
Abstract
Current evidence suggests that for outpatients with suspected pulmonary embolism (PE), multislice computed tomographic angiography (CTPA) is sufficient to rule out PE. However, the accuracy of CTPA alone has not been established for hospitalized patients. Our goal was to determine the prevalence of deep vein thrombosis (DVT) in hospitalized patients who had PE ruled out by CTPA. We conducted a prospective cohort study of patients who developed symptoms indicative of PE, after being admitted to the hospital for any reason other than PE and were evaluated with multislice CTPA. The main outcome was proximal DVT. Between November 2011 and December 2014, 191 hospitalized patients were screened. A total of 99 patients satisfied our inclusion criteria. The average length of hospitalization for this group was 14 days (range: 2-127 days). While hospitalized, 54 (28%) patients underwent a major surgical procedure and 80 (79%) were receiving thromboprophylaxis. Of the 99 patients included, 7 (7.07%; 95% confidence intervals [CIs]: 3.4-13.8) were diagnosed with a proximal DVT. The likelihood of developing a proximal DVT was higher for those with subtle and nonspontaneously reported symptoms of DVT, odds ratio [OR] was 50.93 (95% CI: 5.35-2572) and for those classified as PE likely OR was 37.54 (95% CI: 4.05-186.1). Given the prevalence of DVT in hospitalized patients with suspected PE ruled out by a negative multislice CTPA, our study suggests that compression ultrasonography would, in fact, be justified for patients with these characteristics.
Keywords
Introduction
The utility of compression ultrasonography (CUS) in ruling out proximal deep vein thrombosis (DVT) associated with suspected pulmonary embolism (PE) remains a matter of debate. 1 Current evidence shows that for outpatients presenting to emergency departments, suspected PE can be safely ruled out by multislice computed tomographic angiography (CTPA) with no need for leg CUS. 2 –4 However, to date there is a paucity of evidence to show if the same holds true for hospitalized patients with suspected PE 2,5 and that a normal multidetector CTPA result alone, may not safely exclude PE in patients with a high clinical pretest probability. 6 Based on the limited amount of available data, we estimated the prevalence of DVT in hospitalized patients with suspected PE ruled out by multislice CTPA to be approximately 6% (95% confidence intervals [95% CI]: 1.6-16.1). This estimate suggests that CUS is needed to rule out DVT in hospitalized patients with suspected PE. 7 The purpose of this study was to provide a more accurate estimate of the rate of proximal DVT in hospitalized patients with suspected PE ruled out with multislice CTPA.
Methods
Ethics
The study was approved by the ethics board of Hospital Italiano de Buenos Aires. The ethics board of Hospital Italiano de Buenos Aires approved the use of verbal consent to enroll patients in the study. Current legislation accepts verbal consent for observational studies. Verbal consent was obtained for all participants and recorded on a standardized form by the research coordinator. Medical records missing documentation of verbal consent were not reviewed. All records and information were rendered anonymous prior to analyzes.
Design
We conducted a prospective cohort study approved by the ethics board of the Hospital Italiano de Buenos Aires. Hospital Italiano de Buenos Aires is an academic hospital with 650 beds. In a prior analysis of 48 patients with suspected PE ruled out by multislice CTPA, 3 had a proximal DVT confirmed by CUS (6.25%; 95% CI: 1.6-16.1). We calculated that an additional 52 patients were needed to determine if the rate of proximal DVT in hospitalized patients with suspected PE was lower than 2.5% when PE was ruled out by multislice CTPA (assuming that the real prevalence of DVT was >6.5%). We selected 2.5% as the lower bound of the CI as it is a commonly accepted measure for studies evaluating diagnostic strategies for venous thromboembolism (VTE). 1 –4
Study Population and Intervention
Patients were eligible to participate in the study if (1) they were able to provide consent, (2) they presented with symptoms suggestive of PE (defined as acute onset of new or worsening shortness of breath, chest pain, hemoptysis, presyncope, or syncope), (3) symptoms developed >48 hours after admission in medically ill patients or >24 hours after admission following a major surgical procedure (defined as an anesthesia time >90 minutes), and (4) PE was ruled out after multislice CTPA. All scans were done with a 64-multislice CT scanner (Aquilion; Toshiba, Japan). Patients were excluded if they had symptoms compatible with PE prior to admission, had symptoms of DVT without symptoms of PE, refused to provide informed consent, refused bilateral leg CUS, or had a prior history of VTE. Within 24 hours of providing verbal consent, all patients received a bilateral whole-leg CUS.
