
Abstract
Background:
Catheter-directed thrombolysis (CDT) is seldom used for chronic femoropopliteal occlusive disease.
Methods:
Patients with chronic femoropopliteal occlusive disease enrolled between January, 2011 and April, 2017. Hospitalization expense, limb salvage rate and survival rate were calculated.
Results:
Twenty-nine patients were treated with CDT (CDT group) and 31 patients without CDT (Non-CDT group).The mean hospitalization expense (5.2 ± 0.5), balloon catheter (1.0 ± 0.2) and stents number (0.8 ± 0.2) in CDT group were significantly less compared to Non-CDT group (P < 0.05). The short-term and long-term effect scales showed similar in both groups. The incidences of perioperative complications (10.3% vs. 19.4%), primary patency and second patency rate, limb salvage rate (14.8% vs. 16.1%) and survival rate were also similar (P > 0.05). Six patients died in each group and only 2 disease related deaths were found in Non-CDT group.
Conclusion:
CDT is a safe and economic strategy for patients with chronic femoropopliteal occlusive disease, and should be served as blanket treatment for every patient without thrombolytic contradictions or a remedy for failure PTA to achieve a comparable clinical effect.
Keywords
Introduction
Patients with chronic peripheral artery occlusions often suffer from critical limb ischemia or disabling claudication. 1 Percutaneous recanalization is still technically and clinically challenging, which is hampered by arterial perforation, with a high restenosis rate and reduced primary success rate. 2 Moreover, conventional surgery is often not feasible due to the poor condition of distal arteries or co-morbidities. 3,4 Dotter et al 5 initially reported the satisfactory results achieved by catheter-directed thrombolysis (CDT), with a significant low dosage. The chronic occlusions lesions may arise de novo or as a complication of percutaneous transluminal angioplasty (PTA), or reconstructive surgery. Early studies indicated that CDT was safe, with a better limb salvage and mortality rate compared to surgery for acute lower limb ischemia. Unfortunately, the use of CDT in the treatment of chronic limb ischemia is not widely accepted, although clinical outcomes of CDT for chronic obstructions appeared to be encouraging in early studies of 80 s to 90 s in 19th century. It’s reported that femoropopliteal occlusions can be canalized again by CDT with a high success rate and better prognosis, 6,7 especially in longer occlusions, 8 as well as occluded occlusion of artery grafts. 9,10 Chronic occlusions imply fibrosis as the pathophysiology and fibrosis is not lysable. Nowadays, CDT was seldom used for chronic femoropopliteal occlusive disease in literatures, except for acute ischemia. 11 –14 This study aims to determine the safety and effectiveness of CDT for patients with chronic femoropopliteal occlusive disease during a 6-year period.
Materials and Methods
Patient Selection and Study Population
This retrospective, non-randomized, single-center study was approved by the local institutional review board. Informed consent was obtained from all enrolled patients. The femoropopliteal occlusion was diagnosed by computed tomographic angiography (CTA) and confirmed by digital subtraction angiography (DSA) before procedure (Figure 1). The selection criteria in this study are chronic symptoms of femoropopliteal occlusion (symptoms more than 3 month. 11,12 ) with grades of B to D according to the 2007 TransAtlantic Inter-Society Consensus (TASC II) classification. 15 Patients with chronic femoropopliteal occlusive disease were diagnosed and enrolled between January, 2011 and April, 2017. CDT was performed according to patients’ choice and economic condition. Conservative CDT was performed for patients refused PTA due to critical illness and poor prognosis (n = 5) or heavy economic burden (n = 4). CDT was used as a remedy for failure PTA in 5 patients to improve outcome. The postprocedure prevention of thrombosis was performed in 15 patients. Patients with absolute contraindications to thrombolysis were assigned to Non-CDT group, such as intracranial tumors, stroke, gastrointestinal hemorrhage in the last 3 months. A patient with severe renal insufficiency or allergic to contrast agents was excluded.

