
Abstract
Objective: We evaluated the current evidence on the association between migraine, including aura status, and cervical artery dissection.
Methods: We performed a systematic review and meta-analysis of studies investigating the association between migraine or migraine subtypes (e.g. migraine with aura) and cervical artery dissection published through October 2010.
Results: We identified five case-control studies investigating the association between migraine and cervical artery dissection. In pooled analysis, migraine doubled the risk of cervical artery dissection (pooled odds ratio [OR] = 2.06, 95% confidence interval [CI] 1.33–3.19). All studies allowed evaluation of migraine aura status. While the effect estimate for migraine without aura (pooled OR = 1.94, 95% CI 1.21–3.10) was similar to overall migraine, the association was weaker for migraine with aura (pooled OR = 1.50, 95% CI 0.76–2.96). However, there is no evidence that aura status significantly modifies the association between migraine and cervical artery dissection (meta-regression on aura status p = .58). The risk does not appear to differ between women and men; however, only few studies presented gender-specific data. Heterogeneity among studies was low to moderate.
Conclusion: In this meta-analysis migraine is associated with a two-fold increased risk of cervical artery dissection. This risk does not appear to significantly differ by migraine aura status or gender.
Keywords
Introduction
Migraine is a common disorder affecting approximately 18% of the female population and 6% of the male population (1). Clinically it presents with severe headache attacks and vegetative symptoms. About one-third of migraineurs experience transient neurological symptoms mostly involving the visual system prior to or during the migraine attack, known as migraine aura (2).
Migraine physiology is incompletely understood. While the condition is mainly considered to be a functional disorder of the brain, there are clear links to the vascular system. For example, endothelial dysfunction and hypercoagulability (3) as well as altered vascular reactivity (4) are among the findings in patients with migraine. In addition, migraine, especially migraine with aura, has been shown to increase the risk of ischemic stroke (5). All these associations are particularly strong among younger people and women.
The mechanisms behind the increased risk of ischemic stroke among patients with migraine are not fully understood. One plausible link may be cervical artery dissection (CAD) (6), as CAD is one of the leading causes of ischemic stroke in the young (7). The association between migraine and CAD has been suggested by case series (8,9) and also in some case-control studies (10–13), while another study did not find such an association (14). Further, it is unclear if the risk differs by migraine aura status. The association between migraine and many co-morbidities, for example, cardiovascular events and depression, is particularly strong among those suffering from migraine with aura (15). However, in studies looking at the association between migraine and CAD, the number of patients with migraine with aura was small, obviating firm conclusions (11–14).
The aim of this study was to summarize the current evidence on the association of migraine and migraine aura status with CAD by systematically reviewing the literature and performing a meta-analysis.
Methods
To perform this meta-analysis, we used the guidelines published by the Meta-analysis of Observational Studies in Epidemiology (MOOSE) group for the design, performance and reporting of meta-analyses of observational studies (16).
Data sources and searches
Two investigators (P.M.R., M.S.) independently searched MEDLINE, EMBASE and the Science Citation Index from their inceptions through October 2010 using the terms “headache”, “migraine disorders” or “migraine” combined with the terms “vertebral artery dissection”, “carotid artery dissection”, “cervical artery dissection”, “artery dissection” or “carotid artery injury”. The “explode” feature was used where applicable and no language restrictions were applied. We also manually searched the reference lists of all primary and review articles.
Study selection
A priori, we established the following inclusion criteria. First, the studies must have a case-control or cohort design. Second, the studies must investigate patients with CAD and control subjects without dissection. Third, migraine must be diagnosed according to the criteria established by the International Headache Society (IHS) (17,18). Fourth, in their analyses the authors must use a multivariable model or matching procedure that controls for potential confounding. Fifth, the study must provide effect estimates with 95% confidence intervals (CIs) or enough data to calculate these. Finally, if studies had overlapping cases and/or controls, the largest study with extractable data meeting all the other inclusion criteria was included.
