
Abstract
Carotid and vertebral artery dissections are estimated to account for ∼20% of strokes in patients under 45-years-old. This meta-analysis compared the efficacy and safety of treatment with anticoagulants versus antiplatelet agents to determine the optimal therapy. We searched 4 electronic databases for clinical trials published from January 1, 1980 to August 25, 2021 that included patients who received anticoagulant or antiplatelet therapy for carotid and/or vertebral artery dissections. The curative effect was judged by recanalization evaluated by imaging. The primary outcomes were all cause death and ischemic stroke; secondary outcomes included hemorrhage and transient ischemic attack (TIA). Patients who received only a single drug treatment were divided into antiplatelet or anticoagulant groups; all received conservative treatment without surgical intervention. For this investigation, we pooled the available studies to conduct a meta-analysis, which included 7 articles with 1126 patients. The curative effect of vascular recanalization was not significantly different between the 2 treatment groups (odds ratio [OR] = 0.913, 95% confidence interval [CI]: 0.611-1.365, P = .657); similarly, no significant differences were found regarding the primary outcomes all cause death (OR = 1.747, 95%CI: 0.202-15.079, P = .612) and ischemic stroke (OR = 2.289, 95%CI: 0.997-5.254, P = .051). Patients treated with anticoagulants were more likely to experience TIA (OR = 0.517, 95%CI: 0.252-1.060, P = .072) and hemorrhage (OR = 0.468, 95%CI: 0.210-1.042, P = .063), but the differences were not statistically significant. Overall, there were no statistically significant differences between anticoagulant therapy and antiplatelet therapy for the treatment of carotid and vertebral artery dissections.
Introduction
Cervical artery dissection is one of the most common causes of strokes, accounting for ∼20% of strokes in patients under the age of 45.1,2 Among these patients, carotid artery dissection comprises 70% to 80% of cases and vertebral artery dissection accounts for 15%. 3 Cervical artery dissection has an associated mortality rate of up to 5%, with full resolution occurring in >90% of cases. 4 Many factors are related to cervical artery dissection, such as hypertension, diabetes mellitus, smoking, neck trauma, hyperlipidemia, and atherosclerosis. The pathophysiology of strokes involves endothelial damage. Disruptions to the endothelium can activate platelets and the coagulation cascade, leading to thrombus formation and distal embolization. 5 Therefore, antithrombotic therapy with either antiplatelets or anticoagulants can reduce the risk of stroke in patients with cervical artery dissection. The American Heart Association Guidelines 6 indicate that antithrombotic therapy for at least 3 to 6 months is reasonable for patients to prevent stroke or transient ischemic attack (TIA). However, the guidelines also point out that the efficacy and safety of anticoagulation and antiplatelet therapy are relatively uncertain.
The aim of this study is to compare the efficacy and safety of anticoagulation and antiplatelet therapies using meta-analysis techniques to determine the optimal treatment for cervical artery dissection. The outcomes analyzed included recanalization (imaging), all cause death, ischemic stroke, hemorrhage, and TIA.
Methods
Literature Search
We searched the PubMed, Embase, Web of Science, and Cochrane Library databases for studies published until August 25, 2021. The search employed the term(s) “Carotid and/or vertebral artery dissections,” which were combined with each of the following Boolean operators: “antiplatelet therapy,” and “anticoagulation therapy.” Abstracts of the citations identified by the search were then scrutinized by 2 investigators (Ye and Tang) to determine eligibility for inclusion in the analysis. The inclusion criteria were: (1) studies that compared anticoagulant and antiplatelet therapies; (2) comparative studies, randomized controlled trials, cohort studies, retrospective or prospective studies; (3) effective and intact clinical data; and (4) included 4 or more patients. There were no language restrictions.
We identified 7 studies that met our criteria (Figure 1). Two investigators independently extracted data utilizing a data abstraction tool: number of patients in the experimental (anticoagulant and antiplatelet) groups, study quality, time of follow-up, patients’ characteristics, curative effect, and primary and secondary outcomes. The curative effect was judged by recanalization, as defined by imaging. The primary outcomes were all cause death and ischemic stroke. The secondary outcomes measures included hemorrhage and TIA. Antithrombotic therapy (antiplatelet or anticoagulation) was defined as administration of any antiplatelet agent (acetylsalicylic acid or clopidogrel dipyridamole) or anticoagulation treatment (oral coumarin or therapeutic heparin doses). Patients who received only a single drug treatment were divided according to their initial treatment into antiplatelet or anticoagulant groups; all received conservative treatment without surgical intervention.

Flow chart of literature review.
