
Abstract

Keywords
Persons with non-O blood group (i.e., A, AB or B) may be at higher risk of venous thromboembolism (VTE) than those with O blood (odds ratio 1.79, 95% CI 1.56 to 2.05). 1 Non-O blood groups may also be predisposed to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 2 During the recent SARS-CoV-2 pandemic, a high rate of VTE was observed among infected patients. 3 Lung tissue specimens from coronavirus disease 2019 (COVID-19) patients showed a preponderance of alveolar capillary microthrombi. 4 A unique COVID-19-associated predisposing coagulopathy (CAC) was proposed. 5 It is not known whether SARS-CoV-2 infected patients with non-O blood groups are especially at higher risk of VTE.
This population-based retrospective cohort study was performed across Ontario, Canada, where health care is universal. Patient-level datasets capturing all inpatients, emergency department and outpatient visits, medical imaging billings, and SARS-CoV-2 laboratory tests were linked using unique encoded identifiers and analyzed at ICES (Table S1). The determination of pulmonary embolism (PE) or deep vein thrombosis (DVT) required a coded diagnosis of either condition, in conjunction with performance of objective imaging (Table S1).
Included were individuals aged 16+ years, who had undergone ABO determination between January 2007 and December 2019,
First, the overall risk of PE or DVT was determined in relation to non-O vs. O blood groups. Next, PE or DVT risk was assessed in association with SARS-CoV-2 positivity vs. negativity. Third, the influence of O blood group was stratified by those with a positive or negative SARS-CoV-2 test.
Cox proportional hazard models generated incidence rates and hazard ratios (HR) and 95% CI, with time zero (t0) first set to the date of ABO testing, and then re-set to the date of SARS-CoV-2 specimen collection. Censoring, starting on the date of SARS-CoV-2 testing, was on death or arrival to the end of the study period of July 31, 2020. HR were adjusted for demographics and comorbidities.
In total, 222,670 individuals were included in the final cohort. Their mean age was 51 years at ABO testing and 54 years at SARS-CoV-2 testing; 71% were female (Table 1). No important differences were seen in the rate of prior VTE, or for any other comorbidities (Table 1).
Characteristics of 222,670 Individuals in Ontario, Canada, With Known ABO Blood Group, and Who Subsequently Underwent SARS-CoV-2 Viral RNA PCR Testing Between January 15, 2020, and June 30, 2020.

All data are presented as a number (%) unless otherwise indicated.
*Non-O blood groups are A, AB and B.
Starting t0 from ABO testing, the aHR was higher for PE (1.14, 1.06 to 1.23) and DVT (1.12, 1.05 to 1.19) comparing O vs. non-O blood groups (Table 2).
Non-O Blood Groups, SARS-CoV-2 Infection, and Their Combination, and Future Risk of Pulmonary Embolism or Deep Vein Thrombosis.
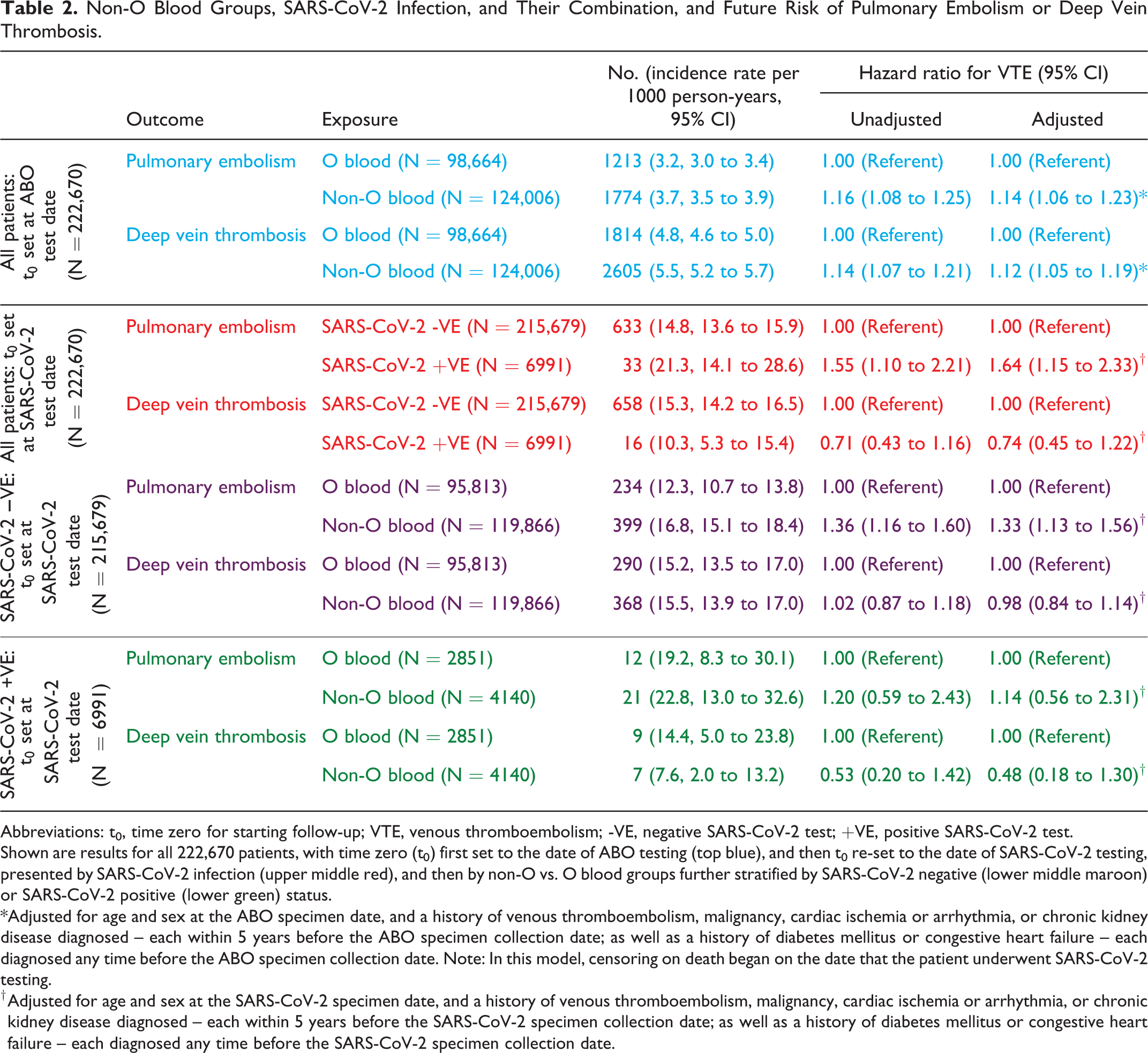
Abbreviations: t0, time zero for starting follow-up; VTE, venous thromboembolism; -VE, negative SARS-CoV-2 test; +VE, positive SARS-CoV-2 test.