To determine which studies to include, two investigators (P.M.R., M.S.) screened the titles and abstracts of all studies identified in the literature search and by consensus excluded all studies that did not meet any of the pre-specified criteria. The same investigators then reviewed the full articles of the remaining studies and excluded any studies not meeting our inclusion criteria.
Data extraction
Two investigators (P.M.R., M.S.) independently extracted data and entered them into a customized database. All disagreements were resolved by consensus. The extracted data included the authors’ names and title of the study, country the study was performed in, year of publication, study design, source population, study size, age and gender distribution of participants, method of diagnosing CAD, criteria used for migraine diagnosis, migraine status including aura, number of migraineurs among patients with dissections and controls, and effect estimates and 95% CIs.
Statistical analysis
We included all studies regardless of their gender and age distributions. We performed an overall analysis of the association between migraine and CAD. We also performed stratified analyses by migraine aura status (migraine with aura and migraine without aura) and by gender.
For each study we weighted the log of the odds ratio (OR) by the inverse of its variance to obtain pooled relative-risk estimates. For studies that did not present ORs and 95% CIs (11,14,19), we calculated these based on the numbers of migraineurs and non-migraineurs among patients with and without CAD. We decided to run random effect models, because they include assumptions about potential differences between studies as opposed to fixed effects models. We performed the DerSimonin and Laird Q test for heterogeneity. Additionally, we also calculated the I2 statistic (20). To visually examine the impact of individual studies on the overall homogeneity of the test statistic, we constructed Galbraith plots (21). Meta-regression was used to statistically evaluate the extent of heterogeneity due to migraine aura status and reported method of diagnosing CAD. Finally, to test for small study effects (e.g. publication bias), we used statistical methods described by Begg and Mazumdar (22) and Egger (23).
A two-tailed p value <0.05 was considered statistically significant and all analyses were carried out using SAS v.9.1 (SAS Institute, Cary, NC, USA) and STATA v.10.1 (Stata, College Station, TX, USA).
Results
Figure 1 summarizes how studies were selected for inclusion in this meta-analysis. The electronic search identified 970 references. After reviewing the titles and abstracts and excluding those not meeting our inclusion criteria, we were left with 10 references. Of these, after evaluating the full references, three were excluded because they were conference abstracts and later published as full papers (24–26), and one was excluded because it did not investigate migraine (27). One additional paper was excluded from the main analysis because the authors did not present adjusted ORs and patients with CAD were not matched to controls (19); however, we used data from this paper for sensitivity analysis. No additional articles were identified when we manually searched the reference lists of all included articles, leaving a total of five articles for inclusion in this meta-analysis (10–14).
Process of selecting studies.
Study characteristics and individual study results
Characteristics of case-control studies investigating the association between migraine and cervical artery dissection

CAD = cervical artery dissection. IHS = International Headache Society. IHS 1 = diagnostic criteria according to IHS 1988. IHS 2 = diagnostic criteria according to IHS 2004. MA = migraine with aura. MO = migraine without aura. MRI = magnetic resonance imaging. MRA = magnetic resonance angiography. NS = not specified.
Overlapping population with Pezzini et al. 2005 (12), but larger. Adjusted odds ratios for this study are not available. Study only used for sensitivity analysis.
Results for this control group are not used for the pooled analysis.