Data Extraction and Quality Assessment
Publication details, inclusion and exclusion criteria, enrolled patient demographics, interventions used, and outcomes were collected. Risk of bias in these works (including masking of participants, methods of sequence generation and allocation concealment, intention-to-treat analysis, incomplete or unclear data, time to follow-up, and loss to follow-up) was assessed. Study quality was assessed using the Newcastle–Ottawa Scale (NOS). Any disagreements between investigators were resolved by consensus.
Statistical Analysis
Statistical analysis was performed by Stata version 13.0. We used fixed-effects models to measure the outcomes. Statistical heterogeneity was assessed by I2. The level of heterogeneity was divided into low (I2 = 25%-49%), moderate (I2 = 50%-74%), and high (I2≥75%). Outcomes were analyzed using odds ratios, with a 2-sided statistical significance level of 5%.
Results
Studies and Quality
The initial search strategy identified 45 full-text articles, and then 38 citations that were initially screened. Of these, 7 trials7-12,13 met the inclusion criteria (Figure 1). The 7 works included 1126 patients divided into anticoagulant therapy and antiplatelet therapy groups. The quality of these 7 articles, as evaluated by NOS, is shown in Table 1. Table 2 shows the baseline characteristics for participants in each trial.
The Newcastle-Ottawa Scale (NOS) for Study Quality Assessment.

Baseline Characteristics of Included Clinical Trials.

Abbreviations: AP, antiplatelet; AC, anticoagulant; TIA, transient ischemic attack; NA, not available.
Baseline Characteristics
Baseline characteristics of patients in the 2 treatment groups are shown in Table 3. The 2 groups were similar with respect to age, sex, history of TIA and stroke, hypertension, diabetes mellitus, hyperlipidemia, and smoking history. The antiplatelet group had a significantly higher proportion of patients with cardiovascular disease (antiplatelet vs anticoagulation: 10.3% vs 2.6%, P < .01); however, the number of patients with cardiovascular disease was too small to be representative. Therefore, there were no significant differences in the baseline characteristics of patients in the 2 groups.
Baseline Characteristics of the 2 Treatment Groups.
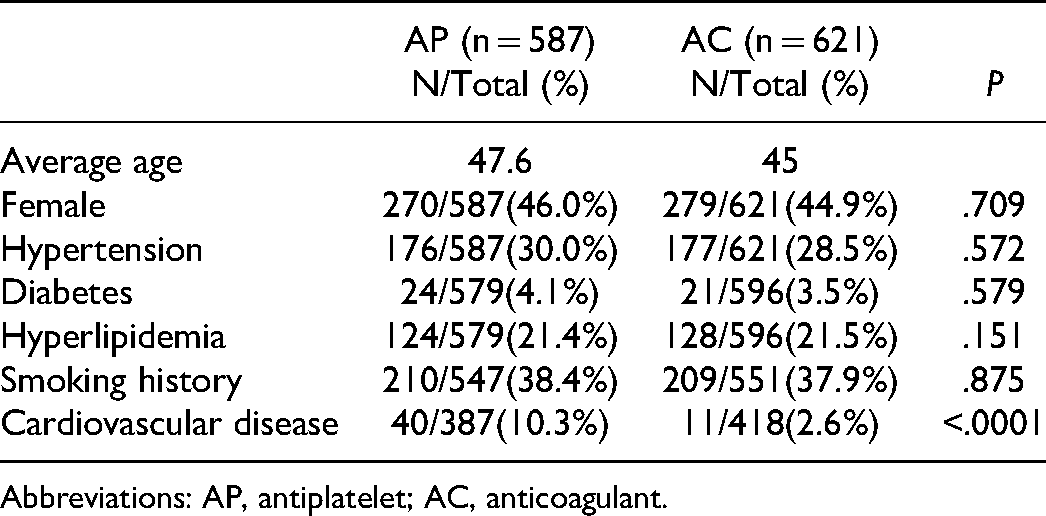
Abbreviations: AP, antiplatelet; AC, anticoagulant.
Outcomes
Primary and secondary outcomes are shown in Table 4. To investigate the efficacy of the 2 procedures, we first analyzed recanalization, which is diagnosed by an imaging examination. As shown in Figure 1, recanalization rates in the 2 treatment groups were not significantly different (odds ratio [OR] = 0.913, 95% confidence interval [CI]: 0.611-1.365, P = .657, I2 = 0.0%). However, due to the lack of imaging follow-up data for some patients, full recanalization results were not available for of all patients in these trials. Therefore, more clinical trials are required to confirm this conclusion.
Primary and Secondary Outcomes in Clinical Trials.

Abbreviations: AP, antiplatelet; AC, anticoagulant; TIA, transient ischemic attack; NA, not available.
