
Abstract
Background
This study aimed to evaluate the predictive value of the red cell distribution width/ albumin ratio (RDW/ALB ratio, RAR) for spontaneous recanalization (SR) in patients with acute ST-segment elevation myocardial infarction (STEMI).
Methods
We conducted a retrospective analysis of 353 patients diagnosed with STEMI who were admitted to our institution between January 2019 and April 2022. Based on the thrombolysis in myocardial infarction (TIMI) flow grades in the infarct-related artery (IRA), the patients were divided into two groups: a non-spontaneous recanalization (NSR) group (TIMI 0–1; n = 230) and an SR group (TIMI 2–3; n = 123). The RAR was calculated for each patient, and its association with SR was evaluated using binary logistic regression and receiver operating characteristic (ROC) curve analysis. Results are presented as odds ratios (OR) with 95% confidence intervals (CI).
Results
Patients in the NSR group had a significantly higher RAR level compared to the SR group (3.34 [3.11, 3.64] vs. 3.18 [2.95, 3.45], P < 0.001). In the multivariable logistic regression analysis adjusted for key confounders including sex, age, white blood cell (WBC), apolipoprotein A1(ApoA1), albumin (ALB), and left ventricular ejection fraction (LVEF), a higher RAR remained an independent predictor for the absence of SR (OR = 2.528, 95% CI: 1.019-6.276). The predictive performance of RAR for SR was modest, with an area under the ROC curve of 0.613 (95% CI: 0.552-0.675), yielding a sensitivity of 53.9% and a specificity of 67.0%.
Conclusion
Our findings suggest that RAR is a promising biomarker for predicting SR in patients with acute STEMI. It helps us to identify high-risk populations in acute STEMI without SR at an early stage, thereby enhancing our ability for early intervention.
Keywords
Background
ST-segment elevation myocardial infarction (STEMI) is one of the most severe manifestations of coronary artery atherosclerosis, characterized by the rupture of atherosclerotic plaques leading to thrombosis, coronary occlusion, and subsequent ischemic myocardial necrosis. 1 Primary percutaneous coronary intervention (PPCI) is effective in reopening occluded or severely narrowed coronary arteries, thereby restoring blood flow to the ischemic myocardium in patients with acute STEMI. 2 Currently, some STEMI patients can achieve a thrombolysis in myocardial infarction (TIMI) grade of 2 to 3 prior to undergoing relevant treatments, indicating infarct-related artery spontaneous recanalization (IRA-SR). This suggests that they may not require thrombolytic or interventional treatments to open the IRA. 3 Research have indicated that SR is associated with reduced infarct size, preserved cardiac function, and lower rates of cardiac events. Patients with SR have significantly a better short-term prognosis compared to those with persistent IRA occlusion. 4 Therefore, identifying a reliable non-invasive peripheral biomarker to detect SR clinically remains an important and challenging objective.
Several lines of evidence have shown that the Red cell Distribution Width (RDW) not only serves as one of the indicators for the differential diagnosis of anemia but also reflects the body's inflammatory status, being closely related to the progression of both acute and chronic diseases, such as cardiovascular diseases, acute kidney injury and diabetes.5–7 Albumin (ALB), the primary protein synthesized by the liver, plays key roles in maintaining nutritional status and immune regulation, and serves as a clinical indicator of inflammatory activity. In patients with acute coronary syndrome (ACS), low albumin levels are significantly associated with a higher risk of in-hospital major adverse cardiac events (MACE). 8 Furthermore, its predictive value extends to chronic cardiovascular conditions and specific treatment populations. Studies have shown that for patients with dual-chamber permanent pacemakers, low serum albumin is an independent predictor of long-term mortality. 9 Similarly, among heart failure with reduced ejection fraction (HFrEF) patients implanted with an implantable cardioverter-defibrillator (ICD), the prognostic nutritional index (PNI), which incorporates albumin and lymphocyte count, has been proven to be a powerful predictor of long-term mortality, indicating that the albumin-related nutrition-inflammatory status profoundly affects the outcomes of these patients. 10 These findings collectively highlight the broad application prospect of albumin in cardiovascular risk assessment.
