
Abstract
Controversy persists regarding the safety and efficacy of an accelerated low-dose recombinant tissue-type plasminogen activator (rt-PA) regimen for reperfusion therapy in acute pulmonary embolism. This study describes the outcomes of an accelerated low-dose rt-PA regimen for the treatment of acute pulmonary embolism in Vietnamese patients. This was a case series from October 2014 to October 2020 from 9 hospitals across Vietnam. Patients presenting with acute pulmonary embolism with high to intermediate mortality risk were administered alteplase 0.6 mg per kilogram (maximum of 50 mg) over 15 min. The main outcomes were the proportion who survived to hospital discharge and at 3 months as well as in-hospital hemorrhage (major and minor according to International Society of Thrombosis and Hemhorrage definitions). A total of 80 patients were enrolled: 48 (60%) with high risk for mortality and 32 patients (40%) with intermediate risk for mortality. A total of 7 (8.8%) died in hospital. All deaths occurred in the high-risk mortality group. The 73 patients who were discharged alive remained alive at 3 months follow up. During hospitalization, 1 patient (1.3%) suffered major bleeding, and 7 (8.8%) had minor bleeding. An accelerated thrombolytic regimen with alteplase 0.6 mg/kg (maximum of 50 mg) over 15 min for acute pulmonary embolism appeared be effective and safe in a case series of Vietnamese patients.
Keywords
Introduction
Thrombolytic therapy is an established treatment for patients with massive acute pulmonary embolism (PE) and evidence of hemodynamic or cardiac compromise. Thrombolysis reduces the embolic burden and improves cardiorespiratory function.1–5 The US Food and Drug Administration (FDA) approved a fixed full-dose regimen of 100 mg of recombinant human tissue-type plasminogen activator (rt-PA) over 2 h for PE thrombolysis in 1990.1,2
To minimize the risk of catastrophic bleeding associated with thrombolytic agents, several trials have examined the efficacy and safety of reduced dose rt-PA regimens.1,3–5 A retrospective study of patients with PE using thrombolysis (both hemodynamically stable and unstable) demonstrated that patients treated with half-dose alteplase (50 mg) required less vasopressor administration and invasive mechanical ventilation but required escalation of therapy more often than patients treated with full-dose alteplase (rt-PA, 100 mg). 1 In the moderate pulmonary embolism treated with thrombolysis (MOPETT) trial, 121 patients were randomly assigned to receive heparin alone or the combination of lower dose rt-PA plus heparin. This dose of rt-PA was ≤50% of the standard dose (100 mg) for patients weighing 50 kg or more and 0.5 mg/kg for those weighing less than 50 kg. Compared with conventional therapy, this lower dose regimen of rt-PA plus heparin resulted at 28 months in lower pulmonary artery systolic pressures (43 ± 6 vs 28 ± 7 mm Hg) and faster resolution of pulmonary hypertension (50 ± 6 mm Hg vs 51 ± 7 mm Hg on admission; 43 ± 6 mm Hg vs 28 ± 7 mm Hg at 28 months).6
Another regimen proposed is bolus or accelerated-dose with 0.6 mg of rt-PA per kg body weight (maximum of 50 mg) over 15 min delivered intravenously. 2 In a direct comparison study, no significant differences were detected between the bolus rt-PA and 2-h rt-PA infusion with respect to bleeding complications, adverse clinical events, or imaging studies. 2 There was less fibrinogenolysis with the bolus dosing regimen. 7 Some clinical cases had been reported with successful outcomes using this regimen for PE patients with cardiac arrest.1,8 Therefore, the European Society of Cardiology recommended 2 regimens: full-dose and accelerated-dose rt-PA. 2 However, the comparison of the 2 regimens of alteplase for efficacy and safety requires further study. Wang et al 5 reported a multicenter randomized controlled trial from China in 118 patients that found similar efficacy between half dose and full dose thrombolysis with reduced major bleeding rate in the subgroup of older patients. The aim of this study was to examine the outcomes from using the accelerated regimen with low-dose rt-PA for treatment of acute pulmonary embolism in a multicenter observational study in Vietnam.
Materials and Methods
Study Design and Participants
This was a cohort study.
This research was carried out from October 2014 to October 2020 in 9 major Vietnam hospitals: Hanoi Medical University Hospital, Bach Mai Hospital, Thu Duc District Hospital, Saint Paul Hospital, Hanoi Heart Hospital, Ninh Binh Provincial General Hospital, Phu Tho Provincial General Hospital, Ha Nam Provincial General Hospital and 103 Military Hospital.
