
Abstract
Ischemic stroke represents one of the leading causes of death and disability in both the United States and abroad, particularly for patients with prior ischemic stroke or transient ischemic attack (TIA). A quintessential aspect of secondary stroke prevention is the use of different pharmacological agents, mainly antiplatelets and anticoagulants. Antiplatelets and anticoagulants exhibit their effect by blocking the activation pathways of platelets and the coagulation cascade, respectively. Clinical trials have demonstrated the safety and efficacy of antiplatelets for noncardioembolic stroke prevention, while anticoagulants are more often used for cardioembolic stroke prevention. Commonly used antiplatelets include aspirin, clopidogrel, and aggrenox (aspirin plus extended-release dipyridamole). Furthermore, commonly used anticoagulants include warfarin, dabigatran, rivaroxaban, apixaban, and edoxaban. Each of these drugs has a unique mechanism of action, and they share some common adverse events such as gastrointestinal bleeding and intracranial hemorrhage in more serious cases. Consequently, physicians should carefully assess the benefits and risks of using different antiplatelet or anticoagulant therapies when managing patients with previous ischemic stroke or TIA. This review discuses the published literature on major clinical trials assessing the efficacy of different antiplatelet and anticoagulant drugs under varying circumstances and the subsequent guidelines that have been developed by the American Heart Association/American Stroke Association. Additionally, the role of imaging in stroke prevention is discussed.
Introduction
Ischemic stroke is a prevalent disease that has a broad spectrum of health implications, including a high morbidity and mortality rate. Approximately 610 000 cases of ischemic strokes are attributed to first-time stroke in the United States. 1 Stroke prevention strategies focus on both primary and secondary preventions—particularly for individuals with modifiable risk factors such as smoking, hypertension, obesity, hyperlipidemia, and/or diabetes. Approximately 30% of individuals with first-time stroke will experience another stroke within their lifetime. 2 Pharmacological treatments for prevention play a key role in stroke management. In this review article, different classes of antiplatelets and anticoagulants, including single and dual applications, along with their mechanisms of action, clinical use, and guidelines, will be discussed.
Thrombus Formation and Its Role in Ischemic Stroke
Thrombus formation is a temporary and innate response to vessel injury, when circulating platelets are exposed to the extracellular matrix components of the injured vessel. 3 This exposure causes a cascade of events that eventually leads to platelet activation as well as thrombin generation. 4 By and large, both soluble agonists and cell matrix components interact with specific glycoprotein-rich membrane receptors of circulating platelets and initiate transmembrane signals through membrane-associated guanosine-5′-triphosphate-binding proteins. This leads to the activation of phospholipase C and formation of second messengers, diacyl glycerol and inositol 3′-5′ trisphosphate (IP3). Diglyceride acts on protein kinase C, and IP3 mobilizes cytosolic calcium from internal membrane stores. The rise in intracellular calcium activates phospholipase A2 and facilitates the release of arachidonic acid from the membranes. This fatty acid is transformed by cyclooxygenase (COX) to prostaglandin endoperoxides prostaglandin H2 and prostaglandin G2, which are further converted to the active proaggregatory metabolite, thromboxane A2 (TXA2). Agonist-induced activation of platelets activates GPIIb/IIIa receptor, which can bind the active site (Arg-Gly-Asp, RGD) of fibrinogen and recruit other platelets to form aggregates and support thrombus development and growth. Activated platelets also express tissue factor on their membrane, which is a procoagulant and supports the formation of thrombin on their modified surface membrane. Thrombin acts on circulating fibrinogen and generates fibrin, which initiates clot formation. Thrombus development, thrombus growth, and fibrin deposition are essential features of a clot formation during the arrest of bleeding and during acute vascular events.
When a blood vessel is damaged, the subendothelial cell matrix components, such as fibronectin, laminin, and collagen, which are exposed, interact with specific domains of platelet membrane called integrins, which are glycoprotein-rich membrane receptors. 3 Also, collagen-bound von Willebrand factor (vWF) binds to platelet GPIb-V-IX, which is required for platelet adhesion at high shear rates. At low shear rates, collagen can bind to platelets in the absence of vWF, along with fibrin and fibrinogen. 5,6 The growing thrombus develops and forms the platelet plug. Activated platelets, monocytes, microparticles, and ruptured plaque express tissue factors that when activated bind to factor VIIa and cause the activation of factor IX. 3,7 The activated factor IX will perform a proteolytic cleavage that will eventually generate active thrombin. Thrombin converts fibrinogen to fibrin, and also it cleaves protease-activated receptor 1 on the platelet surface to activate platelets. 3 Activated platelets release a variety of chemical substrates—such as adenosine diphosphate (ADP), serotonin, and TXA2—that function as a positive feedback loop to activate more platelets. 3 The platelet integrin GPIIb/IIIa (αIIbβ3) when activated assists in recruitment of fibrinogen and vWF. 8
Antiplatelets and Anticoagulants for Stroke Prevention
Antiplatelet and anticoagulant therapies play a vital role in stroke treatment and prevention. While both groups of medications prevent the formation of a clot, each works on a different clot etiology and subsequently alters different intrinsic pathways. Different antiplatelet agents inhibit different receptors on platelets. While aspirin inhibits TXA2 formation, clopidogrel and prasugrel inhibit the P2Y12 (ADP) receptor and dipyridamole inhibits phosphodiesterase (see Figure 1A). 9 On the other hand, oral anticoagulants prevent the function of various clotting factors such as factors II, VII, IX, and X (Figure 1B). 10 Antiplatelet agents have strong clinical evidence supporting their use for prevention of noncardioembolic stroke (class I, Level of Evidence A), whereas anticoagulants are strongly recommended for prevention of most types of cardioembolic stroke (class I, Level of Evidence A). 11,12
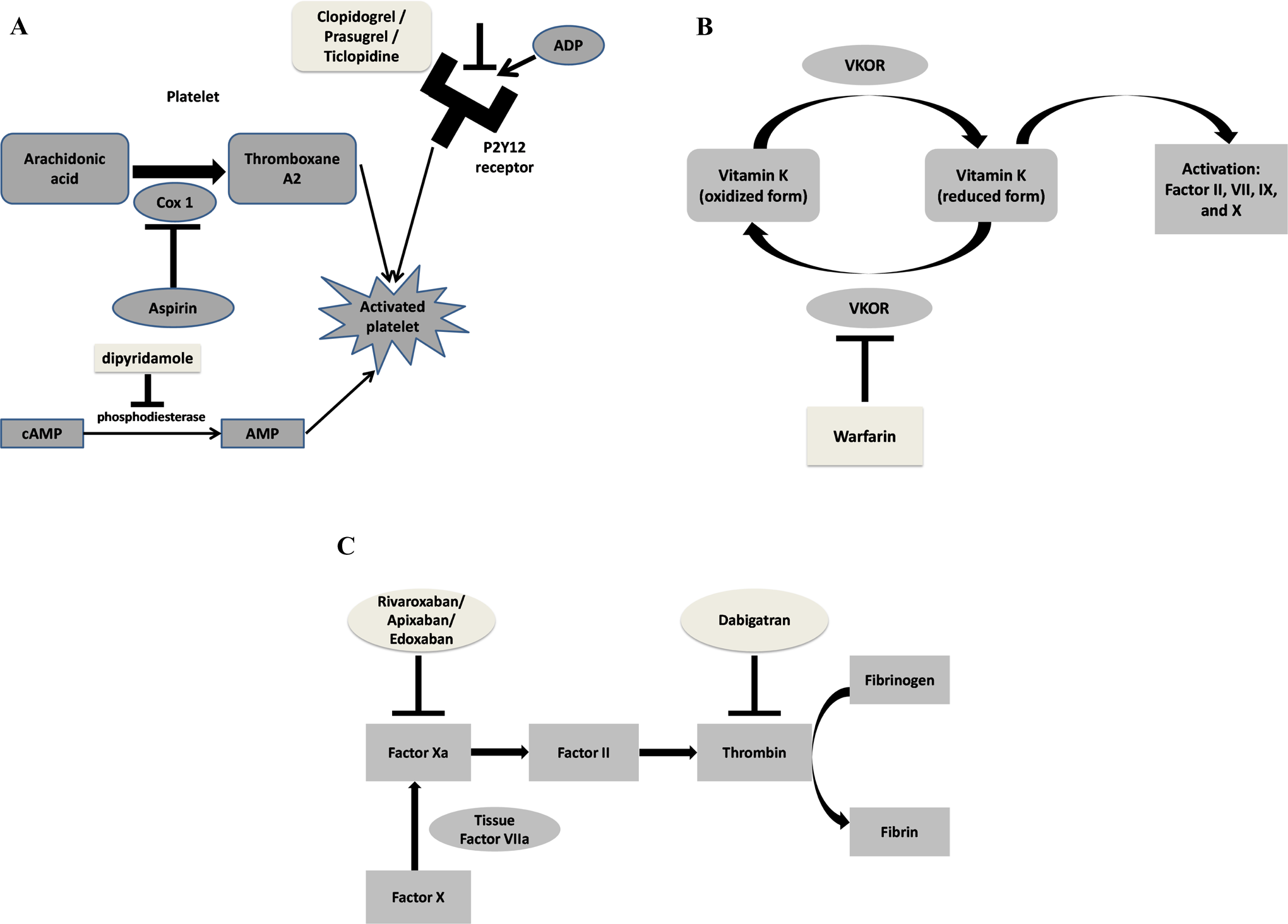
Mechanism of action for various antiplatelet and anticoagulant medications. A, Mechanism for antiplatelet medications that act as ADP receptor antagonists or antiplatelet inhibitors; clopidogrel, prasugrel, and ticlopidine function as ADP receptor antagonists, while aspirin and dipyridamole function as general antiplatelet inhibitors. B, Mechanism of action for the anticoagulant warfarin. C, Mechanism of action of direct factor Xa inhibitors—rivaroxaban, apixaban, and edoxaban—and anticoagulant dabigatran. ADP indicates adenosine diphosphate.
