events in Patients With ACS Under PCI From Kaplan-Meier and Cox Proportional Regression Analysis.
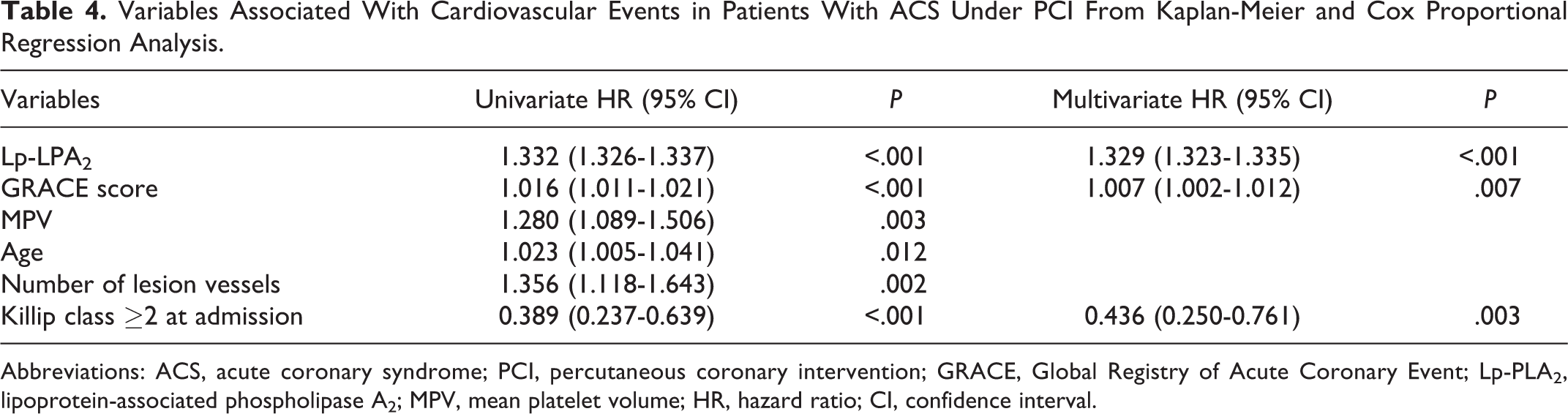
Abbreviations: ACS, acute coronary syndrome; PCI, percutaneous coronary intervention; GRACE, Global Registry of Acute Coronary Event; Lp-PLA2, lipoprotein-associated phospholipase A2; MPV, mean platelet volume; HR, hazard ratio; CI, confidence interval.
Discussion
In the present study, we tested the predictive value of Lp-PLA2 on the long-term prognosis of Chinese patients with ACS undergoing PCI. The main findings were as follows: (1) high Lp-PLA2 was an independent predictor of all-cause mortality and rehospitalization among Chinese patients, (2) Lp-PLA2 had good accuracy for predicting all-cause mortality and rehospitalization in Chinese patients with ACS undergoing PCI, and (3) Lp-PLA2 had a good correlation with GRACE score among these patients.
Coronary artery disease is the most prevalent manifestation of cardiovascular disease. It is necessary to distinguish the high-risk patients and take effective measures to reduce the associated mortality and improve cardiac function. The Lp-PLA2, encoded by the PLA2G7 gene, hydrolyzes oxidized phosphatidylcholine to release oxidized nonesterified fatty acid lysophosphatidylcholine. Elevated Lp-PLA2 has been proposed as a specific indicator of cardiovascular events. 17,18 Our study was in good agreement with other reports that have shown that high Lp-PLA2 was an independent predictor of all-cause mortality and rehospitalization. Additionally, GRACE score plays an important role in helping doctors recognize high-risk patients and take active measures to reduce cardiovascular disease. 19 In this study, our analysis showed that Lp-PLA2 had a significant correlation with GRACE score. The ROC curve analysis indicated that Lp-PLA2 was a good factor (AUC: 0.858) for predicting all-cause mortality and rehospitalization in Chinese patients with ACS undergoing PCI. The MPV is a link between thrombosis and inflammation, which reflects thrombogenesis and active platelets. Many observations had noted that MPV was a strong and independent predictor of mortality in patients with ACS. 20 However, some analysis confirmed that a higher baseline platelet count was a predictor of adverse prognosis or had no significant association in patients undergoing PCI. 21,22 Conversely, in our study, Kaplan-Meier curve showed that MPV (HR: 1.280, 95% CI: 1.089-1.506, P = .003) was associated with cardiovascular events in patients with ACS under PCI, but it was excluded from the Cox proportional regression analysis.
Furthermore, in our study, Lp-PLA2 was shown to have significant correlation with variables associated with cardiovascular disease including GRACE score, MPV, SUA, and age, and had good performance for predicting all-cause mortality and rehospitalization in patients with ACS undergoing PCI. In aggregate, considering the results presented, it is worth emphasizing the prognostic value of Lp-PLA2 in Chinese patients with ACS undergoing PCI.
Limitations
This clinical study had several limitations. First, our study was a single-center observational study, with potential confounders and selection bias that may not have been completely adjusted for. Second, there was a lack of data about the history of antiplatelet drugs use. In addition, not all of the rehospitalization patients underwent coronary angiography.
Conclusion
The Lp-PLA2 could predict all-cause mortality and rehospitalization in Chinese patients with ACS undergoing PCI and had a significant correlation with GRACE score.
Footnotes
Author’s Note
The authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Acknowledgment
All the authors who contributed toward this study met the criteria for authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.