Absolute: (1) History of hemorrhagic stroke or stroke of unknown origin, (2) ischaemic stroke in previous 6 months, (3) central nervous system neoplasm, (4) major trauma, surgery, or head injury in previous 3 weeks, (5) bleeding diathesis, and (6) active bleeding. Relative: (7) Transient ischemic attack in previous 6 months, (8) oral anticoagulation, (9) pregnancy or first post-partum week, (10) noncompressible puncture sites, (11) traumatic resuscitation, (12) refractory hypertension (systolic blood pressure >180 mm Hg), (13) advanced liver disease, (14) infective endocarditis, and (15) active peptic ulcer. Patient or delegates did not give consent to thrombolysis treatment.
Indications for Pulmonary Reperfusion with Thrombolysis.

All patients received alteplase 0.6 mg per kg of body weight (maximum 50 mg) intravenously over 15 min. Unfractionated heparin (initial bolus 80 IU/kg then 18 IIU/kg/hr) was commenced 15 min before, and ceased 15 min after the alteplase administration. An activated partial thromboplastin time (aPTT) ratio from 1.5 to 2.3 times the control value was targeted. Any other medication required was at the discretion of the attending physician. The dosage rate of inotropic or vasoactive drug was maintained constant during the period of hemodynamic measurements. The Vasactive-inotropic Score (VIS) was used to measure the severity level of shock. (VIS = dopamine dose [µg/kg/min] + dobutamine dose [µg/kg/min] + 1.00 × adrenaline dose [µg/kg/min] + 100 × noradrenaline dose [µg/kg/min] + 10 × milrinone dose [µg/kg/min] + 10.000 × vasopressin dose [U/kg/min]). 9
Treatment with rt-PA was followed by oral anticoagulation as recommended by the European Society of Cardiology for a period of 3 months. Surviving patients were discharged and re-examined after 3 to 4 weeks then followed up by trained hospital staff monthly for 3 months. Reasons for failure to return for follow-up were ascertained where possible. Transthoracic cardiac Doppler ultrasound was performed to evaluate the right heart function before and 1 day after treatment with thrombolysis, at time of hospital discharge and at 3 months follow up by a cardiac ultrasound specialist. CTPA was performed before treatment and taken at the time of discharge to evaluate the severity index score of PE. 10
The main outcomes of our study were the survival rates at hospital discharge and at 3 months, and in-hospital hemorrhage (major and minor according to International Society on Thrombosis and Haemostasis (ISTH) definitions).11 Other outcome variables collected prospectively included the duration of mechanical ventilation use, vasopressor use duration, hospital length of stay, right ventricular diameter, the pulmonary artery pressure on cardiac Doppler ultrasound and the severity index score of CTPA.
Statistical Methods
Continuous variables were described as mean and standard deviation or median and interquartile range (IQR) if variables were not normally distributed. Categorical data were described as percentages. Proportions were compared by using the χ2 test or Fisher's exact test when expected values in any of the cells were below 5. The level for statistical significance was set at P < .05. Data were analyzed with R software version 3.0.1.
Results
In total, 80 patients were enrolled in this study. There were 55 of 80 (68.8%) female patients. The mean age of patients was 61.6 years ± 18.7 (range 18-95 years). There were 45 of 80 (56.3%) patients who were aged 60 years or older.
There were 48 of 80 (60%) patients at high risk of mortality from their PE and 32 80 patients (40%) at intermediate–high risk of mortality.