The recent introductions of direct oral anticoagulants (DOACs) have widened the utility of anticoagulant use (note that the International Society of Haemostasis and Thrombosis has agreed upon DOAC as the appropriate term). 13 Unlike warfarin, which targets several vitamin K-dependent clotting factors, DOACs inhibit specific clotting factors. Some of the common DOACs include direct thrombin inhibitors (dabigatran) and factor Xa inhibitors (rivaroxaban, apixaban, and edoxaban; see Figure 1C). 13
Aspirin
Mechanism of action
Aspirin acetylates the active site on the enzyme COX1 and prevents conversion of arachidonic acid to the prostaglandin endoperoxides, the transient intermediates for generation of TXA2 (Figure 1A). Since TXA2 is involved in platelet aggregation and vasoconstriction, aspirin can inhibit primary hemostasis. 14 In vitro studies have demonstrated a nonlinear relationship between TXA2 inhibition and platelet aggregation, since at least 95% inhibition is required to prevent platelet aggregation. 15 Aspirin has a short half-life in vivo ranging between 2 and 3 hours. 16 Within 1 to 2 hours of absorption, aspirin is hydrolyzed into the metabolite salicylic acid. 5,17 The effects of aspirin on existing platelets are irreversible and will last for the life of the platelet, up to 10 days. 18 However, the bone marrow continuously produces new platelets with uninhibited COX1 proteins. 5
The Antithrombotic Trialists’ Collaboration (ATT) 19 was one of the first meta-analyses that tried to identify an optimal dose of aspirin. The study showed that doses ranging from 500 to 1500 mg, as compared to doses ranging from 75 to 325 mg, did not confer a reduced number of vascular events (such as myocardial infarction [MI], stroke, or death). Therefore, it is widely accepted that the optimal dose of aspirin ranges from 81 to 325 mg, though there is still controversy about the dose offers the most prevention while minimizing adverse effects (AEs) such as gastrointestinal (GI) bleeding. 20
Aspirin Resistance
Both clinical and laboratory studies have demonstrated that some patients are less responsive to aspirin therapy, though the so-called “aspirin resistance” is yet to have a standardized definition among the medical community. 21 As such, reports that seek to estimate aspirin resistance prevalence have widely varied. A meta-analysis conducted by Hovens et al 22 estimated a mean prevalence of 25% based on a composite of 42 published studies.
Yi et al 23 studied 634 Chinese patients who had been diagnosed with first stroke (due to large artery atherosclerosis or small vessel occlusion) within 48 hours of symptom onset. 23 Patients were excluded if they had stroke due to other etiologies such as cardioembolism or undetermined etiology. Additionally, patients were excluded if they were using nonsteroidal anti-inflammatory drugs or other aspirin-containing drugs at the time of enrollment. In order to test for aspirin resistance, the researchers administered 200 mg of aspirin/d for the first 2 weeks followed by 100 mg/d. Blood samples were collected and tested for optical platelet aggregation at 7 and 10 days using adenosine 5′-diphosphate and arachidonic acid. Follow-up time was between 12 and 24 months with a median of 19.4 months. About 24.8% of patients had some degree of aspirin resistance, compared with aspirin sensitive patients, leading to a higher incidence of recurrent ischemic stroke (23.3% vs 10%; P < .001), MI (5.3% vs 0.7%; P < .001), and death (8% vs 1.3%; P < .001). The study suggested a strong independent association between aspirin resistance and the occurrence of diabetes and high levels of low-density lipoprotein (LDL). In explaining these results, the authors suggested that hyperlipidemia, found in patients with diabetes and high LDL levels, causes upregulation of isoprostanes such as 8-epi-PGF2a. These isoprostanes can activate arachidonic acid without using COX enzymes and subsequently lead to ineffectiveness of aspirin. The finding was corroborated when the urine samples of these same patients revealed high levels of 11-dehydrothromboxane B2, a breakdown product of TXA2 released by platelets. 24
Other factors may also contribute to aspirin resistance. For instance, in a small trial 25 conducted on healthy volunteers (n = 71), enteric-coated aspirin tablets were shown to have a significantly higher prevalence of incomplete inhibition of thromboxane (defined as <99% thromboxane inhibition) compared with noncoated aspirin (54.3% vs 8%; P = .0004). Enteric-coating causes aspirin to be absorbed in the small intestine, rather than the stomach. In doing so, aspirin is more likely to be inactivated, since the neutral pH of the small intestine causes aspirin to be deacetylated into salicylic acid. Concomitant use of aspirin and proton pump inhibitors (PPIs) has also shown to decrease antiplatelet activity. In a study 26 that compared antiplatelet activity in patients with coronary artery disease (CAD), patients concomitantly using PPIs and aspirin showed higher platelet aggregation (median 180 aggregation units*minute vs 152; P = .003) and serum thromboxane B2 levels (1.29 ng/mL vs 0.92; P = .01) compared with those who used aspirin only.
Patient noncompliance to aspirin therapy is a widespread issue, particularly among elderly patients. 21 With this in mind, it is hard to disentangle true “aspirin resistance” with noncompliance, which can overestimate the rate of aspirin resistance. 21
Complications
The main AEs related to aspirin use include increased risk of GI bleeding and dyspepsia (see Table 1). Other AEs include headache, vertigo, tinnitus, nausea, and bruising. 27 Combining aspirin with other anticoagulants, such as warfarin, has been shown to increase intracerebral hemorrhage (ICH), a serious AE (SAE). 28
Dosing, Half-Life, Usage, and Complications of Different Antiplatelet Agents.
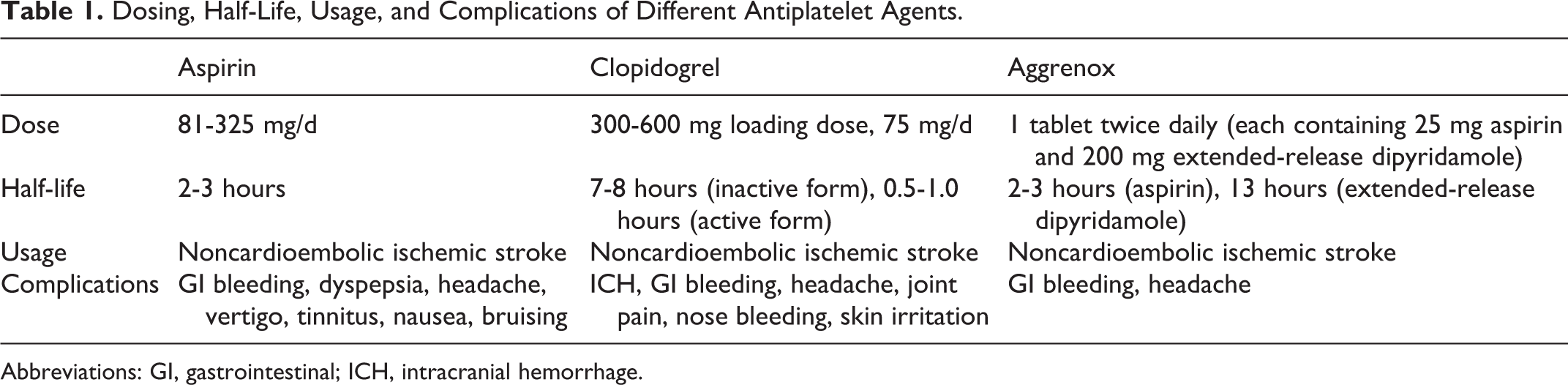
Abbreviations: GI, gastrointestinal; ICH, intracranial hemorrhage.