CTA examination before interventional procedure. (A) A long occlusive segment was found in the left external iliac artery, the common femoral artery, and the proximal end of the superficial femoral artery. (B) Low or equal density thrombus was found in the occlusive segment.
Interventional Procedure
Informed written consent was obtained from all patients before procedure. The access was obtained via the ipsilateral or contra lateral common femoral artery under local anesthesia.
After initial angiographic imaging, a 0.035" hydrophilic guide wire (Terumo) was used to cross the occlusive segment. After exchange of hard stiff guide wire, the thrombolytic catheter was implanted in the occlusive segment in CDT group, balloon angioplasty or adjunctive stenting was performed in Non-CDT group. CDT was performed with urokinase for 1-14 days. Balloon dilation was performed to cease the remained stenosis after CDT. Stent implantation would not perform if satisfactory patency achieved after balloon dilation (Figure 2).

CDT and balloon dilation. (A) The thrombolytic catheter was implanted in the occlusive segment in the left external iliac artery and the common femoral artery. (B) Repatency was shown in the occlusive segment after CDT for 9 days. (C) Balloon dilation was performed to cease the stenosis. (D) Satisfactory patency was found after balloon dilation without stent implantation.
Post Procedural Treatment and Follow-Up
All patients received 3000-6000 IU of low molecular weight heparin intra-arterially as per body weight during the intervention, and intravenous heparin was administered at 3500 IU subcutaneously every 12 hours for 2 days after procedure. After discharge, a lifetime regimen of oral aspirin (150 mg/day) and 3-month course of clopidogrel (75 mg/day) were initiated. Scale for clinical status was valued according to standard of Rutherford. 16 CTA or ultrasonography was used to verify the patency. The limb salvage rate and survival rate were calculated and causes of disease were recorded.
Statistical Analysis
All data were expressed as means ± SEM. Student t test and Fisher exact test were used for statistical analysis. Mann Whitney test was used for non-parametric statistics (Prism 5.0, GraphPad Software, Inc., SanDiego, CA). Differences were considered statistically significant at P < 0.05.
Results
Patient Demographics and Comorbidities
A total of 65 patients were screened between January, 2011 and April, 2017. Five patients were excluded due to severe renal insufficiency (n = 1), allergic to contrast agents (n = 1), and refuse to interventional treatment (n = 1). Twenty-nine patients were treated with CDT (CDT group) and 31 patients without CDT (Non-CDT group). Patient demographics were similar between Groups, and differences between 2 groups did not approached statistical significance. In Non-CDT group, 20 patients showed symptom aggravation, with a median aggravation duration of 30 days (16.3-52.5). In CDT group, 22 patients showed symptom aggravation, with a median aggravation duration of 14 days (9.8-30.0). There was no significant difference in aggravation duration (P = 0.11). Lesions were classified as Trans Atlantic Inter-Society Consensus (TASC II); C and D grades were most common in both groups (Table 1).
Patient Demographic Data.

Hospitalization and Procedure
The mean hospitalization expense was (5.2 ± 0.5) ×104 RMB in CDT group, which was significantly lower than (7.4 ± 0.8) ×104 RMB Yuan in Non-CDT group (P = 0.02). Both balloon catheter and stents were significantly less used in CDT group compared to Non-CDT group (P < 0.05). In CDT group, 18 patients underwent balloon dilation, with a mean number of balloon catheters of 1.0 ± 0.2, and 14 patients underwent stent implantation (0.8 ± 0.2/patient). However, only 1 patient did not undergo balloon dilation and 7 patients did not undergo stenting in Non-CDT group. The mean days of hospitalization between 2 groups did not showed significant difference (P = 0.70). Besides, the mean volume of urokinase was (204.1 ± 31.1) ×104 IU, and the mean duration of thrombolysis was 6.1 ± 0.7 days in CDT group (Table 2).
Hospitalization, Procedure, and Clinical Effect.