Association between migraine and cervical artery dissection in individual studies
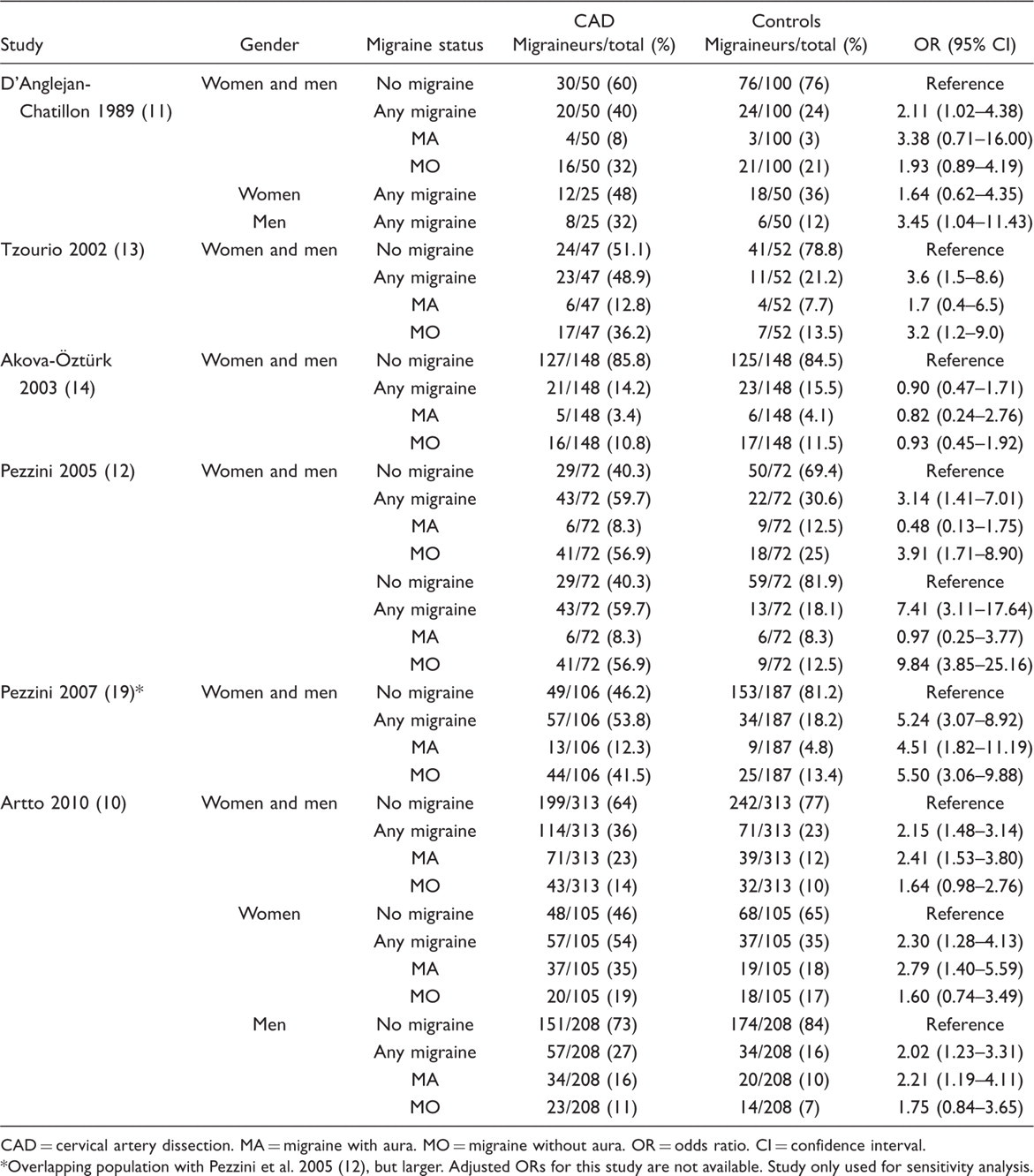
CAD = cervical artery dissection. MA = migraine with aura. MO = migraine without aura. OR = odds ratio. CI = confidence interval.
Overlapping population with Pezzini et al. 2005 (12), but larger. Adjusted ORs for this study are not available. Study only used for sensitivity analysis.
The study by D’Anglejan-Chatillon et al. enrolled 25 men and 25 women with extracranial internal carotid and vertebral artery dissection unrelated to obvious neck trauma (11). The control group consisted of the 50 spouses of the patients and 50 friends of the same age and sex as the patients. The authors found a significant difference in the proportion of patients who experience migraine compared to the controls. We calculated ORs based on the data provided in the manuscript.