Aspirin is contraindicated in patients with allergies to nonsteroidal antiinflammatory drugs, asthma, rhinitis, and nasal polyps due to possible bronchospasm, angioedema, or uitcaria. 17 Aspirin is also contraindicated in children and young adults who have a viral infection, due to the possibility of developing Reye syndrome. 17 Although there is a lack of consensus regarding aspirin use during pregnancy, many clinicians acknowledge the potential harm that aspirin use can have due to its ability to cross the placenta. 12 Aspirin use has been associated with congenital defects such as gastroschisis, anophthalmia, and microphthalmia—particularly during the first trimester. As a result, the American Heart Association/American Stroke Association (AHA/ASA) only recommends low-dose aspirin use during the second and third trimester (class IIa, Level of Evidence B). 12 Furthermore, postpartum women should exert caution when taking aspirin, as high doses have been shown to cause breast milk to contain salicylate, which has been linked to fetal metabolic acidosis and GI bleeding. 12
Clinical Use Guidelines
Aspirin has been used as the gold standard in noncardioembolic ischemic stroke prophylaxis for much of the past century—not only due to its clinical effectiveness but also because of its cost-effectiveness. 5,21,29
The Stroke Prevention in Atrial Fibrillation (SPAF-1) study 30 was one of the first clinical trials to demonstrate the efficacy of aspirin for primary prevention of stroke in patients with atrial fibrillation (AF; see Table 2). In the study, 703 patients were randomized to receive either 325 mg aspirin/d or placebo. The primary outcome of the study was occurrence of ischemic stroke or systemic embolism, and the secondary outcome was death, MI, or transient ischemic attack (TIA). Analysis of the data revealed a lower incidence of the primary outcome compared with the placebo (3.6%/year vs 6.3%/year; P = .02). Furthermore, a similar trend was observed for the combination of primary outcome and death (7.9%/year for aspirin group vs 11.8%/year for placebo group; P = .02).
Summary of Major Clinical Trials Involving Cardioembolic Stroke Using Antiplatelet or Anticoagulant Medication.
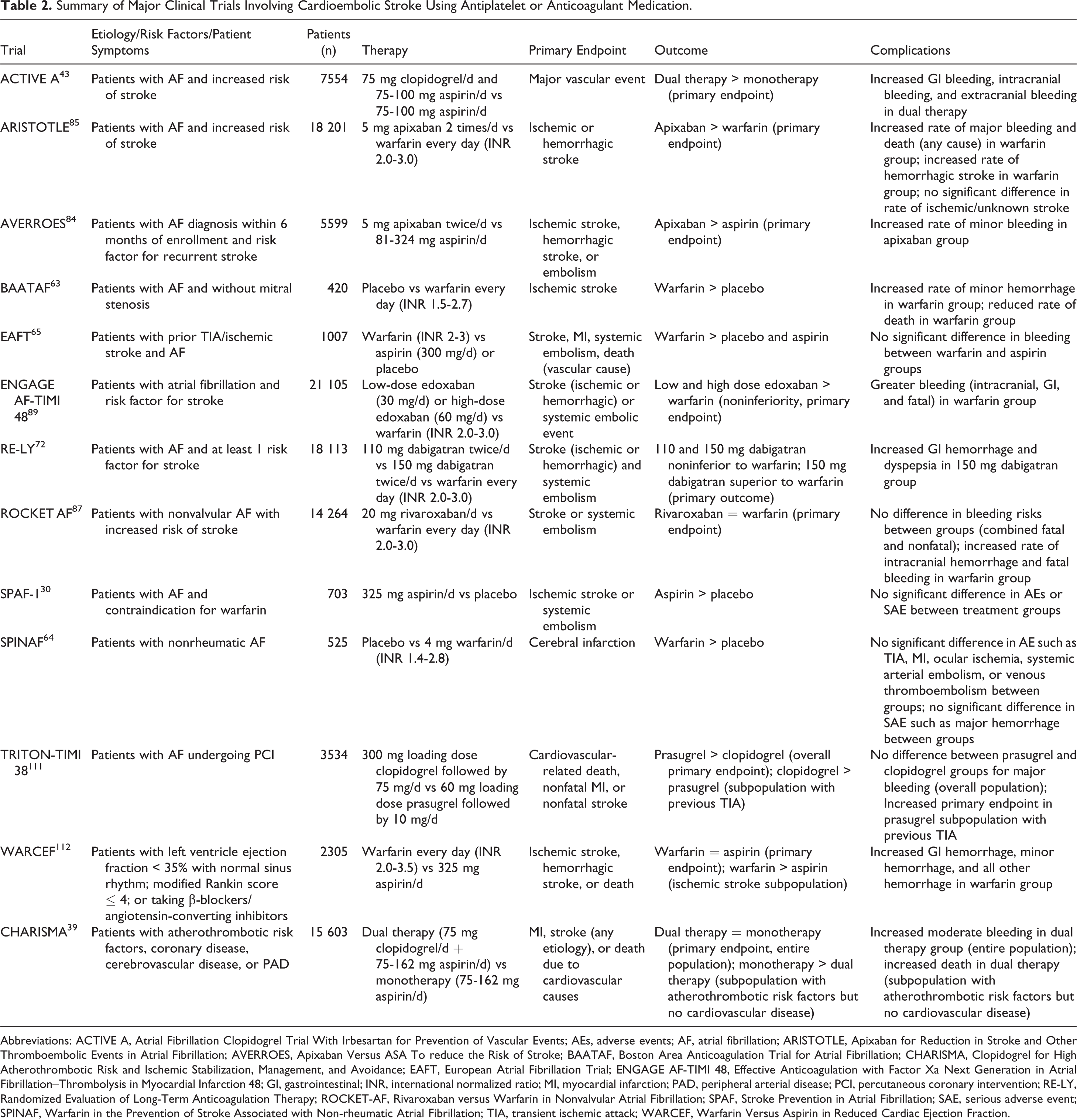
Abbreviations: ACTIVE A, Atrial Fibrillation Clopidogrel Trial With Irbesartan for Prevention of Vascular Events; AEs, adverse events; AF, atrial fibrillation; ARISTOTLE, Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation; AVERROES, Apixaban Versus ASA To reduce the Risk of Stroke; BAATAF, Boston Area Anticoagulation Trial for Atrial Fibrillation; CHARISMA, Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance; EAFT, European Atrial Fibrillation Trial; ENGAGE AF-TIMI 48, Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48; GI, gastrointestinal; INR, international normalized ratio; MI, myocardial infarction; PAD, peripheral arterial disease; PCI, percutaneous coronary intervention; RE-LY, Randomized Evaluation of Long-Term Anticoagulation Therapy; ROCKET-AF, Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation; SPAF, Stroke Prevention in Atrial Fibrillation; SAE, serious adverse event; SPINAF, Warfarin in the Prevention of Stroke Associated with Non-rheumatic Atrial Fibrillation; TIA, transient ischemic attack; WARCEF, Warfarin Versus Aspirin in Reduced Cardiac Ejection Fraction.
Consensus clinical guidelines for aspirin use have also been made for patients with intracranial atherosclerosis. These guidelines were based on studies such as the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) trial (see Table 3). 31 The WASID trial randomized patients into the following groups: a warfarin group who received an initial dose of 5.0 mg/d or an aspirin group who received 1300 mg/d. Patients in the warfarin group had a significantly higher rate of major hemorrhage (8.3% vs 3.2%; P = .01) and death (9.7% vs 4.3%; P = .02) compared with the aspirin group. The study enrollment was discontinued prematurely due to SAE experienced by the warfarin group.
Summary of Major Clinical Trials Involving Noncardioembolic Stroke Using Antiplatelet or Anticoagulant Medication.