The important complications reported in these 7 studies included all cause death, ischemic stroke, hemorrhage, and TIA. Our meta-analysis indicated that there were no differences between antiplatelet therapy and anticoagulant therapy for these complications. First, no significant differences were found in terms of the primary outcomes all cause death (OR = 1.747, 95%CI: 0.202-15.079, P = .612, I2 = 0.0%) or ischemic stroke (OR = 2.289, 95%CI: 0.997-5.254, P = .051, I2 = 0.0%). Only 3 studies mentioned all cause death; therefore, the mortality results are not representative. Additionally, the secondary outcomes TIA and hemorrhage occurred more frequently in patients treated with anticoagulation therapy, but the differences were not statistically significant (TIA: OR = 0.517, 95%CI: 0.252-1.060, P = .072, I2 = 0.0%; hemorrhage: OR = 0.468, 95%CI: 0.210-1.042, P = .063, I2 = 0.0%).

Meta-analysis of outcomes of clinical trials. (A) Meta-analysis of recanalization (OR = 0.913; 95%CI 0.611-1.365; P = .657). (B) Meta-analysis of death (OR = 1.747; 95%CI 0.202-15.079; P = .612). (C) Meta-analysis of ischemic stroke (OR = 2.289; 95%CI 0.997-5.254; P = .051). (D) Meta-analysis of hemorrhage (OR = 0.468; 95%CI 0.210-1.042; P = .063). (E) Meta-analysis of transient ischemic attack (OR = 0.517; 95%CI 0.252-1.060; P = .072).
Discussion
Carotid and vertebral artery dissections are important causes of ischemic stroke in patients <45-years-old. Embolism from thrombus formation at the dissection site plays the major role in stroke pathogenesis. 14 According to the American Heart Association Guidelines, antithrombotic therapy with either antiplatelets or anticoagulants is reasonable for patients to prevent stroke or TIA, but the efficacy and safety of both therapies are uncertain. Despite this, anticoagulant therapy is often used for stroke prevention in patients with carotid artery dissection. 15 For a long time, there was insufficient scientific evidence to support that anticoagulation therapy prevented stroke, which led to a number of randomized controlled trials, including the Warfarin-Aspirin Symptomatic Intracranial Disease Study and the Warfarin-Aspirin Recurrent Stroke Study. Both found that the benefit of warfarin for reducing stroke recurrence did not exceed that of aspirin.7,15-18 The same debate has occurred over the treatment strategy for vertebral artery dissection. Anticoagulation has been used for secondary stroke prevention despite the lack of evidence that it is superior to aspirin.
We pooled the currently available studies to conduct a meta-analysis. Based on 7 articles that included 1126 patients, we demonstrated that both the antiplatelet and anticoagulation groups had low rates of recurrent stroke; all cause death also seemed to be equally low for each treatment. On the other hand, TIA and hemorrhage occurred more frequently in patients treated with anticoagulants, but the differences were not statistically significant.
The Cervical Artery Dissection in Stroke Study (CADISS) was the first randomized controlled prospective trial to compare antiplatelet and anticoagulation treatments. 11 Among the 181 patients with confirmed dissection and complete follow-up imaging, there was no difference in the presence of residual narrowing or occlusion between patients who received antiplatelet and anticoagulation therapy. Additionally, this study showed a low rate of recurrent stroke (2.4%) and no difference between the 2 groups. Besides, the choice of antiplatelet agent was at the clinician’s discretion. In this study, ∼55% of patients received a single antiplatelet drug (either clopidogrel or aspirin) and 45% received dual antiplatelet treatment. All patients who received anticoagulation therapy were given warfarin. Expanding evidence suggests that the combination of aspirin and clopidogrel might have a greater ability to prevent early recurrent stroke risk in patients with atherosclerotic artery stenosis. It is therefore conceivable that antiplatelet therapies are more effective if all patients are given combination antiplatelet treatment. Recently, noninferiority of aspirin has not been demonstrated in the multicenter, randomized controlled trial (TREAT-CAD) comparing aspirin with vitamin K antagonists for carotid artery dissection. 13 As with CADISS, in this trial, ischemic strokes occurred numerically more often in the aspirin group and the only hemorrhage occurred in the anticoagulant group. This may be related to the fact that in the vitamin K antagonist group, patients who had received the recommended bridging with heparin or low-molecular-weight heparin in addition to a vitamin K antagonist before reaching the target INR might have had better protection against early ischemic strokes. It is important to emphasize that although aspirin was not inferior to vitamin K antagonists, these results do not mean that aspirin is inferior to anticoagulants or that vitamin K antagonists are superior to aspirin. In the study by Ramchand et al, 12 the rate of recanalization in patients with cervical arterial dissection did not differ between those treated with anticoagulants and those treated with antiplatelet therapy, and the same was true for stroke recurrence. That study also highlighted that anticoagulation therapy is used more frequently in patients with symptomatic anatomy and greater stenosis on imaging. Furthermore, in multivariate analysis, hypertension was the only important factor related to vascular recanalization, and it was closely associated with vascular recanalization failure. Moreover, hypertension was previously considered to be a risk factor for arterial dissection.19-21 Engelter et al 9 found that efficacy of anticoagulants may be higher than antiplatelets in the prevention of thromboembolic cerebral infarcts but increased the risk of hemorrhagic complications. 22 Therefore, anticoagulation therapy has the potential risk of aggravating the intramural hemorrhage, leading to an additional narrowing of the arterial lumen, which may worsen hemodynamic failure. Antiplatelets seem to be a reasonable treatment choice. Other studies have reported that both antiplatelet therapy and anticoagulation therapy have a lower incidence of complications and a higher number of patients with good clinical outcomes for all types of dissections.