Tzourio et al. performed a hospital-based case-control study in two neurology departments in France (13). A total of 47 patients with CAD were consecutively recruited as were 52 control patients who were hospitalized in the same centers during the same time period for an ischemic stroke or a transient ischemic attack (TIA) unrelated to CAD and were comparable to case subjects in sex and age (± five years). They found that patients with any migraine or migraine without aura were at significantly increased risk of CAD. Patients with migraine with aura also appeared to have an increase in their risk, but this increase was not statistically significant.
Akova-Öztürk performed a case-control study at a university hospital in Germany (14). They recruited 148 patients with CAD and matched them by age and gender to individuals free of CAD who were family members, friends and clinic staff. Neither the provided ORs for any migraine nor our calculated ORs for migraine subtypes suggested an association with CAD.
Pezzini et al. also performed a hospital-based case-control study in which they enrolled 72 consecutively admitted patients with spontaneous CAD (12). Two separate control groups were selected. One consisted of age- and sex-matched patients with ischemic stroke unrelated to CAD consecutively admitted during the same time period as the cases. The second control group was age- and sex-matched hospital staff with no known history of vascular disease. When comparing the cases to either control group, a significant increase in risk of CAD was seen for those with any migraine and migraine without aura, but a non-significant decrease in risk was seen for those who experience migraine with aura. For our analysis we included the results comparing patients with spontaneous CAD to patients with ischemic stroke unrelated to CAD for the following reasons: First, this approach resembles the study design by Tzourio et al. (13). Second, stroke patients without CAD may have a higher prevalence of migraine than healthy hospital staff; hence, estimates for the migraine-CAD association are more conservative. Third, stroke patients with and without CAD are more likely to originate from the same catchment area around the hospitals than patients and hospital staff.
The same group presented data on a larger number of cases and controls as part of another analysis (19), which allowed us to calculate the crude association between migraine and CAD. However, since we could not determine ORs adjusted for potential confounders, we only used this study for sensitivity analysis.
Using a Finnish database for CAD patients, Artto et al. enrolled 313 patients for whom information on migraine status could be obtained (10). Control subjects were recruited randomly from the Finnish Population Register Center and were frequency-matched to the cases on age (five-year intervals) and sex. Among CAD patients, the average follow-up time before the interview to establish migraine diagnosis was 3.5 years. The authors observed a statistically significant increase in the risk of CAD for those who experience migraine with aura. The increase in risk among those with migraine without aura was not statistically significant.
Results from the pooled analysis
Table 3 shows the results from our pooled analysis along with measures of heterogeneity and small study effects. After pooling the results from our five included studies, we observed a statistically significant increase in the risk of CAD among participants who experience any migraine (pooled OR = 2.06, 95% CI 1.33–3.19) (Figure 2). When we stratified our analysis by migraine aura status, a significant increase in the risk of CAD was apparent only for migraine without aura (pooled OR = 1.94, 95% CI 1.21–3.10) (Figure 3) While the pooled results also suggested an increased risk for CAD among migraineurs with aura, this was not significant (pooled OR = 1.50, 95% CI 0.76–2.96) (Figure 4). However, meta-regression did not identify aura status as a significant source of heterogeneity (p = 0.58); hence, there is no indication that aura status significantly modifies the association between migraine and CAD.