Outcomes
The main outcome was proximal DVT (defined as noncompressible segment above the trifurcation of the popliteal vein). The secondary outcome included the prevalence of proximal DVT in patients with symptoms of DVT or in those classified as high probability for PE (ie, those with a Wells score greater than 4 points). Pulmonary embolism was considered ruled out when the multislice CTPA showed no filling defects in a segmental or larger pulmonary artery (single subsegmental embolus was considered as a PE only if the CUS was positive for a proximal DVT). Patients diagnosed with PE based on CTPA were excluded from the study.
Analysis and Statistics
Proportions, 95% CI, χ2 test with Yates correction, Mid-P exact test, and Student t tests were used. Odds ratios and their respective 95% CI were calculated. All analyzes were performed using Stats Direct.
Results
Between November 2011 and December 2014, 191 hospitalized patients were screened. Excluded from the study were 66 patients with confirmed PE, 14 patients with a history of prior VTE, and 12 who did not complete the assigned CUS. A total of 99 patients satisfied our inclusion criteria and were enrolled.
The cohort consisted of 38 males and 61 females. The number of those with cancer was 41. The mean age was 65.5 (standard deviation 18). The average length of hospitalization was 14 days (range: 2-127 days). During their admission, 54 patients had a major surgery and 80 were receiving thromboprophylaxis (70 were on low-molecular-weight heparin, 7 unfractionated, 2 on vitamin K antagonists, and 1 on mechanical