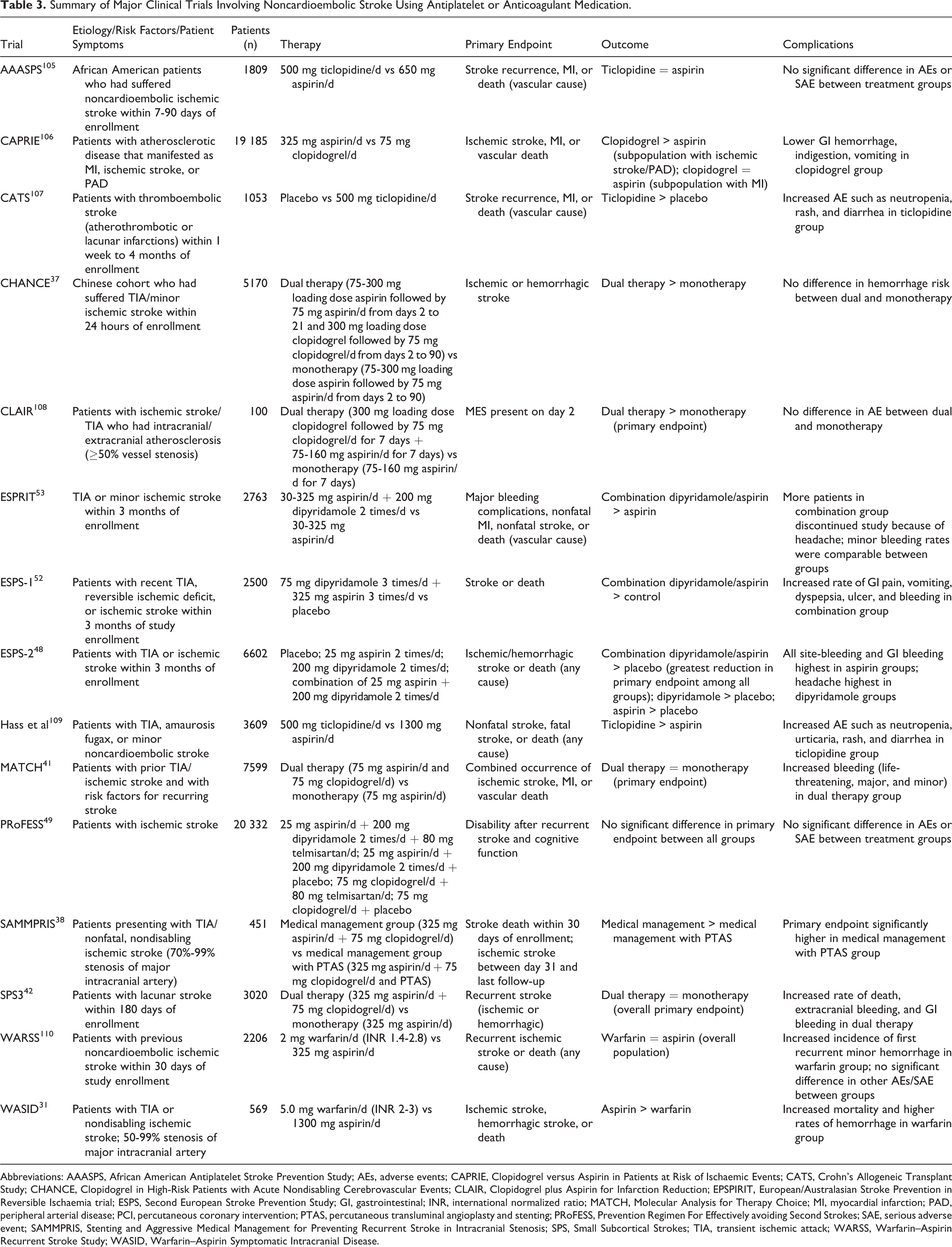
Abbreviations: AAASPS, African American Antiplatelet Stroke Prevention Study; AEs, adverse events; CAPRIE, Clopidogrel versus Aspirin in Patients at Risk of Ischaemic Events; CATS, Crohn’s Allogeneic Transplant Study; CHANCE, Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events; CLAIR, Clopidogrel plus Aspirin for Infarction Reduction; EPSPIRIT, European/Australasian Stroke Prevention in Reversible Ischaemia trial; ESPS, Second European Stroke Prevention Study; GI, gastrointestinal; INR, international normalized ratio; MATCH, Molecular Analysis for Therapy Choice; MI, myocardial infarction; PAD, peripheral arterial disease; PCI, percutaneous coronary intervention; PTAS, percutaneous transluminal angioplasty and stenting; PRoFESS, Prevention Regimen For Effectively avoiding Second Strokes; SAE, serious adverse event; SAMMPRIS, Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis; SPS, Small Subcortical Strokes; TIA, transient ischemic attack; WARSS, Warfarin–Aspirin Recurrent Stroke Study; WASID, Warfarin–Aspirin Symptomatic Intracranial Disease.
Based on the results of several randomized clinical studies, the AHA/ASA has recommended aspirin doses between 50 and 325 mg/d for prevention of reoccurring TIA or ischemic stroke (class I, Level of Evidence A) and the daily use of 325 mg aspirin for patients with stroke with major intracranial stenosis defined as 50% to 99% blockage (class I, Level of Evidence B). 12 The AHA/ASA does not suggest that an increased dosage of aspirin above 325 mg/d provides an increased benefit (class IIb, Level of Evidence C). Moreover, the use of aspirin therapy for stroke prevention in patients with AF who cannot tolerate anticoagulation therapy is recommended (class I, Level of Evidence A). 12
Clopidogrel
Mechanism of action
Clopidogrel has a different mechanism of action than aspirin, since it is a prodrug that is inactive until it is hydrolyzed by cytochrome P450 in the liver via an nicotinamide adenine dinucleotide phosphate (NADPH)-dependent mechanism. 18 Once activated, clopidogrel will bind irreversibly to the ADP receptor, P2Y12, which is located on the membrane of platelets (Figure 1A). 9 This precludes ADP from binding to platelets, thereby inhibiting platelet activation and subsequent thrombus formation. The recommended dose of clopidogrel is 75 mg/d, although a loading dose of 300 or 600 mg is often given to expedite the antiplatelet effects when the patient is scheduled for an endovascular recanalization procedure within a day of the therapy initiation. 32 Unlike the fast-acting effects of aspirin (60 minutes), clopidogrel (75 mg) elicits a much slower onset in which peak platelet inhibition is observed within 3 to 7 days. 29,33 Patients on PPIs are advised against taking clopidogrel, as these drugs have been shown to inactivate the enzyme cytochrome P450 2C19, which is involved in converting clopidogrel from its inactive to active form. 34 Additionally, there is some evidence to indicate that combination use of clopidogrel and certain statins may interfere with antiplatelet function, since both clopidogrel and statins use cytochrome P450 3A4. 35
Complications
Systemic bleeding such as GI is one of the common AEs associated with clopidogrel use (see Table 3). Other AEs include headache, joint pain, nosebleed, and skin irritation. 10 ICH, though presents a risk, is less associated with clopidogrel monotherapy. Patients with liver disease, who are breast-feeding or who have pathological bleeding, are considered to have a contraindication for clopidogrel. 36
Clinical Use Guidelines
Clopidogrel is commonly prescribed for prophylaxis of noncardioembolic stroke for patients who do not tolerate aspirin therapy (class IIa, Level of Evidence C). 11,29
In 2014, the AHA/ASA released 2 new updates regarding clopidogrel use guidelines. 12 The first update states the potential usefulness of combining aspirin and clopidogrel within 24 hours of TIA/minor ischemic stroke and keeping patients on this dual antiplatelet therapy for 90 days (class IIb, Level of Evidence B). This recommendation was influenced in part by the Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack (CHANCE) trial (see Table 1). 37 The second update states that patients with stroke due to severe stenosis (70%-99%) may benefit from 90 days combination of clopidogrel and aspirin therapy (class IIb, Level of Evidence B). This recommendation was influenced in part by the Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis (SAMMPRIS) trial, 38 the details of which are mentioned later (Table 1).
The Role of Dual Antiplatelet Therapy (Aspirin and Clopidogrel) for Stroke Prevention
The Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) 39 was a major trial that looked at dual antiplatelet therapy compared with aspirin monotherapy (see Table 2). A total of 15 603 patients were enrolled in CHARISMA, all of whom had atherothrombotic risk factors, coronary disease, cerebrovascular disease, or peripheral arterial disease (PAD). The primary study end point was defined as occurrence of MI, stroke (any etiology), or death due to cardiovascular causes. The study showed no statistical difference in the occurrence of primary outcome between treatment groups (dual therapy 6.8% vs monotherapy 7.3%; P = .22). On the other hand, patients in the dual therapy group had increased rates of moderate bleeding—defined as any bleeding requiring blood transfusion that did not compromise hemodynamic stability, per the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO) 40 scale (2.1% vs 1.3%; P < .001). Furthermore, a subgroup analysis of the patient population showed that individuals with atherothrombotic risk factors—but without cardiovascular disease—assigned to dual therapy had a greater risk of death (5.4% vs 3.8%; P = .04). These results suggested that dual therapy provides no added benefit compared to monotherapy but increases the risk of AE or SAE.
The Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attacks or Ischemic Stroke (MATCH) 42 trial also found no added benefit of dual antiplatelet therapy in stroke prevention (see Table 1). In the study, 7599 patients were randomized to receive either dual therapy (75 mg aspirin plus 75 mg clopidogrel/d) or monotherapy (75 mg clopidogrel/d). The primary outcome for MATCH was combined occurrence of ischemic stroke, MI, and vascular death after 18 months. Patients were included on the basis of prior stroke or TIA within 3 months of enrollment. Additionally, all patients were required to have one of the following stroke risk factors: previous MI, diabetes mellitus, PAD, or angina pectoris. The trial demonstrated no significant difference in the primary outcome between dual therapy and monotherapy (16% vs 17%; P = .244). However, patients in the dual therapy group had significantly higher rates of life-threatening bleeding (defined as fatal bleeding, ICH, or bleeding requiring transfusion of ≥4 units of blood; 3% vs 1%; P < .0001).
The Secondary Prevention of Small Subcortical Strokes (SPS3) 42 trial also found no benefit of dual antiplatelet therapy in stroke prevention (see Table 1). The SPS3 investigators randomized 3020 patients who had had a lacunar stroke within 180 days of enrollment into a dual therapy (n = 1517, 325 mg aspirin/d and 75 mg clopidogrel/d until study discontinuation) and monotherapy (n = 1503, 325 mg aspirin/d until study discontinuation) group. None of the patients included in this trial had ipsilateral carotid artery disease, cardioembolic stroke, previous ICH, or cortical ischemic stroke. The primary outcome for SPS3 was recurrence of either hemorrhagic or ischemic stroke, and the secondary outcome was acute MI or death. There was no statistically significant difference in primary outcome between dual antiplatelet therapy and monotherapy (2.7%/year vs 2.5%/year; P = .48). However, the rate of death was higher in dual therapy compared to monotherapy (2.1%/year vs 1.4%/year; P < .004). Adding to this, patients in the dual therapy group had a higher incidence of extracranial bleeding requiring red blood cell transfusion, surgery, or leading to death (1.7%/year vs 0.79%/year; P < .001) and GI bleeding (1.1%/year vs 0.52%/year; P < .001). Based on the CHARISMA and SPS3 trials, the AHA/ASA provided the recommendation that long-term dual antiplatelet therapy is not suitable for secondary prevention of recurrent stroke in patients with TIA or ischemic stroke (class III, Level of Evidence A). 12
The investigators in the CHANCE 37 trial examined if dual antiplatelet therapy given over a shorter time period (90 days) would be more effective than aspirin monotherapy in preventing recurrent stroke in a Chinese cohort population who had TIA or minor ischemic stroke (see Table 1). Patients, 40 years or older, who had had a TIA within 24 hours, were randomized to either the aspirin (75-300 mg/d loading dose, 75 mg/d days 2-90) monotherapy group or the dual antiplatelet (75 mg aspirin/d, 300 mg clopidogrel loading dose, 75 mg clopidogrel/d days 2-90) group. Patients were excluded if they presented with strokes with etiology other than TIA, vascular malformation, National Institute of Health Stroke Scale (NIHSS) score >4, a clear indication for anticoagulant therapy, or contraindication to clopidogrel or aspirin. The dual antiplatelet group had a 32% reduction in recurrent stroke compared with the aspirin-only group. The results of this study were important because they demonstrated that administration of dual antiplatelet therapy for patients with TIA did not increase hemorrhage risk. These findings were novel, as previous studies such as CHARISMA 39 and SPS3 42 had focused on combination of aspirin/clopidogrel therapy treatment on patients who had more severe strokes than TIA and were consequently at a greater risk of hemorrhage. In addition, because the divergence in stroke incidence was greatest within the first few days of the experiment, this could suggest that clopidogrel treatment is most effective to prevent early recurrent ischemia. Based on the results of studies like the CHANCE trial, the AHA/ASA provided a new recommendation in 2014 that dual antiplatelet therapy initiated within 24 hours of an ischemic stroke or TIA might be beneficial to continue for up to 90 days (class IIb, Level of Evidence B). 12
The SAMMPRIS 38 study has shown that combination antiplatelet therapy, which consists of aspirin and clopidogrel, may be more effective than percutaneous transluminal angioplasty and stenting (PTAS) for the treatment of intracranial arterial stenosis (see Table 1). Patients in the study were randomized to one of the following groups: the medical management group, which consisted of 325 mg of aspirin/d until study discontinuation and 75 mg of clopidogrel/d for 90 days, and the PTAS plus medical management group. The primary end point of the study was stroke/death within 30 days of enrollment or ischemic stroke between day 31 and up to 3 years post-enrollment. The medical management group had a 12.2% and the PTAS plus medical management had a 20% probability of primary end point 1 year post-enrollment (P = .009). The SAMMPRIS study enrollment was discontinued after 451 patients due to significantly higher primary end point within 30 days in the PTAS plus medical management group compared with the medical management group (14.7% vs 5.8%; P = .002). Consequently, the AHA/ASA does not recommend the use of PTAS as initial treatment for patients with ischemic stroke/TIA caused by severe stenosis of a major intracranial artery (class III, Level of Evidence B). 12 However, the potential benefit of dual antiplatelet therapy in patients with severe intracranial atherosclerosis (class IIb, Level of Evidence B) has been suggested.
The Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events (ACTIVE A) 43 provided crucial insight toward the efficacy of dual antiplatelet therapy in preventing ischemic events in patients with AF (see Table 2). The primary outcome for ACTIVE A was a major vascular event—defined as stroke, noncentral nervous system embolism, MI, or death due to a vascular event. Analysis of the study data revealed that patients subject to dual antiplatelet treatment had a reduced incidence of the primary outcome compared with aspirin treatment (6.8%/year vs 7.6%/year; P = .01). Furthermore, the dual antiplatelet group had a greater reduction in stroke compared with the aspirin group (2.4%/year vs 3.3%/year; P < .001). When strokes were categorized based on severity, the dual antiplatelet group also outperformed the aspirin group (0.9%/year vs 1.2%/year for nondisabling and 1.6%/year vs 2.1%/year for disabling/fatal; P = .004 and .001, respectively). However, due to increased risk of AE, the AHA/ASA recommends that clinicians may consider dual antiplatelet therapy for patients with AF (class IIb, Level of Evidence B). 12
Aggrenox
Mechanism of action
