
Abstract
The aim of this study was to describe clinical, imaging, and laboratory features of acute pulmonary embolism (APE) in patients with COVID-19 associated pneumonia. Patients with COVID-19 associated pneumonia who underwent a computed tomography pulmonary artery (CTPA) scan for suspected APE were retrospectively studied. Laboratory data and CTPA images were collected. Imaging characteristics were analyzed descriptively. Laboratory data were analyzed and compared between patients with and without APE. A series of 25 COVID-19 patients who underwent CTPA between January 2020 and February 2020 were enrolled. The median D-dimer level founded in these 25 patients was 6.06 μg/mL (interquartile range [IQR] 1.90-14.31 μg/mL). Ten (40%) patients with APE had a significantly higher level of D-dimer (median, 11.07 μg/mL; IQR, 7.12-21.66 vs median, 2.44 μg/mL; IQR, 1.68-8.34, respectively, P = .003), compared with the 15 (60%) patients without APE. No significant differences in other laboratory data were found between patients with and without APE. Among the 10 patients with APE, 6 (60%) had a bilateral pulmonary embolism, while 4 had a unilateral embolism. The thrombus-prone sites were the right lower lobe (70%), the left upper lobe (60%), both upper lobe (40%) and the right middle lobe (20%). The thrombus was partially or completely absorbed after anticoagulant therapy in 3 patients who underwent a follow-up CTPA. Patients with COVID-19 associated pneumonia have a risk of developing APE during the disease. When the D-dimer level abnormally increases in patients with COVID-19 pneumonia, CTPA should be performed to detect and assess the severity of APE.
Introduction
In December 2019, the novel coronavirus, now known as SARS-CoV-2, rapidly broke out in the city of Wuhan, China, and caused the COVID-19 epidemic, which is not yet fully under control in early 2020. 1,2 During the course of COVID-19 disease, most patients present with mild symptoms, such as fever, cough, and sputum. However, a small proportion of patients rapidly develops acute respiratory distress syndrome (ARDS), acute respiratory failure, and other serious complications. 3,4 As of May 25, 2020, there were 5 304 772 patients diagnosed with COVID-19 worldwide, and 342 029 patients died of this disease. 5 Our hospital was designated to admit COVID-19 patients only and has hospitalized more than 1000 patients.
Elevation of the level of D-dimer in the clinical samples has been observed in some patients with COVID-19. Elevated D-dimer is related to deep vein thrombosis (DVT) and acute pulmonary embolism (APE), and APE might be fatal. However, APE cannot be diagnosed by elevated D-dimer alone, because D-dimer can also be elevated in a series of other conditions such as cancer, peripheral vascular disease, pregnancy, and inflammatory diseases. 6,7 For patients suspected with APE, accurate diagnosis as soon as possible has a significant impact on the treatment strategy and clinical outcomes. 8,9 Due to its high accuracy and convenience, computed tomography pulmonary angiography (CTPA) is an effective imaging technology to detect APE and assess its severity. 10,11
Severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), 2 previous epidemic viral outbreaks caused by a coronavirus, can also lead to ARDS. 1,12 There are little relevant reports on pulmonary embolism in patients with MERS pneumonia, and in only one published paper pulmonary embolism was detected in a patient with SARS using CTPA. 13 Several previous studies reported the finding of elevated D-dimers in patients with COVID-19 associated pneumonia. 1,3,14 However, these studies did not report whether these patients had APE. Recently, APE events were reported in some countries in COVID-19 patients, 15 –19 but little data are available on APE events in patients with COVID-19 from the city of Wuhan, China.
The aim of this retrospective study was to describe clinical, imaging, and laboratory features of APE in patients with COVID-19 associated pneumonia.
Materials and Methods
This study was approved by the Ethical Committee of the Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology (No.202020). The need for patient informed consent was waived because of its retrospective nature.