Recently, composite ratios derived from routine blood parameters have gained increasing attention as promising prognostic tools in various medical fields. The Red cell Distribution Width/Albumin Ratio (RAR), which integrates markers of chronic inflammation and nutritional status, is one such biomarker that has demonstrated significant predictive value across diverse patient populations beyond cardiovascular disease. For instance, elevated RAR has been consistently associated with increased mortality and poor clinical outcomes in patients with sepsis, chronic kidney disease and stroke. This broad applicability underscores the role of RAR as a robust indicator of systemic physiological derangement, reflecting both inflammatory stress and nutritional deficits.11–13 However, its application in predicting of IRA-SR in patients with STEMI has not been reported.
Methods
Study Population
This study is a retrospective analysis that selected 429 patients with acute STEMI who were hospitalized at the Chest Pain Center of Fujian Medical University Affiliated Mindong Hospital between January 2019 and April 2022. Among these, 353 patients met the inclusion criteria. The diagnosis of STEMI was established based on the “2023 ESC Guidelines for the Management of Acute Coronary Syndromes”. 14 All patients received standardized dual antiplatelet therapy and heparin anticoagulation prior to the procedure, and emergency coronary angiography (CAG) was performed within 12 hours of symptom onset. Based on the results of the CAG, the subjects were categorized into either the spontaneous recanalization (SR) group or the non-spontaneous recanalization (NSR) group. SR was defined as TIMI grade 2 or 3 flow in the infarct-related artery in STEMI patients who had not received thrombolytic therapy, whereas TIMI grade 0 or 1 was classified as NSR. Exclusion criteria included patients with Pre-CAG thrombolysis, coronary artery spasm, history of coronary artery bypass grafting or PCI, biliary and liver diseases, severe anemia or other hematologic disorders, tumors, severe infectious diseases and missing clinical data.
Clinical and Laboratory Data Collection
Baseline data were collected for all patients, including gender, age, smoking history, medical histories such as diabetes and hypertension. Upon admission (before emergency surgery), a complete blood count was immediately tested by Sysmex XN9000 hematology analyzer.
Fasting blood samples were collected from the elbow the following morning and analyzed with the Beckmann Coulter AU480 analyzer to measure triglycerides (TG), cholesterol (CH), low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), fasting blood glucose (FBG), and serum creatinine (Scr). Additionally, all subjects underwent cardiac color Doppler ultrasound within 12 hours of admission to assess abnormal ventricular segmental motion and record left ventricular ejection fraction (LVEF).
CAG
CAG was performed using Judkins catheters to visualize the left and right coronary arteries for the diagnosis of coronary artery disease (CAD). TIMI flow grades were assessed by two interventional cardiologists specializing in coronary interventions. The grades were defined as follows: TIMI 0 indicated no perfusion of the distal IRA; TIMI 1 indicated perfusion without complete filling; TIMI 2 indicated delayed filling or clearance; and TIMI 3 indicated complete and rapid filling and clearance. The Gensini score was calculated by assigning a severity weight to each coronary stenosis according to the degree of luminal narrowing and its topographic importance. 15
Statistical Analysis
Data analysis was conducted and graphs were created using SPSS 27.0 and GraphPad 10 software. Categorical variables are presented as percentages and compared using the chi-square test. Normally distributed metric data are expressed as mean ± standard deviation and compared with independent samples t-tests. Non-normally distributed metric data are presented as median (P25, P75) and compared using the Mann–Whitney U test. Spearman analysis was employed to examine the correlation between two sets of data. The study constructed a series of logistic regression models using a hierarchical approach: Model A: Unadjusted, to show the crude association. Model B: Adjusted for sex and age. These are fundamental demographic variables considered universal confounders in clinical epidemiological studies. Model C: Additionally adjusted for WBC, ApoA1, albumin (ALB), and LVEF. The selection of these covariates was based on the potential association in univariate analysis (P < 0.1). Receiver operating characteristic (ROC) curve analysis was utilized to test the predictive effect of the RAR on SR. A statistically significant difference was defined as a p-value <0.05.