Shown are results for all 222,670 patients, with time zero (t0) first set to the date of ABO testing (top blue), and then t0 re-set to the date of SARS-CoV-2 testing, presented by SARS-CoV-2 infection (upper middle red), and then by non-O vs. O blood groups further stratified by SARS-CoV-2 negative (lower middle maroon) or SARS-CoV-2 positive (lower green) status.
*Adjusted for age and sex at the ABO specimen date, and a history of venous thromboembolism, malignancy, cardiac ischemia or arrhythmia, or chronic kidney disease diagnosed – each within 5 years before the ABO specimen collection date; as well as a history of diabetes mellitus or congestive heart failure – each diagnosed any time before the ABO specimen collection date. Note: In this model, censoring on death began on the date that the patient underwent SARS-CoV-2 testing.
† Adjusted for age and sex at the SARS-CoV-2 specimen date, and a history of venous thromboembolism, malignancy, cardiac ischemia or arrhythmia, or chronic kidney disease diagnosed – each within 5 years before the SARS-CoV-2 specimen collection date; as well as a history of diabetes mellitus or congestive heart failure – each diagnosed any time before the SARS-CoV-2 specimen collection date.
Starting t0 from SARS-CoV-2 testing, the overall incidence rate of VTE rose considerably. Those with vs. without SARS-CoV-2 had a higher aHR of PE (1.64, 1.15 to 2.33), but not DVT (0.74, 0.45 to 1.22) (Table 2). The aHR for PE was higher among non-O blood groups in patients without SARS-CoV-2 infection (1.33, 1.13 to 1.56), but not those with SARS-CoV-2 infection (1.14, 95% CI 0.56 to 2.31) (Table 2).
These findings confirm a higher risk of PE and DVT with non-O blood groups. 1 The risk of PE, but not DVT, was elevated in those with SARS-CoV-2, as also suggested elsewhere, possibly due to pulmonary immunothrombi arising in situ. 3,4 Preliminarily, non-O blood group did not appreciably modify the risk of VTE in SARS-CoV-2 positive patients, yet, the number of VTE events was low, producing imprecise risk estimates.
While a coded diagnosis and objective imaging for VTE were required, imaging tests and their reports were not available. This study also did not quantify illness severity among SARS-CoV-2 infected patients, or their receipt of anticoagulants. Those most profoundly affected by the infection may have died prior to SARS-CoV-2 testing, such as from a fatal PE or respiratory failure, so the influence of ABO status among that group could not be determined herein.
Those with O blood group express lower plasma levels of factor VIII and von Willebrand factor, which may protect them against VTE. 1 SARS-CoV-2 infected patients exhibit much higher levels of both of these factors, 5 potentially blunting any protective effect from O blood group. The interaction between these and other blood factors and ABO status in patients with SARS-CoV-2 infection should be properly studied.
Supplemental Material
Supplemental Material, sj-pdf-1-cat-10.1177_10760296211008986 - ABO Blood Group, SARS-CoV-2 Infection, and Risk of Venous Thromboembolism: Population-Based Cohort Study
Supplemental Material, sj-pdf-1-cat-10.1177_10760296211008986 for ABO Blood Group, SARS-CoV-2 Infection, and Risk of Venous Thromboembolism: Population-Based Cohort Study by Joel G. Ray, Marian J. Vermeulen, Michael J. Schull and Alison L. Park in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
MJS, MV: Analysis and interpretation of the data, approval of final version. JGR, AP: Study concept, analysis and interpretation of the data, drafting of manuscript, manuscript revision, approval of final version. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board. Funded by a grant from the Ontario Academic Health Sciences Centre AFP Innovation Fund, and the Ontario Ministry of Health and Long-Term Care.
Acknowledgments
This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Parts of this material are based on data and information compiled and provided by MOHLTC and CIHI. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.