Patients
Our institution hospitalized 1008 patients with COVID-19 associated pneumonia between January 2020 and February 2020. Considering the huge requirement for noncontrast-enhanced chest computed tomography (CT) and the high transmissibility of SARS-CoV-2, CTPA examination was only performed in a few patients with an elevated D-dimer level or accompanying symptom(s), including chest pain, hemoptysis, and dyspnea. Eventually, 25 consecutive COVID-19 patients who underwent CTPA between January 2020 and February 2020 were retrospectively enrolled in this study. The diagnosis of COVID-19 associated pneumonia was based on the Guidelines for the Diagnosis and Treatment of Novel Coronavirus (2019-nCoV) Infection published by the National Health Commission of China (Trial Version 7). 20 Twenty patients received one or more follow-up D-dimer tests, and 3 patients underwent a follow-up CTPA examination to assess the effect of anticoagulant therapy. The interval between CTPA examination and D-dimer test was less than 2 days.
Computed Tomography Pulmonary Artery Image Acquisition
Computed tomography pulmonary artery examinations were performed on a 128 slice multidetector CT scanners (Philips Ingenuity Core128, Philips Medical Systems) or a 64 slice multidetector CT scanner (Somatom Definition FLASH; Siemens) by using a standard CTPA protocol. The whole chest was craniocaudally scanned from lung apex to the lowest hemidiaphragm for each patient in the supine position. All patients were instructed to hold breath to minimize motion artifacts, and CTPA images were acquired during a single breath-hold. Scan parameters were as follows: tube voltage of 120 kV, tube current of 100 to 300 mAs, collimation of 0.6 to 0.625 mm, pitch of 0.937 to 1.0, table speed of 39.37 mm/s, and gantry rotation time of 0.5 s. The soft tissue reconstruction kernel (iDose4 for iCT, B30f for Definition FLASH) was used. A volume of 50 to 70 mL (calculated based on the patient’s body weight) of nonionic iodinated contrast medium (iopamidol, Iopamiron 370; Bracco) was injected into an antecubital vein at a flow rate of 5.0 mL/s followed by a 25-mL saline flush using a mechanical power injector. For optimal intraluminal contrast enhancement, the automatic bolus-tracking technique had the region of interest positioned at the level of the main pulmonary artery with a trigger threshold of 100 HU. Images were reconstructed with a thickness of 1 mm and an increment of 1 mm or 1.25 mm. The imaging data were transmitted to a post-processing workstation for multiplanar reconstruction and picture archiving and communication systems.
Clinical Data Collection
Relevant clinical and laboratory data were obtained from electronic medical records. The interval between CTPA examination and laboratory data selected was less than 2 days. We collected clinical data on age, gender, time to CTPA, any comorbidity (hypertension, diabetes, cardiovascular disease, malignancy, DVT, surgery, and smoking), outcome, laboratory values (D-dimer, C-reactive protein, white blood cell count, lymphocyte count, brain natriuretic peptide, alanine aminotransferase, aspartate transaminase, glutamyl transferase, albumin, globulin, creatinine, blood urea nitrogen, arterial partial pressure of carbon dioxide [PaC
Image Interpretation
All CT and CTPA image analysis were performed by 2 radiologists experienced in thoracic radiology (Y.X., with 20 years of experience; X.W., with 22 years of experience), who were blinded to the clinical information. Disagreements were resolved through discussion until consensus was reached. Based on previously published articles, 22 4 stages of lung involvement were defined based on CTPA images at lung widow: (1) early stage, (2) progressive stage, (3) peak stage, and (4) absorption stage. The lung window was set with a width of 1500 HU and level of −700 HU. In addition, all CTPA images were analyzed using the mediastinal window setting (width, 250 HU; level, 50 HU). The anatomical sites of the APE were recorded.
Statistical Analysis
Continuous variables were expressed as median with its interquartile range (IQR) and compared with the Mann-Whitney U test. Categorical variables were described as number (%), and proportions of categorical variables were compared using the Fisher exact test. The rate of moderate and severe type was compared between the APE group and non-APE group with Fisher exact test. The rate of progression and peak stages was compared between APE group and non-APE group with Fisher exact test. A 2-sided α of less than .05 was considered statistically significant. Statistical analyses were done using the SPSS version 21.0 software (IBM).