Results
Baseline Characteristics and Angiographic Analysis
All subjects were divided into two groups (Table 1) according to TIMI grade, NSR group (TIMI 0-1, n = 230) versus SR group (TIMI 2-3, n = 123). The comparison of baseline clinical characteristics between two groups showed no statistically significant differences. NSR group had a signifcantly higher RAR than that in SR group [3.34(3.11, 3.64) vs. 3.18(2.95, 3.45); P < 0.001] (Table 1; Figure 1). Laboratory and echocardiographic findings further indicated elevated white blood cell (WBC) count and reduced levels of apolipoprotein A1 (ApoA1), albumin (ALB), and left ventricular ejection fraction (LVEF) in the NSR group. No significant differences were observed between the NSR and SR groups in plasma concentrations of hemoglobin (HGB), platelet (PLT), TG, CH, HDL, LDL, ApoB, FBG, Scr, and RDW.

The Distribution of RAR at NSR and SR Patients. RAR: Red Cell Distribution Width/Albumin Ratio. NSR: non-Spontaneous Recanalization. SR: Spontaneous Recanalization.
Baseline Characteristics of the Subjects in the Two Groups.

Abbreviations: NSR: non-spontaneous recanalization. SR: spontaneous recanalization. WBC: white blood cell. HGB: hemoglobin. PLT: platelet. TG: triglycerides. CH: cholesterol. HDL: high-density lipoprotein. LDL: lowdensity lipoprotein. ApoA1: apolipoprotein A1. ApoB: apolipoprotein B. FBG: fasting blood glucose. Scr: serum creatinine. RDW: red cell distribution width. ALB: albumin. RAR: red cell distribution width/albumin ratio. LVEF: left ventricular ejection fraction.
There were no significant differences in the location of the IRA and the number of diseased vessels between the two groups. However, regarding CAD severity, the NSR group showed higher Gensini scores than the SR group (Table 2).
Vascular Characteristics.

Abbreviations: NSR: non-spontaneous recanalization. SR: spontaneous recanalization. LAD = left anterior descending artery. LCX = left circumflex artery. RCA = right coronary artery.
Analysis of Correlation Between RAR and TIMI Grade, Gensini Score
Spearman's rank correlation analysis in patients with acute STEMI revealed a significant negative association between RAR and TIMI grade (r = –0.211, p < 0.001; Table 3 and Figure 2), further supporting the relationship between RAR and IRA-NSR. In addition, There was also a significant positively correlation between the RAR and the severity of CAD, as estimated by the Gensini score (r = 0.145, p = 0.006, Table 3; Figure 2).

Relationship Between RAR and TIMI Grade, Gensini Score. RAR: Red Cell Distribution width/albumin Ratio. TIMI: Thrombolysis in Myocardial Infarction.
Spearman Correlation Analysis Between RAR and TIMI Grade, Gensini Score.

Abbreviations: RAR: red cell distribution width/albumin ratio. TIMI: thrombolysis in myocardial infarction.
Multivariable Logistic Regression Analysis After Adjustment for Covariates.

Model A:adjusted for none covariates.
Model B:adjusted for sex and age.
Model C:adjusted for sex, age, WBC, ApoA1, ALB, LVEF.
Abbreviations: CI, confidence interval. OR, odds ratio. WBC: white blood cell. ApoA1: apolipoprotein A1. ALB: albumin. LVEF: left ventricular ejection fraction.
Binary Logistic Regression Analysis of NSR
Univariable logistic regression analysis identified white blood cell (WBC) count (OR = 1.065, 95% CI: 1.001–1.133) and RAR (OR = 2.262, 95% CI: 1.336–3.830) as risk factors for NSR. In contrast, apolipoprotein A1 (ApoA1) (OR = 0.304, 95% CI: 0.102–0.772), albumin (ALB) (OR = 0.942, 95% CI: 0.891–0.995), and left ventricular ejection fraction (LVEF) (OR = 0.970, 95% CI: 0.943–0.998) were identified as protective factors. After adjustment for confounding factors, RAR remained an independent predictor of NSR in the multivariate model (OR = 2.528, CI95%: 1.019-6.276) (Figure 3, Table 4).