Odds ratios for cervical artery dissection (CAD) among patients with any migraine from the individual studies and from the pooled analysis. ES = estimate (indicates odds ratio). CI = confidence interval. Odds ratios for cervical artery dissection (CAD) among patients with migraine without aura from the individual studies and from the pooled analysis. ES = estimate (indicates odds ratio). CI = confidence interval. Odds ratios for cervical artery dissection (CAD) among patients with migraine with aura from individual studies and from the pooled analysis. ES = estimate (indicates odds ratio). CI = confidence interval. Association between migraine and CAD from random effects model, heterogeneity and small study effects OR = odds ratio. CI = confidence interval. Q = Cochran’s Q. df = degrees of freedom.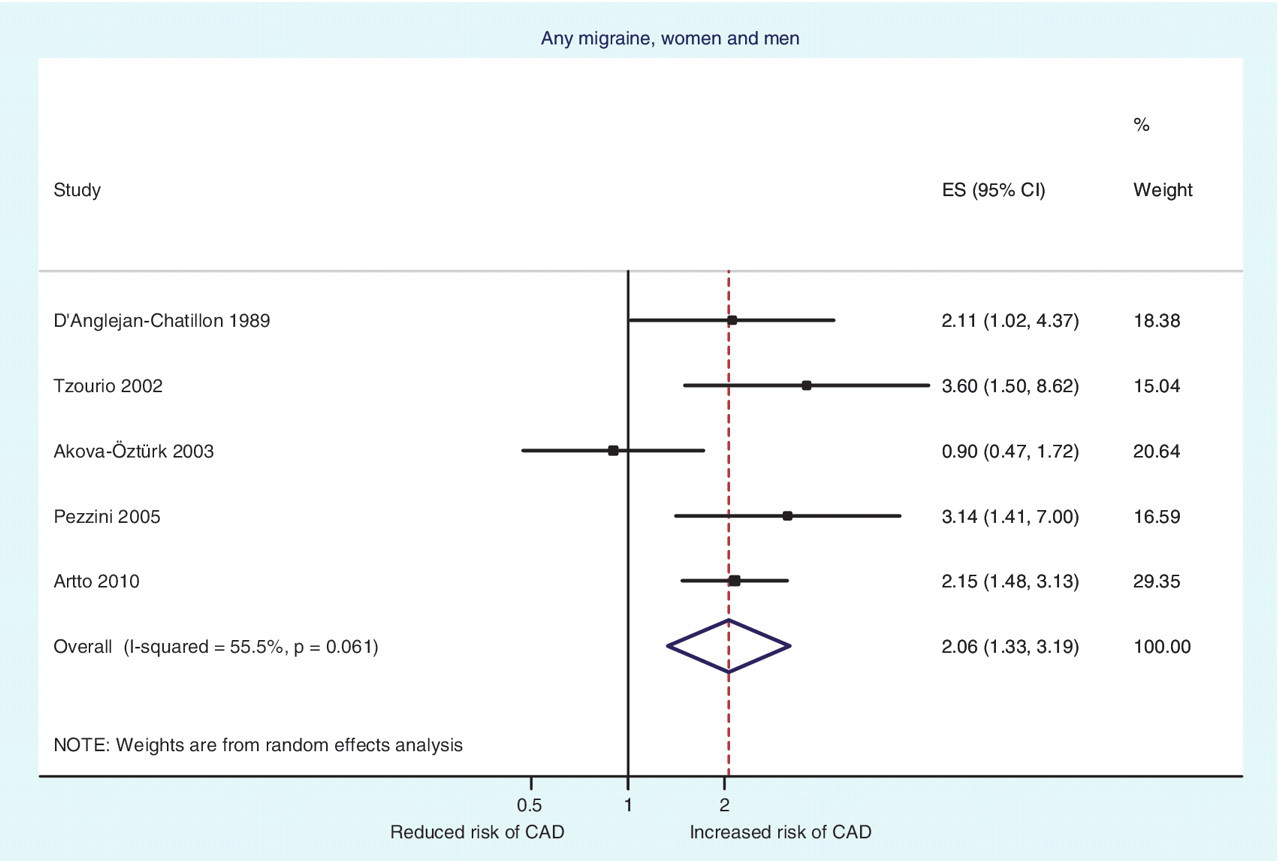



Gender stratified data are available from only two studies and the pooled analyses do not suggest a different effect for the association between any migraine and CAD by gender (women: pooled OR = 2.10, 95% CI 1.27–3.47; men: pooled OR = 2.18, 95% CI 1.38–3.45).