Indications for CDT and Its Clinical Effect
As shown in Table 3, short-term and long-term effect scales showed similar in both groups. According to the indications for CDT, patients with postprocedure prevention showed a good clinical outcome, however, patients with conservative CDT and remedy for failure PTA showed a worse clinical status of “Minimal to moderately improved” than Non-CDT group (P < 0.05).
Indications for CDT and Its Clinical Outcome.a
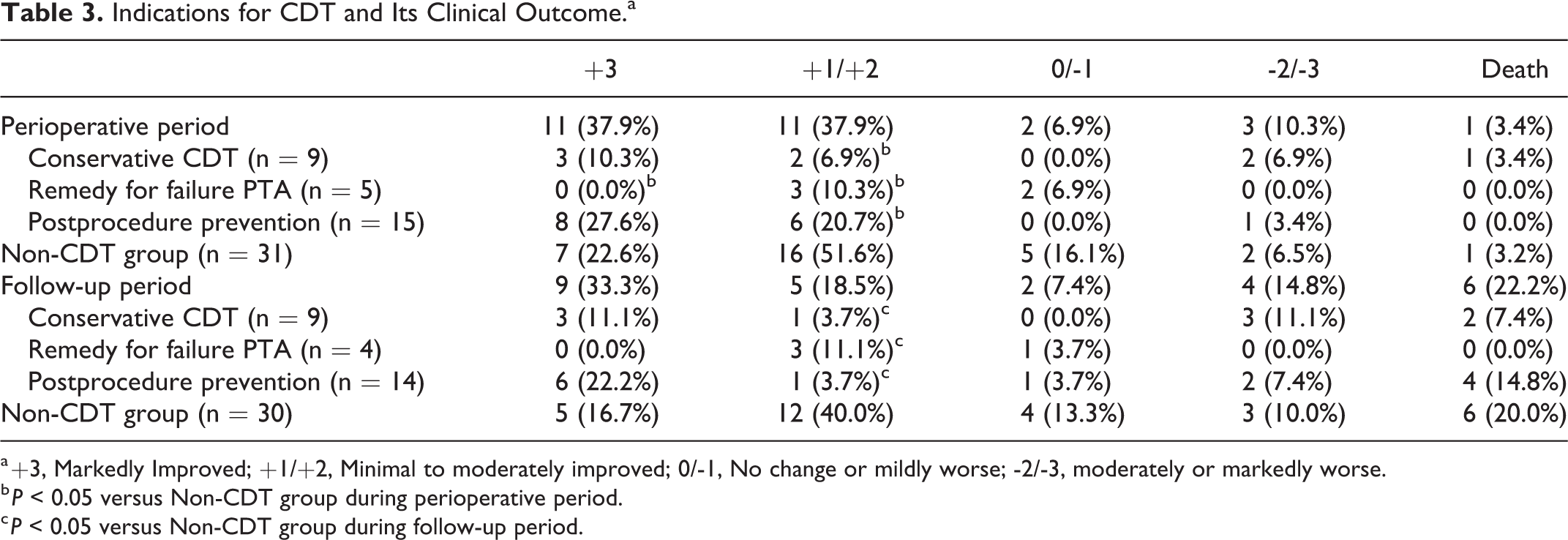
a +3, Markedly Improved; +1/+2, Minimal to moderately improved; 0/-1, No change or mildly worse; -2/-3, moderately or markedly worse.
b P < 0.05 versus Non-CDT group during perioperative period.
c P < 0.05 versus Non-CDT group during follow-up period.