The Univariable Logistic Regression Analysis of NSR. NSR: non-Spontaneous Recanalization. SR: Spontaneous Recanalization. WBC: White Blood Cell. HGB: Hemoglobin. PLT: Platelet. TG: Triglycerides. CH: Cholesterol. HDL: High-Density Lipoprotein. LDL: Lowdensity Lipoprotein. ApoA1: Apolipoprotein A1. ApoB: Apolipoprotein B. FBG: Fasting Blood Glucose. Scr: Serum Creatinine. RDW: Red Cell Distribution Width. ALB: Albumin. RAR: Red Cell Distribution Width/Albumin Ratio. LVEF: Left Ventricular Ejection Fraction. CI: Confidence Interval. OR: Odds Ratio.
ROC Curve Analysis to Assess the Predictive Efficacy of RAR
To assess the predictive efficacy of RAR in identifying NSR, ROC curves were constructed, employing NSR as the outcome variable and RAR, ALB and RDW as the test variables (Table 5, Figure 4). The result revealed that the area under the curve (AUC) for RAR was 0.613 (95% CI: 0.552–0.675). An RAR level greater than 3.201 was identified as an independent predictor for SR in STEMI patients, with predictive performance significantly superior to that of ALB and RDW (P = 0.038 and 0.011, respectively).

ROC Curves of RDW, ALB and RAR for predicting NSR. ROC: receiver operating characteristic. RDW: Red Cell Distribution Width. ALB: Albumin. RAR: Red Cell Distribution Width/Albumin Ratio. AUC: Areas Under the Curve. NSR: non- Spontaneous Recanalization.
Comparison of the Predictive Efficacy of RDW, ALB and RAR.
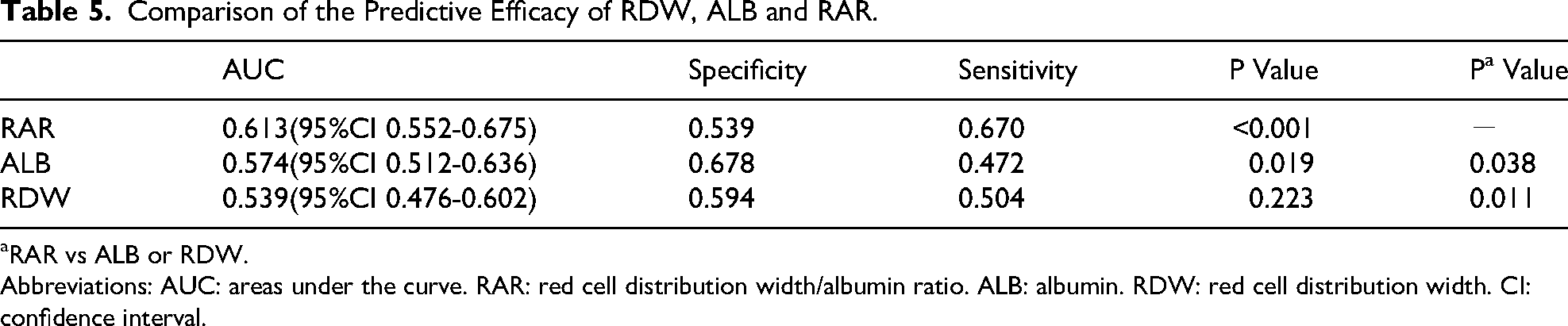
RAR vs ALB or RDW.
Abbreviations: AUC: areas under the curve. RAR: red cell distribution width/albumin ratio. ALB: albumin. RDW: red cell distribution width. CI: confidence interval.
To further test our hypothesis that combining RAR with WBC and ApoA1—both significant predictors from Table 1—would improve predictive accuracy, three index models were developed. Figure 5 and Table 6 demonstrate that Model 3, which integrates RAR with WBC and ApoA1, achieved a higher specificity of 0.817 and an increased AUC. However, the improvement in AUC was not statistically significant compared to RAR alone (P = 0.149).

ROC Curves of Combined Makers for Predicting NSR. ROC: Receiver Operating Characteristic. RAR: Red Cell Distribution Width/Albumin Ratio. NSR: non-Spontaneous Recanalization.
Comparison of the Predictive Efficacy of Combined Markers.