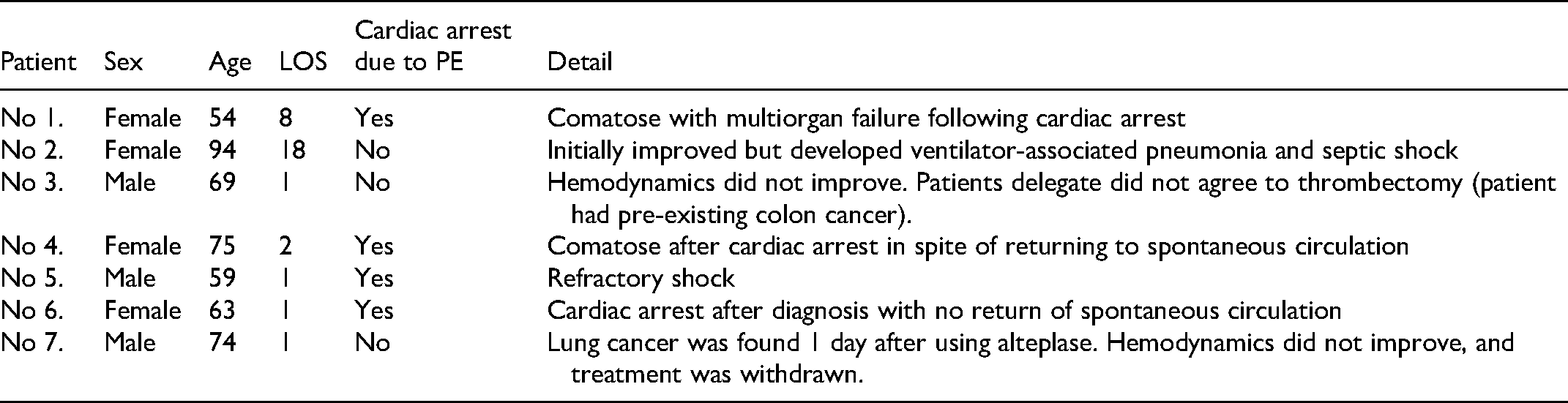
Survival to hospital discharge occurred in 73 of 80 (91.3%). All deaths occurred in the high-risk mortality PE group. The details of each death are shown in Table 2. All 73 patients that were discharged were alive 3 months later.
Characteristics of Patients who Died In-Hospital.
Clinical Course and Adverse Events
In high-risk mortality PE, 23 of 48 (47.9%) patients manifested shock requiring inotropic or vasoactive agents. The median peak of VIS was 34 (interquartile range [IQR] 20-70) most commonly 3 days post admission (IQR 1-6 days). Invasive ventilation was required in 18 of 48 (37.5%) patients for a median of 4 days (IQR 3-7days). A total of 7 of these patients (14.6%) had a cardiac arrest; 5 had return of spontaneous circulation and 4 were discharged without neurological abnormalities. No patient had thrombectomy or percutaneous catheter-directed treatment; Tables 3 and 4.
In-Hospital Adverse Events.

Transthoracic Echocardiography and Computer Tomography Pulmonary Angiogram (CTPA) Before and After Thrombolysis.

The severity index score based on the Quanadli formula: ∑(n·d)/40 } × 100
where n represents the number of affected pulmonary arteries (there are 20 pulmonary arteries; 1 ≤ n ≤ 20 and d is the weighted coefficient of obstruction, where 0 indicates no embolism, 1 partial embolization, and 2 complete embolization. Complete embolization of pulmonary arteries is graded 40 and the severity index equals 100%. 10
There were 2 of 80 (2.5%) patients who developed chronic thromboembolic pulmonary hypertension diagnosed at 3 months follow up.
Discussion
This is the first multicentered study to report on the experience and outcomes of patients treated with an accelerated low-dose thrombolysis regimen for PE in Vietnam. When implementing fibrinolytic agents for treatment of PE in Vietnam, a low-dose regimen was recommended for a number of reasons. First, a lower risk of bleeding was expected.7,12 Second, Vietnamese have lower body weights compared to populations where the original studies were reported. Third, rt-PA is an imported drug considered expensive relative to the health economic conditions of Vietnam. Therefore, reducing the cost of drug dosing is a relevant consideration. The low-dose regimen has now been implemented widely across Vietnam and was recommended by Vietnam National Heart Association and Vietnam National Association of Emergency, Intensive Care Medicine, and Clinical Toxicology.
The survival and major bleeding rates observed in our study compare favorably with previous reports.5,7,12 The pooled survival rate in those 3 studies where 1 group received low-dose regimen group was 96%, with a major bleeding rate of 4%.
There are several limitations to the study. This was a case series without a control group. In addition, the sample size was small.
In conclusion, the accelerated regimen with injection of alteplase at 0.6 mg per kg of body weight (maximum of 50 mg) over 15 min was shown to be effective and safe in a case series of Vietnamese patients with acute high risk and intermediate risk PE.
Footnotes
Authors’ Contributions
BHH conceived and designed the study. BHH, GPD, DLL, NTB, MQN, DAN, and LHN acquired, analyzed, and interpreted the data. BHH and GPD drafted the manuscript. HBH, VTN, LHN, THTB, NTB, MD, RD, and SZG critically revised the manuscript for important intellectual content. HBH and GPD did the statistical analysis. DLL and GPD provided administrative, technical, or material support.
HBH and LHN supervised the study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This trial was approved by The Ethics Committees of Thu Duc District Hospital (Declaration No10/BV-HDDD, September 14th, 2014).