Perioperative Complications
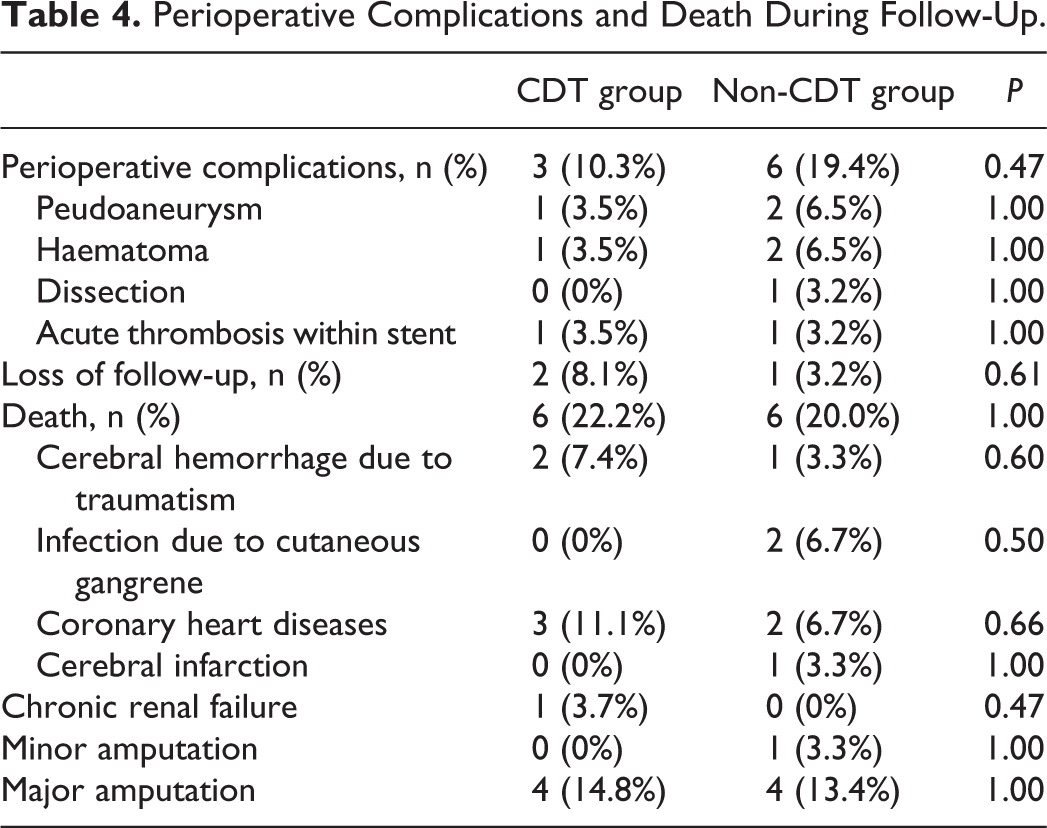
Perioperative complications were found in 3 patients in CDT group, included 1 peudoaneurysm and 1 hematoma of the access arteries, and 1 acute thrombolysis within stent. Severe bleeding caused by CDT, such as cerebral hemorrhage, was not observed. Six complications were found in Non-CDT group, included 2 peudoaneurysms, 2 hematomas and 1 dissection of the access arteries, and 1 acute thrombolysis within stent. Incidences of perioperative complications did not showed significant difference between 2 groups (P = 0.47). All peudoaneurysms and hematoma were confirmed by ultrasonography, and then compressed by bandage for 1 to 3 days. Only 1 peudoaneurysm in Non-CDT group needed thrombin injection under guidance of ultrasonography. The dissection was shown after balloon dilation, which was successfully compressed after stent implantation (Table 4).
Perioperative Complications and Death During Follow-Up.
Long Term Follow-Up
The primary patency and second patency rate did now showed significant difference between 2 groups (P > 0.05). The primary patency rates and the second primary patency rates in CDT group were 51.4% and 74.0% at 1 year, 44.1% and 74.0% at 3 years, 44.1% and 59.2% at 6 years, respectively. The limb salvage rate and survival rate were also similar difference between 2 groups during follow-up (P > 0.05, Figure 3). There were 4 major amputations in CDT group, and 1 minor and 4 major amputation in Non-CDT group. During the 6 years of follow-up, 6 patients died in each group during follow-up. In CDT group, 2 died from cerebral hemorrhage due to traumatism, 3 died from coronary heart disease, and 1 died from chronic renal failure. In Non-CDT group, 1 died from cerebral hemorrhage due to traumatism, 2 died from coronary heart disease, and 1 died from cerebral infarction. All above patients died due to non-procedure-related causes. Only 2 disease related deaths were found in Non-CDT group, who might die from infection induced by cutaneous gangrene in lower extremity (Table 4).