thromboprophylaxis). The initial symptoms triggering the investigation for PE were dyspnea in 77.7%, followed by pleuritic chest pain in 15.2%. The mean duration of immobilization (more than 90% of the time in bed) was 12.1 days (range: 0-90). Fourteen (14.3%) patients presented subtle symptoms suggestive of DVT, which were not reported spontaneously, but to the directed and exhaustive questioning. The average Wells score in patients without symptoms of DVT was 2.6 versus 5.1 in those with DVT symptoms (P value <.001). Baseline characteristics are presented in Table 1.
Baseline Characteristics of the Study Population.
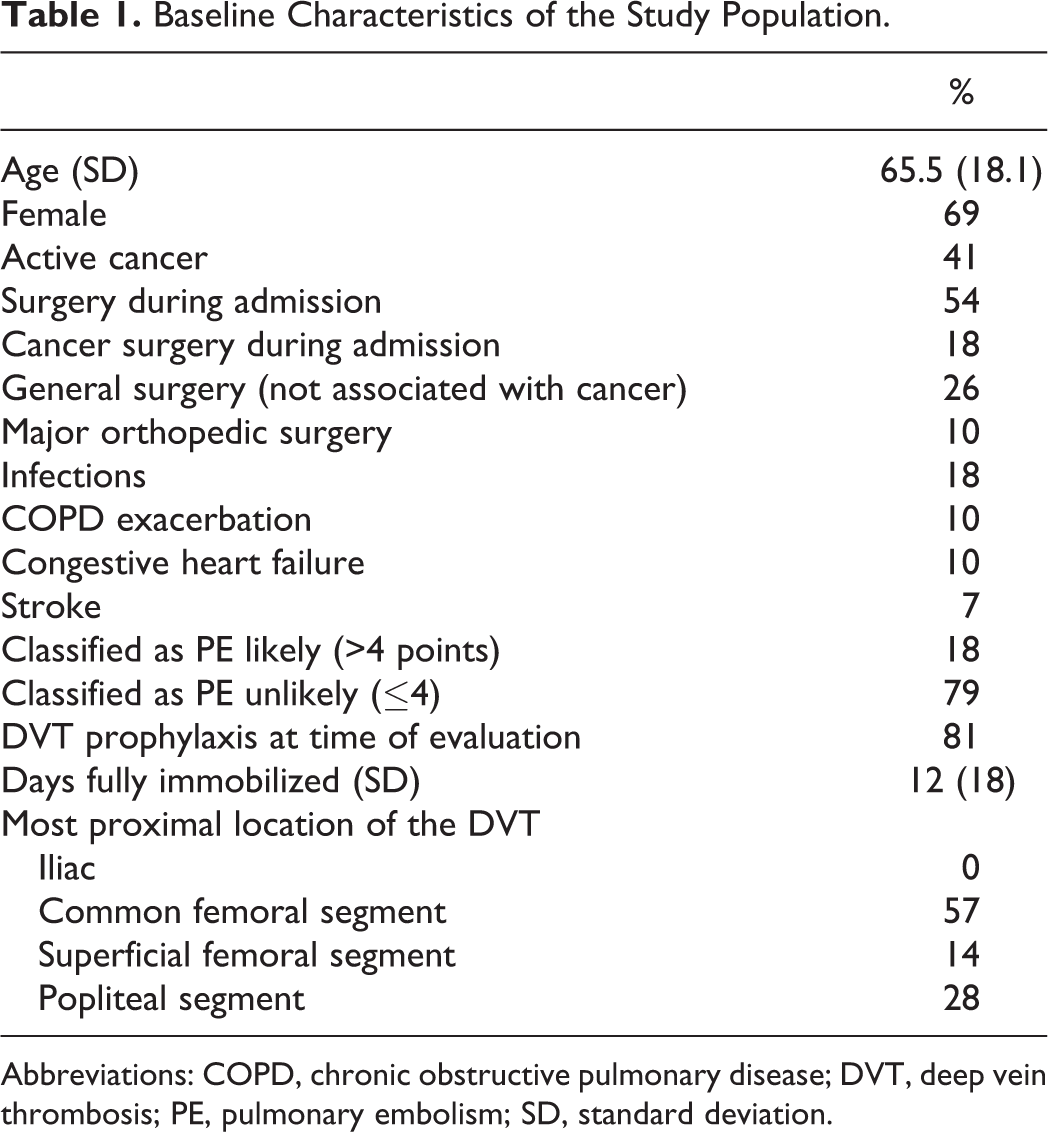
Abbreviations: COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; PE, pulmonary embolism; SD, standard deviation.
Of the 99 patients included, 7 (7.1%; 95% CI: 3.4-13.8) were diagnosed with a proximal DVT. Of these, 1 had an extensive DVT extending from the common femoral segment to the popliteal vein and 2 had an isolated popliteal DVT.
The prevalence of proximal DVT in patients without signs or symptoms of DVT was 1/84 (1.2%; 95% CI: 0.0-6.9). In contrast, the prevalence of DVT in patients with subtle symptoms was 6/14 (42.86%; 95% CI: 21.3-67.4) and OR was 50.93 (5.3-2572). The incidence of proximal DVT in patients classified as PE likely was 6/18 (33.3%; 95% CI: 15.7-56.9), whereas, in those classified as PE unlikely, the incidence was 1/79 (1.3%; 95% CI: 0.06-6.2) and OR was 37.54 (95% CI: 4.1-186.1). No other variables were associated with the presence of DVT (see Table 2).
Variables Associated With the Diagnosis of DVT.