Aggrenox is unique in the sense that it combines the use of 2 different antiplatelet drugs (aspirin and dipyridamole; see Figure 1A). Aggrenox tablets contain 25 mg of aspirin and 200 mg of extended-release dipyridamole and are usually taken twice per day. Dipyridamole is believed to have 3 different effects that contribute to antiplatelet activity. 44 First, dipyridamole blocks the activity of platelet cyclic adenosine monophosphate (cAMP)-phosphodiesterases (PDEs), preventing activation of PDEs increases intracellular cAMP levels and thereby preventing the initiation of key cellular pathways involved in platelet aggregation, such as calcium release and G-protein linked activation. 45 Second, it prevents the breakdown of adenosine. In vivo, adenosine binds to various G-protein-linked receptors and causes increased cAMP levels. 46 Third, dipyridamole amplifies the synthesis/effectiveness of prostanoids such as prostacyclins. Prostacyclins are used in producing cAMP and thus function to inhibit platelet activation. 44
Complications
The 2 major AEs associated with aggrenox are GI bleeding and headache (see Table 3). 47 Nonetheless, aggrenox has a relatively comparable level of safety to aspirin monotherapy. For example, AEs such as GI bleeding were seen at similar levels in the European Stroke Prevention Study (ESPS)-2 trial 48 between the aggrenox and aspirin groups (8.7% and 8.2%, respectively; P< .001). In the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial, 49 patients subjected to aggrenox therapy had slightly higher GI bleeding compared with patients subjected to clopidogrel therapy (4.1% vs 3.6%, 95% confidence interval [CI]: 1.00-1.32). Adding to this, patients in the aggrenox group also had higher rates of SAE such as intracranial bleeding (1.4% vs 1.0%, 95% CI: 1.11-1.83). In some circumstances, the headaches experienced by patients taking aggrenox can be quite severe, as 10% of patients in the ESPS-2 trial chose to discontinue treatment due to headache. Further investigation on aggrenox-induced headaches demonstrated an inverse relation between time since treatment started and headache severity. 50 Similar to aspirin, contraindications for aggrenox are included for patients with allergies to nonsteroidal antiinflammatory drugs as well as children or young adults with viral infections. 51
Clinical Use Guidelines
There have been 4 major clinical trials that have looked at the effectiveness of aggrenox. 12 These trials include ESPS-1 and ESPS-2 48,52 , the European/Australasian Stroke Prevention in Reversible Ischaemia Trial (ESPRIT) 53 , and the PRoFESS 54 trial. Overall, the results from the ESPS-1, ESPRIT, and PRoFESS trials have demonstrated the efficacy of aggrenox in secondary stroke prevention against placebo, aspirin, and clopidogrel, respectively (Table 1). 12
In 2014, the AHA/ASA updated their guidelines to include the use of 25 mg aspirin/200 mg extended-release dipyridamole for prevention of noncardioembolic ischemic stroke or TIA (class I, Level of Evidence B). 12 Future clinical trials will be needed to determine the optimal pharmacological therapy for treatment of stroke/TIA with 50% to 99% stenosis of a major intracranial artery, as there is not enough information to provide clear recommendations regarding aggrenox, clopidogrel, or other drugs such as the phosphodiesterase inhibitor cilostazol (class IIb, Level of Evidence C). 12
Warfarin
Mechanism of action
Warfarin is an anticoagulant that functions by inactivating the VKORC1 subunit of vitamin K epoxide reductase (Figure 1B). This prevents γ-carboxylation of vitamin K-dependent coagulation proteins (II, VII, IX, X, C, S, and Z), leading to decreased levels of active protein. 55 The overall effect of warfarin is to decrease coagulation, even though the natural anticoagulant proteins C, S, and Z are also reduced. 92 From a clinical standpoint, administration of warfarin decreases the risk of embolism and thrombosis. Warfarin has a slow onset of action, usually 2 to 3 days. In addition, warfarin takes longer to be metabolized, as the effects of warfarin are still detectable between 2 and 5 days after cessation of the medication. The metabolism of warfarin is in part dependent on a patient’s haplotypes of the vitamin K epoxide reductase complex subunit 1 (VKORC1) and cytochrome P450 2C19 (CYP2C9); VKORC1 polymorphisms account for about 30% of the variation in warfarin efficacy. Individuals with the type A haplotype have an increased effect of warfarin because they produce less VKORC1, and individuals with the type B haplotype have a decreased effect of warfarin because they produce more VKORC1. The CYP2C9 polymorphisms account for 10% of variation, mainly affecting people of European ancestry. 56
Complications
The main AE for warfarin is GI bleeding, with the risk of ICH of greatest concern (see Table 4). Occasionally, patients experience diarrhea, vomiting, and there is concern of osteoporosis in long-term use. Because of the significant interpatient metabolism variation, the warfarin dose must be monitored and adjusted for therapeutic range of the international normalized ratio (INR), with the goal INR usually between 2 and 3. 57 Contraindications for warfarin use include bleeding diathesis, thrombocytopenia, uncontrolled hypertension, recent GI bleeding, and liver disease. 58
Dosing, Half-Life, Usage, and Complications of Different Anticoagulant Agents.
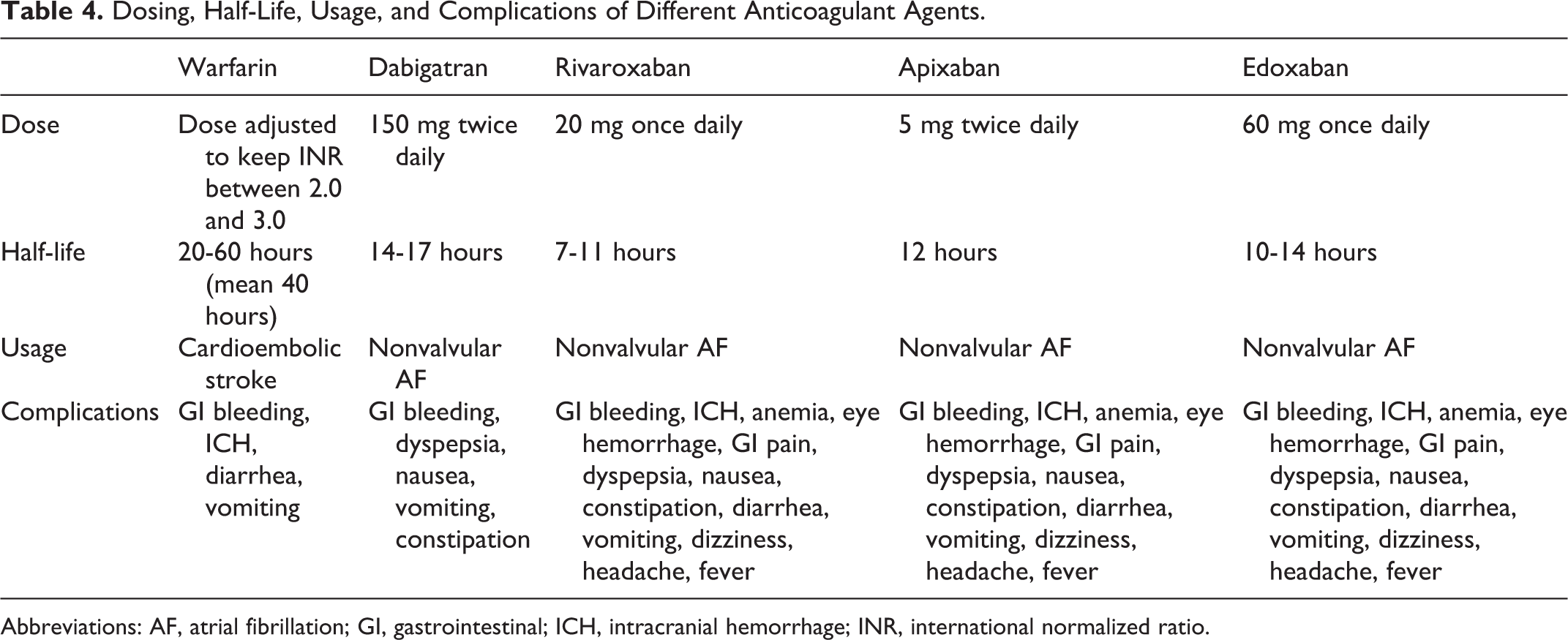
Abbreviations: AF, atrial fibrillation; GI, gastrointestinal; ICH, intracranial hemorrhage; INR, international normalized ratio.
Patients who take warfarin are advised to monitor their daily vitamin K intake by being consistent in their use of foods rich in vitamin K. In addition, patients who consume large amounts of ginger and garlic have also reported increased bleeding risks. 59,60 Warfarin use in pregnant women is generally avoided, due to teratogenic effects. There is inconclusive evidence about whether warfarin use increases the risk of osteoporosis, as some studies suggest that there is a relationship, while others do not. 57 Thyroid function can also affect the efficacy of warfarin. Patients with hypothyroidism have a reduced effect of warfarin, while patients with hyperthyroidism have an increased effect of warfarin. This is believed to occur because thyroxine increases the affinity of warfarin to its receptor site in the liver. 61,62
Clinical Use Guidelines
Warfarin therapy is commonly used for prevention of cardioembolic stroke. 11 The results of the trials such as Boston Area Anticoagulation Trial for Atrial Fibrillation (BAATAF), 63 Warfarin in the Prevention of Stoke Associated with Non-rheumatic Atrial Fibrillation (SPINAF), 64 and the European Atrial Fibrillation Trial (EAFT) 65 influenced the AHA/ASA recommendation that patients with ischemic stroke/TIA and AF (either paroxysmal or permanent) be subject to warfarin therapy by maintaining the INR levels between 2 and 3 (class I, Level of Evidence A; see Table 2). 11
A new guideline that was introduced in 2014 by the AHA/ASA was that postpartum women who are at risk of stroke and are breast-feeding may benefit from warfarin use even after pregnancy (class IIa, Level of Evidence C). 12 This recommendation may have been based in part on a clinical study 66 of 13 females who were breast-feeding and taking warfarin (either during pregnancy or postpartum). Analysis of the breast milk found insignificant amounts of warfarin (<0.08 μmol/L); in addition, none of the babies had any detectable amounts of serum warfarin.