Results
Clinical Characteristics of COVID-19 Patients With Suspected APE
A total of 25 patients (15 males and 10 females) were retrieved from medical records. All patients who underwent CTPA scans had elevated D-dimer levels, and most of the patients had some accompanying symptoms related to suspected APE (20 with dyspnea, 4 with chest pain, and 4 with hemoptysis). The median age was 65 years old (IQR, 56-70; range, 36-78 years). Fifteen patients were diagnosed positive for SARS-CoV-2 infection by real-time reverse transcription–polymerase chain reaction (RT-PCR) during hospitalization, while 10 patients with a negative in RT-PCR test were confirmed by immunoglobulin G/immunoglobulin M detection after discharge. Five (20%) patients had moderate, and 20 (80%) patients had severe disease according to the COVID-19 classification. Based on the lung window of the CTPA images, 3 (12%) patients were at the progressive stage, 16 (64%) were at the peak stage, and 6 (24%) were at the absorption stage. Several comorbidities were detected, including hypertension (40%), diabetes (20%), and cardiovascular disease (16%). By April 10, 2020, 19 patients were discharged and 6 patients died. Relevant clinical and radiological details are presented in Table 1.
Clinical Characteristics of COVID-19 Patients With Suspected APE.a

Abbreviations: APE, acute pulmonary embolism; CVDs, cardiovascular diseases; CTPA, computed tomography pulmonary artery; DVT, deep vein thrombosis; IQR, interquartile range.
a Data are median (IQR) or n (%). The rate of moderate and severe type compared with Fisher exact test between APE group and non-APE group. The rate of progressive and peak stages compared with Fisher exact test between APE group and non-APE group.
Laboratory Data of COVID-19 Patients With Suspected APE
An increased D-dimer level (median, 6.06 μg/mL; IQR, 1.90-14.31 μg/mL) was detected in all 25 patients. Ten patients were APE positive according to the CPTA images and had a median D-dimer value of 11.07 μg/mL (IQR, 7.12-21.66). Fifteen patients were APE negative and have a median D-dimer value of 2.44 µg/mL (IQR, 1.68-8.34). There was a significant difference in D-dimer levels between both groups (P < .05). The CRP level was elevated in 21 (84%) patients. White blood cell count was elevated in 5 (20%) patients and decreased in 2 (8%) patients. Lymphocyte count was decreased in 19 (76%) patients, and normal in 6 (28%) patients. B-type brain natriuretic peptide was elevated in 16 (64%) cases. Albumin was decreased, with a lowered ratio of albumin to globulin in almost all patients. Arterial blood gas analysis showed a low Pa