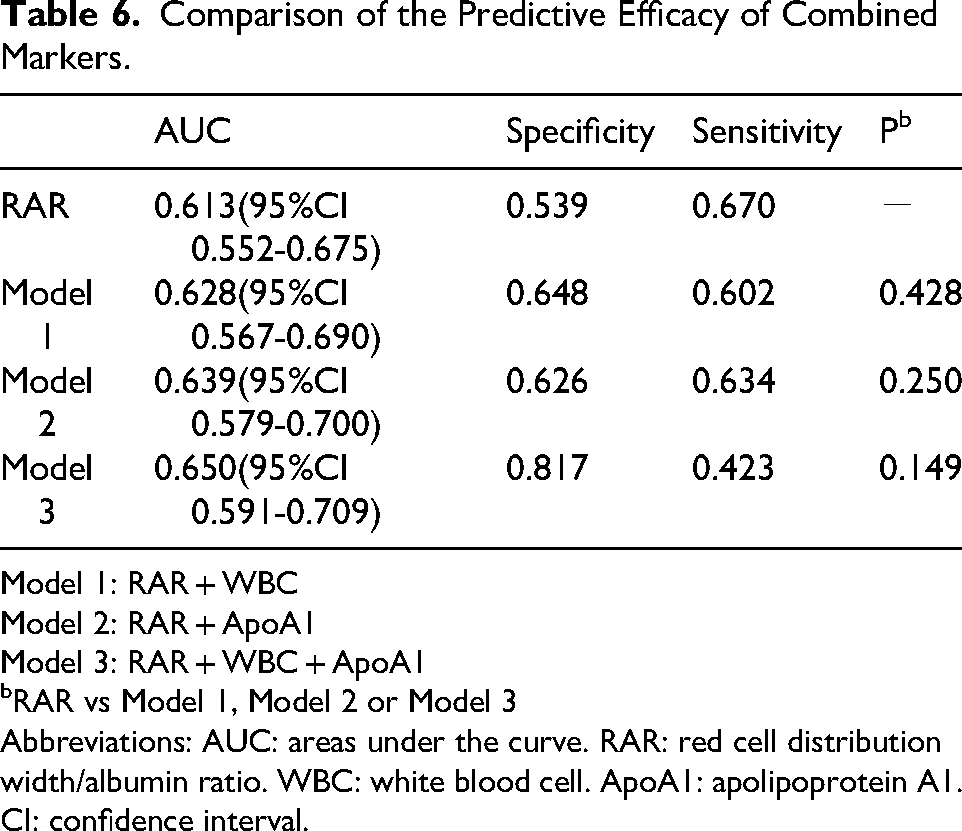
Model 1: RAR + WBC
Model 2: RAR + ApoA1
Model 3: RAR + WBC + ApoA1
RAR vs Model 1, Model 2 or Model 3
Abbreviations: AUC: areas under the curve. RAR: red cell distribution width/albumin ratio. WBC: white blood cell. ApoA1: apolipoprotein A1. CI: confidence interval.
Discussion
This study illustrated that the RAR is an independent predictor of NSR in the STAMI patients and is positively associated with severity of CAD. We confirmed that this composite indicator exhibits superior predictive power for NSR compared to ALB or RDW evidenced by comparative analysis of the area under ROC curves.
A recent global meta-analysis comprising 22 studies and 29,826,717 individuals reported that the prevalence of myocardial infarction (MI) was 3.8% in individuals younger than 60 years and 9.5% in those over 60. 16 Given the high mortality and disability rates associated with STEMI, timely and effective identification and treatment are crucial not only for saving lives but also for preserving long-term quality of life. In alignment with the latest expert consensus on cardiovascular interventions and therapeutics (CVIT), PPCI is the recommended reperfusion therapy for patients with STAMI over fibrinolysis when performed by an experienced team within 120 minutes from first medical contact (FMC). Importantly, better prognostic outcomes are observed when PPCI is performed in patients with IRA-SR. 17 Early IRA-SR and successful restoration of coronary flow are crucial for improving cardiac function following STEMI. Schaaf et al 18 found that contrast-enhanced cardiac magnetic resonance examination can reveal that STEMI patients with early IRA-SR had smaller infarct sizes, lower incidence of microvascular obstruction, better cardiac function, and more favorable prognoses. A study incorporating CAG data demonstrated that 30% of patients with acute STEMI had an early SR, which was mostly in line with our research findings. The research also showed that clinical factors such as gender, hypertension, diabetes, smoking, hyperlipemia were not associated with NSR. However, it found that patients with SR were were generally younger, had lower cardiac troponin I (CTnI) peak value, and higher thrombosis burden compared to those with NSR. 19 In our study, we find no significant differences between the two groups of patients not only in clinical characteristics, such as gender, age, smoking history, hypertension and diabetes, but also in several laboratory parameters including HGB, PLT, TG, CH, HDL, LDL, ApoB, FBG, Scr, and RDW.