Long-term follow-up results. The primary patency (P = 0.23) and second patency rates (P = 0.56) did not show significant difference. The limb salvage rate (P = 0.86) and survival rate (P = 0.86) also showed similar difference between 2 groups during follow-up.
Discussion
The arterial thrombotic conditions are often superimposed on an intrinsic vascular lesion, which can be corrected by PTA if pharmacological thrombolysis is possible. 7 Considering that the systemic administration of thrombolytic agents has not achieved encouraging effect, CDT of low dose streptokinase or urokinase has been used in chronic arteriosclerotic lesions. 7
Chronic occlusions imply fibrosis as the pathophysiology and fibrosis is not lysable. According to our knowledge, there is not completely fibrotic tissue in chronic occlusion; there are some non-fibrotic artery segments. The purpose of the CDT is to expose the potential non-fibrotic artery segment as much as possible, and the remaining fibrotic occluded vessels are treated with balloon dilatation or stent placement. Although there was no significant difference in aggravation duration and acute thrombotic event was not observed in all patients, most patients showed symptom aggravation may explain why CDT works.
Clinical outcomes of CDT for chronic obstructions appeared to be encouraging. It’s reported that several week 13 or month-old 6 femoropopliteal occlusions can be canalized again by CDT with a high success rate. PTA of femoropopliteal arteries seems to have a better prognosis if combined with CDT, especially in longer occlusions. 8 Lupattelli et al 6 reported that effective CDT with low-dose urokinase was accomplished in 85.7% patients with chronic arteriosclerotic obstructions, and 71.4% cases underwent balloon dilation for underlying stenosis to prevent thrombosis again. Besides, CDT was successful for recanalization of acute and chronically occluded occlusion of artery crossover graft and artery bypass graft. 9,10
The segmental femoral popliteal artery occlusion of TASC II C, D lesions were mostly found in the vascular bifurcation sites of short segment calcification secondary thrombosis. Arterial thrombolysis combined with PTA, can make some femoropopliteal artery occlusion of the TASC II C type D lesions into TASC II A, B lesions, and may improve the success rate of endovascular treatment. For TASC type C type D femoral popliteal artery lesions, Conrad et al 17 reported that the secondary patency rate and limb salvage rate can reach 89.7% and 94.2% respectively 3 years after surgery. This procedure was usually performed in patients with acute or sub acute arterial occlusion disease, with good distal outflow tract and signs of thrombosis shown in MRA or CTA examination.
In our study, the femoropopliteal TASC II C or D type of long segment occlusion often showed different degrees of improvement in patency if firstly treated by CDT, leading to the subsequent success of PTA possible. The thrombolytic agents should be directly injected with the catheter tip in the thrombus, to avoid outflow through the hypertrophic collateral arteries present at the origin and come into maximal contact with the surface of the clot. 7 If the thrombus is broken through mechanical thrombolysis during PTA, the thrombolytic agents and fresh plasminogen will have access to a larger surface of the thrombus. 6,7
Some study limitations need to be addressed. First, this single center study included only a small number of patients in CDT group, leading to an ineffective subgroup analysis according to different indications. Second, there was an obvious bias in patient selection since CDT was also performed as remedy for failure PTA and conservative treatment. This bias was unfavorable for the CDT group, since it included more difficult cases with critical illness and poor prognosis, which could account for comparable outcome in CDT group. Thus, this bias in patient selection does not weaken, but rather strengthens, the results of our study.
In summary, CDT is a safe and economic strategy for chronic femoropopliteal occlusive disease, and can serve as conservative treatment or remedy for failure PTA to achieve a comparable clinical effect.
Footnotes
Authors' Note
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Author Contributions
Yi MF and Guo JJ contributed equally to this work and share co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 81501569).