Laboratory Data of COVID-19 Patients With Suspected APE.

Abbreviations: Alb, albumin; ALT, alanine aminotransferase; APE, acute pulmonary embolism; AST, aspartate transaminase; BNP, brain natriuretic peptide; BUN, blood urea nitrogen; Cr, creatinine; CRP, C-reacted protein; CVDs, cardiovascular diseases; DVT, deep vein thrombosis; GGT, glutamyl transferase; Glb, globulin; IQR, interquartile range; LC, lymphocyte count; PaC
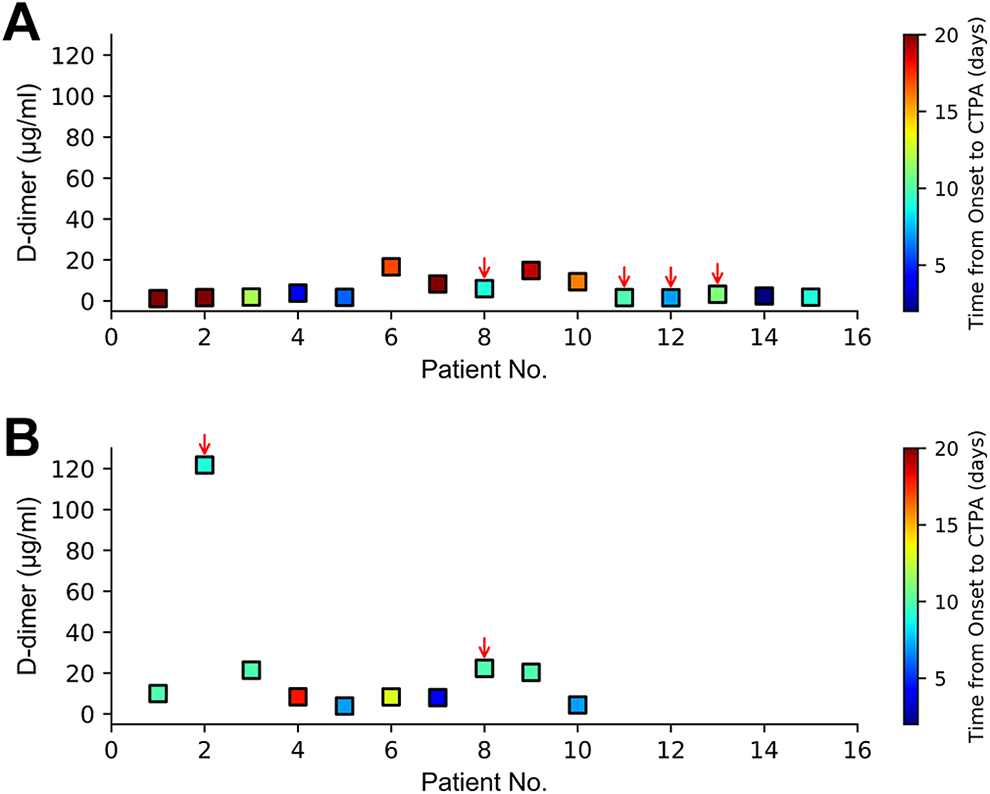
Serum (D-dimer) levels in 25 patients with COVID-19 pneumonia. (A) D-dimer values for patients without acute pulmonary embolism (APE; n = 15) tested over multiple days. (B) D-dimer values for patients with APE (n = 10) tested over multiple days. Color-coded squares correspond to D-dimer values for different dates. Red arrows indicate patients deceased during treatment.
Twenty patients were treated with anticoagulant therapy (low-molecular weight heparin, 0.6 mg/kg per 12 hours) regardless of the findings of APE in CTPA. These patients underwent a follow-up D-dimer test afterward. The D-dimer levels decreased in all patients.
Imaging Characteristics of COVID-19 Patients With APE
According to the chest CT image staging criteria of COVID-19, 3 patients were in the progressive stage, 16 were in the peak stage, and 6 were in the absorption stage. Ten (40%) patients showed APE on CTPA imaging (1 progressive stage, 7 peak stage, and 2 absorption stage), while 15 (60%) patients presented without APE (2 progressive stage, 9 peak stage, and 4 absorption stage). Of note, DVT was detected by ultrasonography in one patient with negative APE findings on CTPA. In the 3 patients who underwent a follow-up CTPA after anticoagulant therapy, all APE lesions were smaller compared with the first CTPA examination, and the corresponding D-dimer levels also decreased. In all these patients, filling defects on CTPA images occurred in the small branches of each lobar or segmental artery, but not in pulmonary trunk. Among 10 patients with APE, 6 (60%) patients had bilateral PE and 4 had unilateral PE. The thrombus-prone sites were the right lower lobe (70%), the left upper lobe (60%), both upper lobe (40%) and the right middle lobe (20%). The relevant characteristics of the 10 patients with APE are presented in Table 3. Figures 2 and 3 show typical APE images in patients with COVID-19.
Characteristics of COVID-19 Patients With APE.