Heterogeneity among the included studies for all analyses was low to moderate and there was no evidence for small study effects in formal investigations with Begg and Egger’s tests (all p values > 0.14). Meta-regression showed that type of CAD diagnosis (duplex + MRI and MR angiography [MRA] and/or conventional angiography versus no details given) was not a significant source of heterogeneity in any of our analyses (p values >0.24)
Sensitivity analyses
For our first sensitivity analysis, we included the larger study by Pezzini et al. from 2007 (19), which did not allow us to determine adjusted ORs, and excluded the smaller study from 2005 (12). We observed results similar to our main analysis, the pooled effect estimates being somewhat higher (any migraine: pooled OR = 2.38, 95% CI 1.34–4.21; migraine with aura: pooled OR = 2.37, 95% CI 1.46–3.84; migraine without aura: pooled OR = 2.19, 95% CI 1.16–4.13). These results further support that the migraine-CAD association does not differ according to migraine aura status.
We further used Galbraith plots to identify individual studies that may be potential sources of heterogeneity. We excluded any study that fell outside the margin set by two standard deviations of the z-score and re-ran our analysis. For the association between any migraine and CAD, the study by Akova-Öztürk (14) was identified and exclusion of this study yielded higher pooled-effect estimates than our main analysis (pooled OR = 2.39, 95% CI 1.78–3.91). With regard to the association of migraine with aura and CAD, the study by Pezzini et al. (12) was identified as a potential source of heterogeneity. Excluding this study gave results similar to the main analysis (pooled OR = 2.12, 95% CI 1.40–3.20). For the association between migraine without aura and CAD, Galbraith plots did not suggest any of the studies as sources of heterogeneity.
Discussion
This meta-analysis shows that any migraine increases the risk of CAD by two-fold. There is no strong evidence that migraine aura status significantly modifies this association. Results do not appear to differ between women and men; however, the number of studies with gender-stratified data was small.
Most (8–13) but not all (14) available studies have suggested that migraine increases the risk for CAD. Furthermore, the study results were inconsistent with regard to potential modifying effects of migraine aura status or gender (Table 2). In particular, the association between migraine with aura and CAD could not be reliably assessed due to the low number of migraineurs with aura in individual studies. Some of the inconsistencies in the results may derive from differences among control groups (Table 1). Population-based controls, matched to CAD patients by age and gender, may be considered the most appropriate control group (6). In contrast, for example, stroke patients without CAD may have a higher prevalence of migraine than healthy hospital staff or population-based controls and may also differ with respect to other vascular risk factors. This may result in an underestimation of the migraine-CAD association. Furthermore, hospital staff may differ with respect to their health status from CAD patients and may not be representative of the catchment area from which patients originate. This may result in an overestimation of the migraine-CAD association. Differences in results in the study by Pezzini et al. (12) for the two control groups illustrate these issues. However, differences in the control groups do not introduce high overall heterogeneity (Table 3).
Our pooled results firmly suggest that the risk for CAD is doubled for any migraine, a finding supported by low-to-medium heterogeneity among the studies (Table 3) and robustness in sensitivity analyses. The associations were driven by migraine without aura, the largest subgroup in all but one study (10). The results for migraine with aura also show an increased risk of CAD. Although this was not statistically significant in the main analysis, meta-regression did not identify aura status as a significant source of heterogeneity and sensitivity analyses do indicate a statistically significant association with the same order of magnitude as seen for migraine without aura.
The exact mechanisms behind the association between migraine and CAD are unclear, but vessel pathologies are plausible linking factors. First, endothelial dysfunction, which may in part be genetically determined – for example, by the insertion/deletion polymorphism in the angiotension-converting enzyme gene–has been reported in migraineurs (3) and may account for the altered systemic vascular reactivity among migraine patients (4). Such vessel-wall pathologies are also among the most important risk factors for CAD. For example, an increased aortic root diameter and increased relative diameter change of the common carotid artery during the cardiac cycle increase the odds of CAD by 14- and 10-fold, respectively (6). Second, biological evidence is provided by studies suggesting that migraine and CAD share common genetic susceptibility factors such as the 677C > T variant in the gene coding for the methylenetetrahydrofolate reductase (19,28,29). Third, the activity of serum elastase, a metallo-endopeptidase involved in the extracellular matrix degradation, is increased among migraineurs (30), providing one physiological explanation for the increased risk of CAD we observed.