Currently, while a considerable body of research exists on the influencing factors of IRA-SR in patients with acute STEMI, there remains a lack of specific reports addressing quantitative predictive indicators. Rahim Kanji. et al. demonstrated that in the setting of STEMI, SR was related to a more favorable global thrombotic profile, characterized by reduced platelet reactivity and more effective endogenous fibrinolysis, as measured by comparing occlusion times (OT) and lysis times (LT). 20 Not coincidentally, other scholars have also identified several independent predictors of SR in STEMI patients including endothelin-1, homocysteine, and apelin.21–23
Red blood cell distribution width (RDW), which reflects the variability in the size of circulating red blood cells, is a routine parameter in blood tests. Extensive research has established its strong association with cardiovascular diseases. RDW has predictive and prognostic value for different clinical types of atrial fibrillation (AF), including postoperative and recurrent AF, and shows potential for incorporation into risk scoring system. 24 High RDW values at both admission and discharge in hospitalized heart failure patients are linked to adverse outcomes, leading to its inclusion in recent heart failure (HF) prognostic models. Investigating RDW as a therapeutic target in HF may represent a promising research direction. 25
Despite the established sensitivity of RDW in predicting ACS and its correlation with adverse cardiovascular events and mid-term mortality in patients undergoing primary PCI,26–27 our study found that no significant difference in admission RDW values between patients with SR and those with NSR (P = 0.224). What's more, RDW failed to serve as a standalone predictor for NSR (AUC = 0.539, 95%CI 0.476-0.602, P = 0.223). Given the limited number of previous studies exploring the relationship between RDW and SR, the reasons for this discrepancy remain unclear. Potential explanations may include the exclusion of patients with anemia or other hematological disorders, as well as the relatively small sample size in our study.
Albumin(ALB), synthesized by the liver, is the most abundant and widely used protein in human blood. Known for its ligand-binding, transport, and antioxidant properties, it is extensively applied in assessing nutritional status and systemic responses. 28 ALB is classified as a negative acute-phase protein, and its synthesis may be inhibited by pro-inflammatory mediators such as interleukin-1, interleukin-6, and tumor necrosis factor-alpha during the inflammatory response. 29 Therefore, the level of ALB reflects, to a certain degree, the inflammatory status of the organism. In recent years, composite scoring systems that integrate multidimensional information on inflammation and nutritional status, such as the Prognostic Nutritional Index (PNI) and the Naples Prognostic Score (NPS), have demonstrated superior predictive value by providing a more comprehensive reflection of the patient's pathophysiological state. It is noteworthy that serum albumin is a common core component of these scores, and the predictive utility of PNI and NPS has extended beyond oncology into cardiovascular emergencies. For instance, PNI has been established as an independent predictor of survival in patients with pulmonary embolism. 30 Similarly, NPS has been validated to effectively predict long-term mortality in both patients with pulmonary embolism and STEMI patients undergoing primary percutaneous coronary intervention.31–32 In patients with ACS, studies have shown that ALB levels are negatively correlated with high-sensitivity C-reactive protein (hsCRP) and white blood cell (WBC) counts. And it has been identified as an independent predictor of heart failure events (adjusted HR: 2.31, 95%CI: 1.87-2.84) and in-hospital mortality risk (adjusted HR: 1.88, 95% CI: 1.23-2.86). Furthermore, it is speculated that systemic inflammation may be an underlying mechanism contributing to hypoalbuminemia in this clinical context. 33 Our study showed that there was significantly difference in WBC and ALB values at admission of patients with SR and NSR (P = 0.034 and 0.030). Moreover, WBC and ALB were identified as a hazardous and a protective factor, respectively, for NSR (OR = 1.065, 95%CI: 1.001-1.133 for WBC and OR = 0.942, 95%CI: 0.891-0.995 for ALB). These findings suggest that diminished anti-inflammatory capacity, reflected by hypoalbuminemia, may reduce the likelihood of IRA-SR in patients with STEMI.