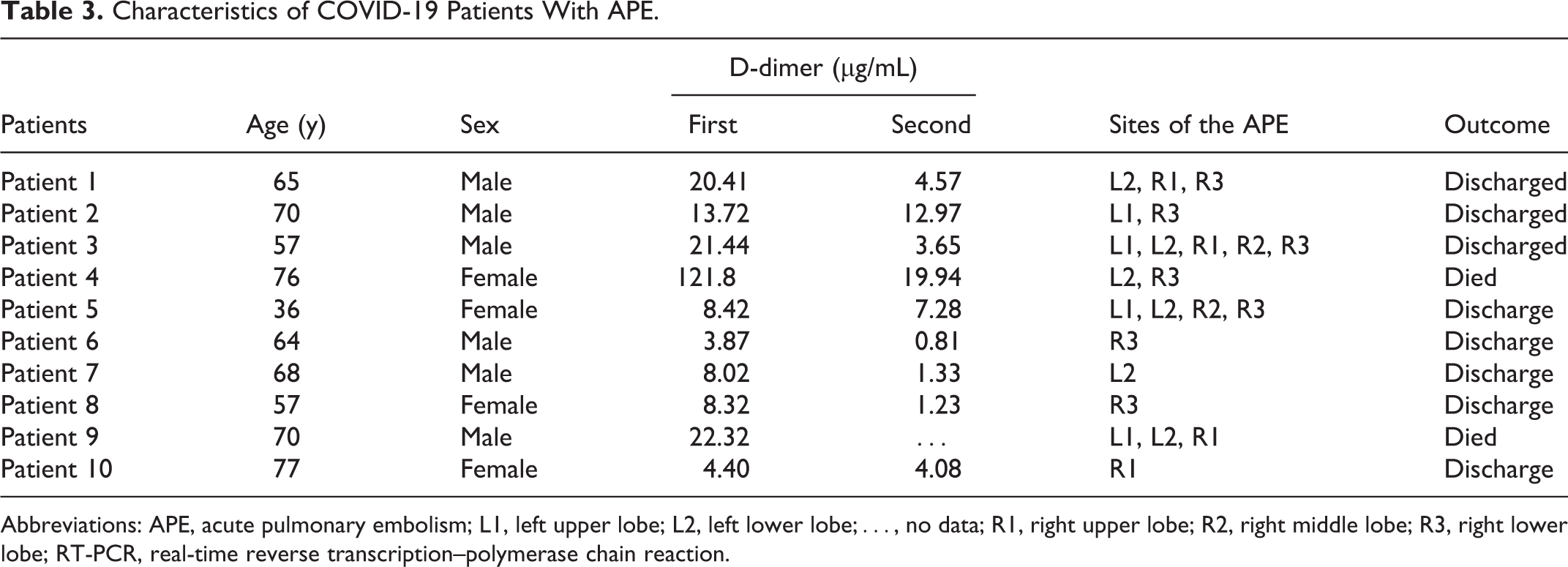
Abbreviations: APE, acute pulmonary embolism; L1, left upper lobe; L2, left lower lobe;…, no data; R1, right upper lobe; R2, right middle lobe; R3, right lower lobe; RT-PCR, real-time reverse transcription–polymerase chain reaction.

A 76-year-old women with severe COVID-2019 pneumonia. (A) Thrombus (arrow) occurred in bilateral lower lobe pulmonary artery on axial computed tomography pulmonary artery (CTPA) image. (B) Axial computed tomography (CT) image showed widely increased density of both lungs, showing a “white lung” appearance, indicating the patient was at the peak stage.

A 57-year-old man with moderate COVID-19 pneumonia. (A, B) The first computed tomography pulmonary artery (CTPA) examination: thrombus (thick arrow) in left upper lobe pulmonary artery and right lower lobe pulmonary artery. (C, D) Follow-up CTPA examination: corresponding acute pulmonary embolism (APE) lesions (thin arrow) at the same location were absorbed after anticoagulant therapy. (E) The first CTPA images at lung window: axial computed tomography (CT) image showed a little fibrous stripe (arrow), indicating the patient was at absorption stage.
Discussion
Similar to SARS-CoV-2, 2 other human epidemic coronaviruses, SARS and MERS, also cause severe lung damage and ARDS. 1,12 It is estimated that more than 10 000 patients have been infected by MERS and SARS in the past 2 decades, with mortality rates of 37% for MERS-CoV and 10% for SARS-CoV. 23,24 Global efforts were made to diagnose and treat these diseases. However, there are no published reports on APE in patients with MERS pneumonia, and only one case report described PE in patients with SARS. 13 In this study, we report the finding of APE in patients with COVID-19 pneumonia. Therefore, we should be alert to the APE events, which can be fatal, in patients with COVID-19 associated pneumonia.
In our study, of the 25 patients, 4 had chest pain, 4 had hemoptysis, and 20 had dyspnea even if under oxygen therapy. However, none of these symptoms is specific to APE, but may also result from coronary artery disease, aortic dissection, pneumothorax, or severe pneumonia. 25,26 Therefore, when patients with COVID-19 pneumonia have these symptoms, in association with elevated D-dimer levels, the risk of developing APE should be considered.