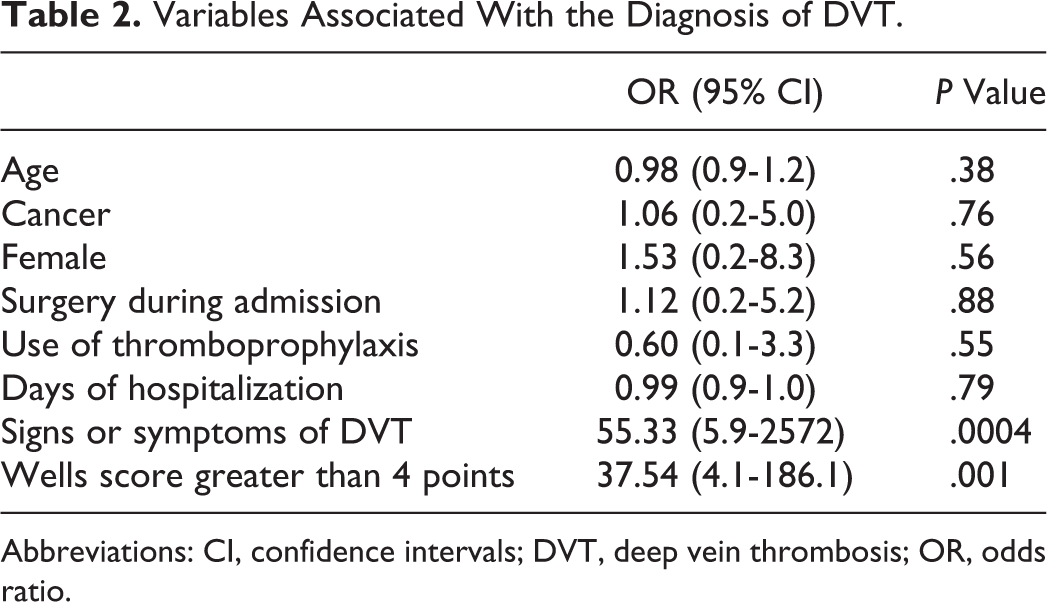
Abbreviations: CI, confidence intervals; DVT, deep vein thrombosis; OR, odds ratio.
Discussion
Our study suggests that in contrast to the outpatient population, the prevalence of proximal DVT in hospitalized patients with suspected PE ruled out by negative multislice CTPA is high. Therefore, bilateral leg CUS seems appropriate for this population (especially for patients with subtle or not spontaneously reported symptoms of DVT or patients classified as having a high clinical probability of PE using the Wells score). Our study was based on the assumption that patients with suspected PE ruled out by multislice CTPA do not require a bilateral leg CUS even if symptoms of DVT are present. To date, there are 4 large studies (3 prospective cohort studies and 1 randomized controlled study) supporting this approach for outpatients. Righini et al compared a strategy using
Unlike prior studies, our study looks specifically at hospitalized patients. Omitting bilateral leg CUS in patients with PE ruled out by CTPA has not been adequately validated in patients who develop symptoms of PE during hospitalization. The high incidence of DVT in our cohort could be explained by the high number of patients who had cancer or recent surgery. The incidence of cancer or recent surgery for patients in our study was double that of prior studies.
2
–4,8
–14
Van der Hulle et al
14
recently reported outcomes for hospitalized patients from 2 prospective cohorts who had suspected PE ruled out by clinical prediction rules,
Geographical variation is another possible explanation for the high rate of DVT in our cohort. Current information regarding the efficacy and safety of diagnostic strategies for suspected PE in developing countries is limited. 17 As previously suggested by Penaloza et al, current diagnostic approaches used to rule out PE have been validated in North America and therefore, may not apply in other regions around the world (eg, European countries) where the prevalence and severity of the disease are higher. 18 Our study highlights the need for adequate validation of clinical prediction rules across different settings (both global and local) to account for variation in the patient population.
Our findings have limitations. First, as this was a single-center study, there exists a potential for practice bias regarding diagnostic approach. Second, the interpretation of CUS reports lacked rigorous blinding. Nevertheless, all reports were read by radiologists specializing in CUS. Third, patients classified as PE unlikely did not receive a
In conclusion, given the high prevalence of DVT in hospitalized patients for whom PE is ruled out by a negative multislice CTPA (especially in those with symptoms of DVT or a high clinical probability of PE), a proximal bilateral leg CUS could be required to safely exclude DVT. This study does not prove the clinical importance of DVT found and that is why we strongly believe that this should be carefully assessed with a randomized controlled trail.
Footnotes
Authors’ Note
The results of this study were presented at the XXV Congress of the International Society of Thrombosis and Haemostasis in Toronto, Canada, 2015.
Acknowledgments
The authors would like to thank Maria Laura Martin and Alejandra Romero, who collaborated in collecting the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.