Dabigatran
Mechanism of action
Dabigatran functions by competitively binding to the active site of thrombin (Figure 1C). In doing so, dabigatran prevents thrombin from converting fibrinogen to its active form, fibrin, and thereby inhibits thrombus development. 67 Dabigatran is a hydrophilic molecule that has a constant charge at physiological pH; this feature causes very poor bioabsorption of dabigatran. 68 In order to reverse this, hydrophobic groups such as ethyl and hexyloxycarbonyl are added to dabigatran, facilitating GI absorption. Furthermore, dabigatran tablets are often coated with tartaric acid, which further assist in gastric absorption. 68 Similar to clopidogrel, dabigatran tablets are ingested as a prodrug. Dabigatran becomes activated upon esterase-catalyzed hydrolysis. 69 Unlike clopidogrel, however, dabigatran does not use CYP enzymes to convert to its active form. This reduces the likelihood of drug–drug interactions, since many drugs use CYP enzymes. 68 Because it binds to the active site of thrombin, dabigatran is able to inhibit both fibrin-bound and unbound thrombin. 67 This is because exosite 1 of thrombin—which serves as a docking site for fibrin—is unable to interact with the active site. In this regard, dabigatran is superior to unfractionated heparins and low-molecular-weight heparins since these heparins are unable to inhibit fibrin-bound thrombin. 67 Unlike warfarin, for which onset can take 4 days, dabigatran has a much faster acting effect, as onset is seen within 36 to 72 hours. Furthermore, dabigatran does not require regular INR monitoring or diet modifications. 67 Dabigatran has a half-life ranging from 14 to 17 hours. 70
Complications
The most common AE in dabigatran use is dyspepsia and GI bleeding (see Table 4). Less reported AEs include nausea, vomiting, and constipation. 71
Clinical Use Guidelines
One of the major phase III clinical trials that tested the efficacy of dabigatran was the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) 73 study group (see Table 2). In the study, 2 doses of dabigatran (110 mg and 150 mg twice/d) were compared to warfarin (INR between 2.0 and 3.0) for occurrence of stroke and systemic embolism in patients with AF. The study showed that dabigatran was not inferior to warfarin (P < .001), while resulting in a lower rate of hemorrhagic stroke compared with the warfarin group. Based on the overall clinical benefit seen from dabigatran therapy, the AHA/ASA has included the use of dabigatran for prevention of recurrent stroke in patients with paroxysmal/permanent nonvalvular AF (class I, Level of Evidence B). 12
It is worth mentioning that although both dabigatran doses used for RE-LY trial showed noninferiority to warfarin, the US Food and Drug Administration (FDA) only approved the use of 150 mg tablets. 73 This decision was due in part to a subanalysis of RE-LY that compared the efficacy of both doses of dabigatran in patients aged ≥75 or impaired kidney function. These patients were chosen since they had an increased risk of bleeding or higher than normal dabigatran serum concentration and thus might benefit from a lower dabigatran dose. Within patients over 75, the higher dose of dabigatran conferred lower stroke and systemic embolism rates (1.4 per 100 patient-years) compared with the lower dose (1.9 per 100 patient-years). Although the higher-dose group also had increased rates of major bleeding (5.1 per 100 patient-year vs 4.4), the benefit of higher stroke prevention was considered to exceed the risk of bleeding. Patients with severe renal impairment were excluded from RE-LY, but the investigators were still able to analyze a group with moderate renal impairment (defined as creatinine clearance between 30 and 50 mL/min). In this group, the higher dose of dabigatran also conferred a reduced occurrence of stroke (1.3 per 100 patient-years vs 2.4). Furthermore, the higher dose did not confer an increased risk of bleeding. The FDA has also approved 75 mg tablets for patients with severe renal impairment based on pharmacokinetic data.
Factor Xa Inhibitors (Rivaroxaban, Apixaban, and Edoxaban)
Mechanism of action
Rivaroxaban is a factor Xa inhibitor. 74 Rivaroxaban binds reversibly to the S1 and S4 pockets of factor Xa (the common factor between intrinsic and extrinsic coagulation pathways; Figure 1C). In order to do this, structural molecules in rivaroxaban, such as the (S)-oxazolidinone ring, facilitate binding to factor Xa. Furthermore, tyrosine-228—located in the interior of the S1 binding site—binds to a chlorine molecule on rivaroxaban, creating the S1-chlorothiophene moiety. This moiety has 2 functions. First, it removes a water molecule from the active site, which assists in ligand binding. 75 Second, the interaction precludes any strongly basic groups from binding to factor Xa. The latter function is important because rivaroxaban is a nonbasic protein and otherwise would not be able to bind to factor Xa. Because of its nonbasic and lipophilic nature, rivaroxaban can readily pass through the GI tract epithelia. 74 Consequently, when orally ingested, rivaroxaban exhibits its maximum concentration within 2 to 4 hours and has a half-life between 7 and 11 hours. 76
Apixaban and edoxaban share mechanisms similar to rivaroxaban, as they both inhibit factor Xa (Figure 1C). 77 Furthermore, both drugs bind to the S1 and S4 pockets of factor Xa and also have been shown to exhibit a dose-dependent inhibition of factor Xa. 78 Apixaban—similar to rivaroxaban—exhibits maximum concentration within 3 to 4 hours of oral ingestion and has a half-life of 12 hours. 77 Edoxaban has a half-life ranging from 10 to 14 hours and exhibits maximum concentration within 1 to 2 hours. 79,80
A major benefit of using direct factor Xa inhibitors is that they can inactivate prothrombinase activity in addition to clot-bound or free factor Xa. Furthermore, patients taking factor Xa inhibitors do not need constant monitoring/dose adjustments to ensure therapeutic INR levels. 81
Complications
The most common SAE for factor Xa inhibitors is hemorrhage (GI and intracranial; see Table 4). 82 The AE for factor Xa inhibitors include anemia, eye hemorrhage, GI pain, dyspepsia, nausea, constipation, diarrhea, vomiting, dizziness, headache, and fever. 83
Factor Xa inhibitors are contraindicated in patients with clinically significant bleeding, liver disease, renal impairment requiring dialysis, concomitant use of HIV protease inhibitors and other medications that interact with cytochrome P450 or p-glycoprotein, pregnant women, and breast-feeding women. 83
Clinical Use Guidelines
Although there is strong evidence (class I, Level of Evidence A) to indicate that patients with paroxysmal or permanent nonvalvular AF should be started on warfarin therapy in order to prevent stroke, there are some patients who are hesitant to begin warfarin therapy due to the dietary restrictions and routine monitoring that is involved. 12 As such, factor Xa inhibitors have shown to be a viable alternative to warfarin therapy. 12 One study that exhibited the efficacy of factor Xa inhibitors was the Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment trial (see Table 2). 84 In the trial, the patients with a history of stroke/TIA were randomized to receive either 5 mg of apixaban twice daily or 81 to 324 mg of aspirin per day. The primary end points of the study were ischemic stroke, hemorrhagic stroke, or embolism. Patients in the apixaban group had significantly less occurrence of the primary end point (1.6%/year vs 3.7%/year; P < .001).
Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation 85 trial (Table 2) is another study that demonstrated the efficacy of apixaban. In the study, 10 mg apixaban/d was compared to warfarin (INR 2.0-3.0) for occurrence of stroke. A total of 18 201 patients were recruited on the basis of diagnosed AF and at least 1 risk factor for stroke (defined as age ≥ 75, prior stroke/TIA, prior heart failure, or hypertension). Patients were excluded if they had mitral stenosis, a prosthetic heart valve, stroke within 7 days of enrollment, glomerular filtration rate (GFR) < 25 mL/min or creatinine > 2.5 mg/dL, contraindication for study drugs, or clear indication for antiplatelet therapy (aspirin or clopidogrel). Patients were followed for a median duration of 1.8 years. Compared with the warfarin group, patients in the apixaban group had a reduced incidence of the primary outcome (1.27%/year vs 1.60%/year; P = .01). Within the primary outcome, the greatest benefit was seen in hemorrhagic stroke as patients in the apixaban group had a lower incidence compared with the warfarin group (0.24%/year vs 0.47%/year; P < .001). Furthermore, across 2 different bleeding scales—GUSTO and Thrombolysis in Myocardial Infarction (TIMI) 86 —apixaban was shown to have reduced bleeding events (0.52%/year vs 1.13%/year GUSTO severe and 1.29%/year vs 2.18%/year GUSTO moderate or severe; 0.96%/year vs 1.69%/year TIMI major, 1.55%/year vs 2.46%/year TIMI major or minor; P< .001 for all comparisons).
The Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) 87 demonstrated the efficacy of rivaroxaban (Table 2). In the trial, 14 264 patients were randomized to either the rivaroxaban (20 mg/d) or warfarin group (INR 2.0-3.0). Patients were recruited on the basis of nonvalvular AF and increased risk of stroke (prior stroke/TIA, systemic embolism, hypertension, age ≥75, or diabetes mellitus). Patients with GFR <30 mL/min and liver disease were excluded. Patients were kept on study drugs for a median time of 590 days and followed for a median time of 707 days. The primary outcome for ROCKET AF was stroke (ischemic/hemorrhagic) or systemic embolism. For occurrence of the primary outcome, rivaroxaban was shown to be noninferior to warfarin (1.7%/year rivaroxaban vs 2.2%/year warfarin; P < .001). Furthermore, the rivaroxaban group had reduced SAE such as fatal bleeding (0.2%/year vs 0.5%/year; P = .003) and ICH (0.5%/year vs 0.7%/year; P = .02).
Based on these results, the AHA/ASA provided new recommendations suggesting a benefit of factor Xa inhibitors in patients with nonvalvular AF (class IIa, Level of Evidence B; see Table 1). 12 Patients with AF will usually take 60 mg edoxaban/d, 20 mg rivaroxaban/d, or 10 mg apixaban/d—although lower doses are given for patients with renal impairment. 88 Lower doses for patients with significant renal failure are based on pharmacokinetic data, since patients with low GFR were excluded from the randomized clinic trials.
The Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48 89 trial has substantiated the use of edoxaban in patients with AF (see Table 2). In the trial, 21 105 patients were randomized to 1 of the following groups: warfarin (INR 2-3), high-dose edoxaban (60 mg/d), and low-dose edoxaban (30 mg/d). Patients were included on the basis of documented AF within 12 months of enrollment and excluded on the basis of impaired kidney function, high bleeding risk, mitral stenosis, contraindication for study drugs, or prior stroke within 30 days of enrollment. Enrolled patients were maintained on study drugs for a median of 907 days and followed for a median of 2.8 years. The primary end point was occurrence of stroke (ischemic or hemorrhagic) or any systemic embolic event. Only the high-dose edoxaban treatment group was shown to have a reduced incidence of combined primary outcome compared to warfarin (1.50%/year warfarin vs 1.18%/year high-dose edoxaban; P < .001 for noninferiority). However, both edoxaban groups had reduced incidence of hemorrhagic stroke compared with warfarin (0.47%/year warfarin, 0.26%/year high-dose edoxaban, 0.16%/year low-dose edoxaban; P < .001 for both treatments). Furthermore, both edoxaban groups had lower annual rates of major bleeding (defined as fatal, intracranial, or GI bleeding): 3.43%/year warfarin, 2.75%/year high-dose edoxaban, and 1.61%/year low-dose edoxaban; P < .001 for both comparisons. Edoxaban is not approved for patients with GRF >95 mL/min or < 15 mL/min.
DOAC Reversal Therapy
Despite the aforementioned advantages of DOACs, there is still a need for adequate reversal therapies—particularly in cases of major bleeding. 90 Unlike warfarin, which can be simply reversed by administering vitamin K, there are fewer options available to counteract DOACs. Currently, idarucizumab and prothrombin complex concentrate (PCC) are the only FDA-approved DOAC reversal agents. 91 Idarucizumab is a monoclonal antibody that reverses dabigatran. The PCC is a combination of a variety of clotting factors and has shown promising results in reversing DOACs such as rivaroxaban and apixaban. 92 Clinical trials are ongoing for other DOAC inhibitors including andexanet alfa and ciraparantag. 93
The Role of Imaging in Stroke Prevention
Imaging plays a significant role in stroke prevention by identifying possible sources of embolism and also the severity of cerebrovascular pathology. 94 Transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) have been widely used for stroke prevention in patients with AF. While TTE provides anatomic information and identifies predisposing anomalies to the development of AF, TEE is more useful in stroke prevention as it can detect blood stasis, left atrial (LA) enlargement, or thrombus formation with high sensitivity and specificity. 95 Blood stasis can be classified by an imaging spectrum ranging from spontaneous echo contrast (SEC) to sludge. The SEC represents a low-flow state with increased thromboembolic risk. Sludge, an echodensity without discrete mass on ultrasound, represents thrombus in situ. 96 The presence of LA thrombus on TEE is associated with a 10.4% risk of embolism and 15.8% risk of death per year, irrespective of OAC use. 97 Additionally, the SPAF trial demonstrated the utility of TEE in detecting descending aortic plaques that increase thromboembolic risk. 98
The indications for duplex ultrasound have been summarized by the Guidelines on the Management of Patients with Extracranial, Carotid, and Vertebral Artery Disease. 99 Ultrasound is not recommended for screening of atherosclerotic disease in asymptomatic patients. When standard physical examination of an asymptomatic patient reveals the presence of a carotid bruit, which is suggestive of carotid atherosclerotic disease, ultrasound is indicated to further quantify the degree of stenosis (class IIa, Level of Evidence C). It is appropriate to evaluate lesion progression annually with ultrasound if the initial examination reveals greater than 50% stenosis. In the setting of symptomatic vertebrobasilar artery disease, magnetic resonance angiography or computed tomography angiography are preferred over ultrasound to assess posterior circulation flow. 99 Limitations of ultrasound include dependence on operator experience and patient anatomic variability. Cerebral angiograms can provide excellent resolution for imaging vascular abnormalities and pathology. However, the relatively invasive nature of cerebral angiogram makes it suitable only under certain conditions such as planning for endovascular procedures or postoperative procedures. Therefore, the importance of noninvasive imaging as a first-line measure in the prevention of stroke is evident. As clinical trials continue to guide screening efforts, great preventative measures will continue to be a focus of medical management.
Future Research
Prior proof-of-concept in vitro experiments have demonstrated the superiority of triple antiplatelet therapy in platelet aggregation. 100 Consequently, the triple antiplatelets for reducing dependency after ischemic stroke (TARDIS) trial 101,102 is an ongoing phase III clinical trial that may determine the utility of using triple antiplatelet therapy for noncardioembolic secondary stroke prevention in a non-Asian population. Enrolled patients (n = 4100) will be assigned to one of the following treatment groups for 30 days: triple therapy (aspirin, dipyridamole, and clopidogrel), dual therapy (aspirin and dipyridamole), or monotherapy (clopidogrel). The primary outcome for this study will be recurrence/severity of stroke within 90 days, and the secondary outcomes will be occurrence of bleeding, disability, vascular events, or death within 90 days.
Polypills may provide as a new method of reducing strokes within a general population. 103 Polypills contain a combination of several medications that aim to generally reduce hypercholesterolemia and hypertension—2 conditions that greatly increase the risk of stroke. Since they are only taken once daily, there is a greater chance that patients will comply to therapy. Furthermore, the cost of polypills could be reduced significantly since many of the drugs have generics. Polypill concoctions would be based on preexisting conditions, such as CAD. For instance, patients with no prior CAD could benefit from a polypill containing pravastatin, amlodipine, and valsartan. On the other hand, patients with CAD could take a polypill containing aspirin, atorvastatin, atenolol, amlodipine, and valsartan. 103 Future clinical trials will need to be conducted in order to establish the efficacy of polypills.
Conclusions
Being one of the leading causes of death in the United States, stroke is a debilitating disease. 104 Individuals who survive a stroke often face long-lasting health and financial consequences. Commonly used antiplatelet medications include aspirin, clopidogrel, and aggrenox, while a commonly used anticoagulant is warfarin. Clinical use of DOACs (including rivaroxaban, apixaban, edoxaban, and dabigatran) has provided a promising alternative to warfarin therapy. The DOACs offer a major advantage over warfarin therapy by decreasing the risk of ICH, eliminating the need to adjust the dosing for targeted INR range, and patients do not need to implement dietary restrictions. 13 Due to their shorter half-lives, however, patients taking DOACs must be more rigorous in following their prescribed regimen. 13 Each drug has a separate mechanism of action and under certain circumstances may be recommended over other treatment options. As such, clinicians must carefully weigh the relative benefits with potential side effects when deciding an appropriate treatment regimen.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.