In clinical practice, clinicians prefer to choose novel oral anticoagulants (NOAC) instead of traditional anticoagulants. Compared with vitamin K, NOACs have similar or better efficacy in preventing ischemic stroke with a lower risk of bleeding. In the first report with NOACs and cervical artery dissection (CAD), there were no major bleeds and 5% minor hemorrhagic complications being equal to the rate in the antiplatelet group. 19 The European Society of Cardiology recommends NOACs in preference to Vitamin K antagonist (VKA) therapy for stroke prevention in patients with atrial fibrillation (AF). 23 As the literature on the use of NOACs for treatment and prevention of CAD in patients is sparse, the safety and efficacy of NOAC in primary and secondary prevention in stroke patients with CAD are uncertain, more clinical trials are needed to investigate the short- and long-term use of NOACs in populations of patients with CAD.
However, in most studies, the decision to choose an antithrombotic agent and the duration of treatment for cervical artery dissection remains empirical. This treatment is customized by clinicians for the specific risks and benefits of each patient. Theoretically, antithrombotic agents could diminish the risk of thrombus formation and embolization, which is the proposed mechanism of cerebral ischemia,24-26 despite the fact that stroke might additionally occur as a result of hemodynamic insufficiency. 27 Anticoagulation may be preferred when there is a severely stenotic or occluded vessel, 19 or when a luminal thrombus or micro embolism is detected. 28 Conversely, antiplatelet agents may be favored when there is a large cerebral infarction, intracranial extension of the dissection, spinal cord trauma, or a medical contraindication to anticoagulants such as systemic hemorrhage or recent surgery.19,27,29 For these cases, AP agents may be favored due to concern over intramural hematoma expansion. 19
The main limitation of this study was the lack of randomized controlled trials, which caused our sample size to be too small. With most of the included data coming from case series and retrospective analyses, the quality of our evidence may be classified as very low. Furthermore, in the included studies, treatment decisions were made by clinicians and lacked random selection, which may also affect the results, and subsequently, this meta-analysis. Another limitation of this study was that the duration of follow-up from those included studies was relatively short. Long-term follow-ups for complications of these therapies are necessary for further evaluations. More randomized controlled trials are needed to confirm our results. According to previous estimates, 30 thousands of patients are needed. Assuming an annual stroke risk of 2%, one would need 600 dissection patients in each group (1200 total) with average follow-up of 4 years 23 to compare the efficacy of anticoagulation to antiplatelet in preventing stroke in patients with CAD.
Conclusion
Overall, there were no significant differences between anticoagulant therapy and antiplatelet therapy when treating carotid and vertebral artery dissections in terms of curative effect, all cause death, and ischemic stroke. Additionally, TIA and hemorrhage occurred more frequently in patients treated with anticoagulants, but the rates were not statistically significant. Finally, more randomized controlled trials are needed to confirm these results.
Footnotes
Authors’ Contributions
Sheng-Lin Ye and Tao Tang conceived of the idea and were major contributors in writing the manuscript; Sheng-Lin Ye and Chuang Wang collected the data; Lu-Lu Wang, Tao Tang, and Sheng-Lin Ye performed the statistical analysis. All authors contributed to the interpretation of the results and critically reviewed the first draft. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code Availability
Stata version 13.0.
Ethics Approval and Consent for Participate
The data for this research were extracted from studies published in public databases, thus not needing informed consent. According to local regulations, this retrospective and noninterventional study did not require the approval of the institutional review board (The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.).
Consent for Publication
Written informed consent for publication was obtained from all participants.