The association between migraine and CAD may be one explanation for the increased risk of cerebral ischemic events, especially among young migraineurs. A recent meta-analysis has firmly established a link between migraine and cardiovascular events, especially ischemic stroke (5), an association that appears to be independent of classical cardiovascular risk factors (31) and particularly strong among people without most cardiovascular risk factors (32). This association may extend to sub-clinical brain lesions. MRI studies have reported an increased risk for sub-clinical brain lesions in areas supplied by the posterior (33,34) and anterior (35) circulation, mostly for migraine with aura (34,35).
The following limitations should be considered. First, two included studies did not specify the methods used to diagnose CAD in their participants (10,14), leaving the potential for misclassification. However, meta-regression did not identify this as a source of heterogeneity. Second, the clinical spectrum of migraine is wide and it is possible that some participants may have been misdiagnosed. However, all studies used standardized methods for migraine diagnosis strictly adhering to the criteria established by the International Headache Society (17,36). Third, we used only data that were extractable from the papers and did not contact authors for additional data. All studies allowed us to determine measures of association for any migraine as well as migraine subtypes and CAD. Only two studies presented gender-stratified results (10,11); hence, our pooled analysis leaves some remaining uncertainties. However, there is no a priori reason to believe that the biological link between migraine and CAD differs between women and men and results from the available studies do not suggest a differential effect by gender (Tables 3). Finally, the available studies do not definitively establish the direction of association. Most studies did not specify the temporal relationship between CAD diagnosis and migraine diagnosis, and one study reported an average follow-up time of 3.5 years after CAD diagnosis before the interview to establish migraine diagnosis (10). Headache and neck pain with various characteristics may be the initial and only signs of CAD in about 8% of patients (37,38). Among those, some patients may have migraine-like headaches; however, by three months after CAD patients are typically pain free (37,38). Given this small prevalence of CAD patients with migraine-like headaches, and because diagnosis of migraine according to IHS criteria requires multiple attacks separated by pain-free episodes (36), it is unlikely that a migraine-like headache will be misdiagnosed as an overt migraine.
In summary, the increased risk for CAD among migraineurs appears to be well-supported by available evidence. This association does not appear to differ by migraine aura status or gender.
Footnotes
Funding
There was no specific funding for this study. P. Rist is supported by a T-32 training grant from the US National Institutes of Health (NIH; AG 00158).
Full disclosures for the last five years
P. Rist is supported by a T-32 training grant from the US National Institutes of Health (NIH; AG 00158).
Dr Diener has received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Addex Pharma, Allergan, Almirall, AstraZeneca, Bayer Vital, Berlin Chemie, Coherex, CoLucid, Böhringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline (GSK), Grünenthal, Janssen-Cilag, Eli Lilly, La Roche, 3M Medica, Medtronic, Minster, MSD, Novartis, Johnson & Johnson, Pierre Fabre, Pfizer, Schaper and Brümmer, SanofiAventis and Weber & Weber. Financial support for research projects was provided by Allergan, Almirall, AstraZeneca, Bayer, GSK, Janssen-Cilag and Pfizer. Headache research at the Department of Neurology in Essen is supported by the German Research Council (DFG), the German Ministry of Education and Research (BMBF) and the European Union. Dr Diener has no ownership interest and does not own stocks of any pharmaceutical company.
Dr Kurth has received investigator-initiated research funding from the NIH, McNeil Consumer & Specialty Pharmaceuticals, Merck and Wyeth Consumer Healthcare; he is a consultant to i3 Drug Safety and World Health Information Science Consultants, LLC, and he has received honoraria from the American Academy of Neurology, Genzyme, Merck and Pfizer for educational lectures.
Dr Schürks has received investigator-initiated research grants from the German Research Foundation and the Migraine Research Foundation. He has received honoraria from L.E.K. Consulting for telephone surveys and from the American Academy of Neurology for educational material.