Based on previous research findings and existing hypothetical mechanisms, we have become interested in evaluating whether RAR can predict SR. Firstly, compared to endothelin-1, homocysteine and apelin previously reported, both RDW and ALB are routine components of blood tests and biochemical assays. They require no additional examinations, making RAR a simpler, faster, and more economical indicator that could facilitate broader clinical application. Secondly, there is no doubt that RAR is correlated with the severity and prognosis of AMI. Jian L et al. reported that RAR may be a potential biomarker of AMI, which is an independent risk factor for in-hospital all-cause mortality in intensive care unit (ICU) patients with AMI. 34 Besides, Li H's study suggested that the RAR level may be a better predictor of 90-day mortality in AMI patients than ether albumin or RDW alone. 35 Remarkably, our study indicated that in patients with STEMI accompanied by IRA-SR, the admission RAR levels were significantly lower than those in patients with NSR. Furthermore, RAR values were negatively correlated with TIMI flow grades and Gensini scores. Multivariate analysis adjusted for sex, age, WBC, ApoA1, ALB and LVEF identified a high RAR level as an independent risk factor of NSR in STAMI patients (OR = 2.528, 95%CI: 1.019-6.276). In addition, the AUC for RAR in predicting SR was 0.613 (95%CI: 0.552–0.675), which was significantly larger than that of ALB or RDW alone, suggesting that the RAR level may have a better predicting performance of SR in STAMI patients compared to individual biomarkers.
Nevertheless, this study does have several limitations that should be considered when interpreting our findings. Firstly, this was a single-centre, small-sample-size retrospective cohort study, thus the findings may reflect correlation rather than causation and cause an inevitable selection bias. A larger cohort research would strengthen our ability to validate the predictive value of the RAR for SR in STAMI. Secondly, the analysis did not include survival predictive factors, meaning we cannot ascertain how effective the RAR is in predicting long-term outcomes in patients who experience SR. Thirdly, generally speaking, the value of combined diagnostics is superior to that of single-index. We attempted to enhance the predictive power for SR by combining RAR with potential independent risk factors such as WBC and ApoA1, found that the combined diagnostic ability of the three was better than RAR, but without statistical significance. Seeking a new marker to combine with RAR may be a direction for the continued progress of the research. Fourthly, despite adjusting for a comprehensive set of clinically relevant variables in Model C, the potential for residual confounding persists by unmeasured factors such as medication adherence prior to admission and body mass index (BMI) were not available in our dataset. Most importantly, given its modest predictive accuracy (AUC value of 0.613), its clinical utility may not lie in being a sole decision-making tool, but rather as a component within a comprehensive predictive model that incorporates other clinical, echocardiographic, or laboratory parameters. Future research should focus on developing such integrated models to improve predictive performance.
Conclusion
In summary, this study indicates that in patients with acute STEMI, TIMI grade before PPCI is associated with RAR levels, and it may be an independent risk factor for IRA-NSR. The RAR value of 3.201 are expected to become a promising biomarker for predicting SR in patients with acute STEMI.
Footnotes
Abbreviations
Acknowledgements
Not applicable.
ORCID iDs
Author Contributions
HFM and YW have made substantial contributions to conception and design of the study. LXR wrote the manuscript. ZZM, LZQ, XJM, RWZ, ZRG, WJF, LQ and HDY contributed to acquisition, analysis, and interpretation of data. GCL, LHB, HBB, LYX, XJH, YHX and FJM contributed to statistical analysis. HFM and YW critically reviewed, edited and approved the manuscript. All authors have read and approved the manuscript.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of the Fujian Medical University Affiliated Mindong Hospital[Ethical Approval No.: 2021120202 K] and was in accordance with standards set forth by the Declaration of Helsinki. All participants provided their written informed consent before officially entering in the study.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Fujian Province, (grant number 2022J011523).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.