All patients with suspected APE in our study had an elevated D-dimer level with a median value of 6.06 μg/mL (IQR, 1.90-14.31). In fact, the finding of an elevated D-dimer level in patients with COVID-19 associated pneumonia was already reported several times. 1,3,14,27 These studies showed that patients with severe COVID-19 associated pneumonia usually have a significantly higher D-dimer level compared to nonsevere patients, and a markedly elevated D-dimer is common in deaths due to COVID-19 associated pneumonia. Some researchers assume that elevated D-dimer levels in COVID-19 patients result from an excessive consumption of coagulation factors due to activation and acceleration of the coagulation system, which might lead to disseminated intravascular coagulation (DIC). 28,29
It is known that elevated D-dimer levels are not only associated with APE but also with a series of other conditions such as DVT, cancer, peripheral vascular disease, pregnancy, and inflammatory disease.
6
Therefore, CTPA examinations and lower limb deep vein ultrasonography are important in the diagnosis of APE and DVT in COVID-19 patients with elevated D-dimer levels. Recently, some case reports and series
15
–19
described the presence of APE in patients with COVID-19. We also confirmed that COVID-19 patients had a risk of developing APE. In our study, APE lesions were detected by CTPA in 10 of the 25 COVID-19 patients, and these patients had a significantly higher D-dimer level compared to non-APE patients. Unfortunately, we could not assess the presence of DVT since most patients did not undergo lower limb deep vein ultrasonography. In recently published studies,
30
–32
DVT events were frequently reported, indicating that lower limb deep vein ultrasonography is necessary to detect DVT in COVID-19 patients. No significant differences were found in blood gas test results (PaC
In our study, APE lesions only occurred in the small branches of each lobar artery. Six (60%) patients presented with a thrombus in bilateral pulmonary artery branches, and 4 (40%) in unilateral pulmonary artery branches, indicating that the thrombus might derive from other sites, such as deep vein of the lower extremity. 13,33 One patient in our study underwent ultrasonography of the deep vein of the lower extremity, and a thrombus was found. In addition, 3 patients in our study underwent a follow-up CTPA examination after anticoagulant therapy. As the D-dimer levels decreased, the size of the emboli decreased compared with the first CTPA examination, suggesting an important role of CTPA in monitoring the changes of APE during and after anticoagulant therapy.
The mechanism of APE development in COVID-19 patients is unclear. There are no published relevant animal studies. Only a few previous reports described APE in patients with SARS. Autopsy results of multiple series of patients with SARS showed that vascular thromboses were common in lung specimens, suggesting the underlying thrombophilia in the lungs. However, another autopsy study of 8 patients with SARS showed that PE was found in the pulmonary arteries in 4 patients, 3 of whom had DVT, suggesting that the pulmonary artery thrombus derived from the deep vein of the lower limb. 13 Due to the COVID-19 quarantine requirements, reduced physical movement may result in higher risk of limb DVT. A previous study 34 also demonstrated that epithelial damage and platelets and endothelial cells dysfunction may contribute to thrombosis-associated influenza associated viral pneumonia. Additionally, DIC caused by an excessive consumption of coagulation factors in response to severe infection might be one of the causes of APE. 27,35 However, there are no autopsy studies in COVID-19 fatalities yet, and hence the pathogenesis of APE in these patients remains unclear.
This study has several limitations: First, the sample size of this study is relatively small. Based only on the data provided in our study, we cannot conclude what the incidence of APE is, and what potentially fatal factors for APE are present in patients with COVID-19 associated pneumonia. However, the 10 cases of APE in the 25 patients examined suggest a high incidence. Therefore, clinicians should be alert for the development of APE in the course of COVID-19 treatment. Second, this study is retrospective, and therefore prone to bias. Prospective studies are required to investigate the true incidence and fatality rate of APE in patients with COVID-19 associated pneumonia. Third, ultrasonographic screening for lower extremity DVT was not performed in our patients. Therefore, we could not determine whether inflammation or secondary lower extremity DVT was the primary cause of APE.
Conclusion
In conclusion, the results of the present study suggest that patients with COVID-19 associated pneumonia have a risk of developing APE during the disease. When D-dimer levels are elevated in the patients with COVID-19 associated pneumonia, CTPA should be performed to diagnose APE and assess its severity.
Footnotes
Authors’ Note
J.C. and X.W. contributed equally to the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.